
Abstract
SUMMARY: Gas gangrene is a severe form of gangrene (tissue death) that usually is caused by Clostridium perfringens. It generally occurs at the site of trauma or a recent surgical wound. We report the case of a 45-year-old woman with sphenoid-ridged meningioma who received preoperative transarterial embolization with polyvinyl alcohol. The patient later developed an intratumoral C perfringens infection and died despite intensive medical care. The case represents an extremely rare complication following transarterial embolization of meningioma.
Preoperative embolization of meningiomas is considered valuable to allow simpler resection by reducing intraoperative blood loss and decreasing surgery time. Though the embolization procedures are quite safe with careful techniques in our general practice,1 reports of some rare complications—such as tumoral and subarachnoid hemorrhage, scalp necrosis, retinal embolus, facial nerve palsies, and occlusion of the vasa nervorum of cranial nerves—have been published. We now report what is, to the best of our knowledge, the first case of gas gangrene due to Clostridium perfringens infection after preoperative embolization of a meningioma. We also propose that prophylactic antibiotics should be used in meningioma embolization to avoid this complication.
Case Report
A 45-year-old woman with complaints of intermittent headache, nausea, dizziness, and progressive loss of visual acuity during a 5-year period was admitted to our emergency department because of aggravation of these symptoms. A cerebral MR imaging study revealed a large meningioma, about 5.5 cm × 5 cm × 5 cm in size, at the right sphenoid ridge. The tumor was accompanied with perifocal edema and subfalcine herniation. Because of the neovascularity of the tumor and its large size, preoperative embolization was planned. Cerebral angiography showed a large hypervascular tumor mainly fed by branches of the right middle meningeal artery. Thereafter, selective embolization of the right middle meningeal artery using coaxial microcatheter systems and standard technique was performed. The embolization was performed by using one bottle of 50–100-μ polyvinyl alcohol (PVA) particles (Ultra-Drivalon; CathNet-Science, Paris, France) followed by half a bottle of 150–250-μ PVA particles. A postembolization arteriogram showed a significant decrease in tumor vascularity. The patient then returned to the ward in stable condition. Unfortunately, the patient developed a high fever (≤39.3°C) about 1.5 days after the embolization procedure. The patient complained of a persistent headache despite analgesics and mannitol infusion. About 48 hours after the embolization procedure, the patient suddenly lost consciousness with ipsilateral pupil dilation. An emergency brain CT study showed tumor necrosis with gas formation inside and around the tumor (Fig 1). There was associated severe brain edema with subfalcine and right uncal herniation. Surgical decompression with subtotal tumor removal was immediately performed. Histopathology of the tumor showed marked necrosis with residual meningioma and gas bubble formation. Gram-positive organisms were found (Fig 2). Later, both tissue and blood culture yielded C perfringens. Because of irreversible brain stem dysfunction, this patient died 16 days after the onset of uncal herniation, despite intensive management.

Unenhanced axial brain CT image taken about 2 days after the preoperative meningioma embolization showed tumor necrosis with gas formation inside and around the tumor.
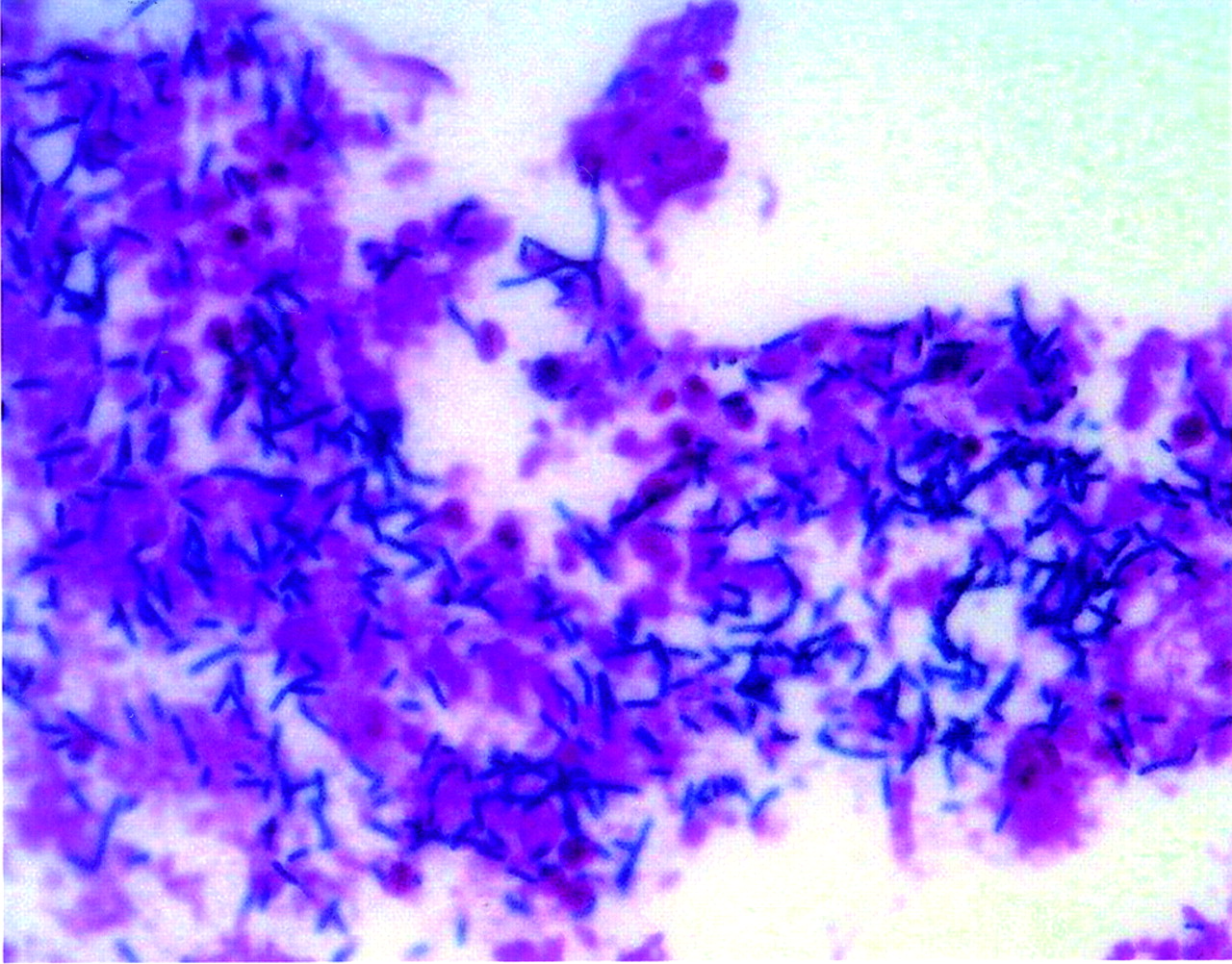
Gram stain (×400) of the specimen from the tumor shows numerous Gram-positive bacilli consistent with C perfringens.
Review of the patient’s history revealed no obvious symptoms or signs of infection in the upper respiratory tract, gastrointestinal tract, or urinary tract before admission.
Discussion
The goal of preoperative meningioma embolization is safer and more successful surgical procedures by reducing operating time and blood loss. Toward this end, the surgeon should plan the procedure to minimize risks. This procedure is safe and effective,1 with complication rates ranging from 1.6%2 to 3%.3 Anecdotal reports of complications include tumoral and subarachnoid hemorrhage, scalp necrosis, retinal emboli, facial nerve palsies, and occlusion of the vasa nervorum of cranial nerves. To the best of our knowledge, postembolization C perfringens infection has not been reported. Indeed, C perfringens is a rare cause of CNS infection, usually occurring as a complication of penetrating trauma. For example, neurosurgical procedures were reported in 9 cases: 2 were due to intraoperative contamination4,5; 2 had entry portals due to surgical drain and intra-abdominal infection6,7; and 5 had no precise source of infection.8-12 Six of the 9 died of meningitis, and one died of brain abscess.
Spontaneous gas gangrene without external wound or injury occurs frequently in patients who have serious underlying conditions, such as vascular disease (atherosclerosis), diabetes, or colorectal or hematologic malignancy. In our patient, infection might have been due to contamination during the procedure or to hematogenous spread from respiratory gastrointestinal or genitourinary tracts. It was not due to PVA particles, because no bacterial growth was found when PVA was put into anaerobic culture.
The course of infection is variable, depending on host immunity and various toxins produced by C perfringens, such as epsilon toxin, which is thought to damage the blood-brain barrier. C perfringens is a Gram-positive, gas-forming, sporing commensal bacterium of the colon and vagina. It grows only in mechanically or chemically damaged tissues. In one study,13 extended microembolization with 50–150-μ PVA particles caused significant tumor necrosis seen on MR imaging and histopathologic examination after surgery, as compared with larger particle embolization. The authors concluded that extended microembolization with small PVA particles improved surgical treatment of meningiomas. We had performed about 100 cases of meningioma embolization with 150–250 μ PVA particles without major complications. This was the first in which we extended microembolization with small PVA particles. The devascularization of the tumor with subsequent tumoral ischemia and necrosis may have provided an anaerobic environment for the growth of C perfringens. Whether embolization with small particles increased the risk of C perfringens infection is unclear, because no other cases were reported.
We conclude that this rare complication of preoperative meningioma embolization should be kept in mind in the differential diagnosis of postembolization fever. C perfringens infection remains fatal despite frequent, prompt, and aggressive treatment.
References
- Received May 1, 2005.
- Accepted after revision August 14, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.