
Abstract
SUMMARY: A patient with hypopharyngeal cancer developed carotid blowout syndrome (CBS) treated by self-expandable stent-graft in the left carotid artery. CT scan for progressive right hemiparesis 4 months later showed multiple left cerebral abscesses and left carotid thrombosis. Although deployment of stent-grafts for CBS can achieve initial hemostasis in patients with head-and-neck cancer, the placement of a stent-graft in a field of necrosis and infection is associated with poor long-term outcome. We recommend the use of prophylactic antibiotics if endovascular foreign materials are placed in a contaminated field.
Carotid blowout is increasingly recognized as a devastating complication associated with radical head-and-neck surgery. For management of carotid blowout, endovascular therapy (eg, permanent balloon occlusion or reconstruction with stents) is reported as an excellent alternative to surgery.1-3 In addition, endovascular reconstruction with stent-grafts shows promise for patients with carotid blowout syndrome (CBS) at risk of cerebral ischemia.4 Some reports, however, have noted poor long-term outcome of stent-grafts for treatment of lesions in a field marked by radiation necrosis with infection.5,6 To the best of our knowledge, brain abscess formation in association with a patient with CBS treated by self-expandable stent-graft has not been reported.
Case Report
A 52-year-old man was diagnosed with stage T4 N2 M0 hypopharyngeal cancer 1 year before presentation to us. CT of neck showed the tumor was in the left supraglottic region, and pathologic examination revealed a squamous cell carcinoma. The patient received concurrent chemoradiotherapy (total dose to larynx and neck region, 7200 cGy). Follow-up laryngoscopy 6 months after treatment showed only necrotic tissue, and biopsy revealed necrosis and inflammation.
The patient was admitted to our hospital after presenting with massive bleeding from the mouth. Physical examination showed swollen and rigid soft tissue in the left neck due to previous irradiation. On the basis of the impression of impending CBS, a CT scan of the neck was performed, revealing an area of necrosis in the left pyriform sinus near the left carotid bifurcation (Fig 1). Another episode of active bleeding from the mouth occurred, and emergent angiography showed a pseudoaneurysm in the left carotid bifurcation (Fig 2A). Because of extensive radiation change in the soft tissue of the left neck region, we embolized the main trunk and proximal branches of the left external carotid artery with 3 fiber coils to avoid reconstitution of collaterals from the contralateral external carotid artery or ipsilateral thyrocervical trunks to branches of the left external carotid artery, followed by deployment of a self-expandible stent-graft of 8 × 50 mm (Wallgraft, Boston Scientific, Natick, Mass) from the left proximal internal carotid artery to the common carotid artery (Fig 2B). Active extravasation stopped immediately. We maintained conservative treatment for the irradiation change in the left neck region. The patient was discharged in stable condition.

Axial CT of the neck with contrast medium shows slightly irregular axial contour of the left carotid bifurcation (arrow). An area of necrosis with gas bubbles is seen in the left pyriform sinus (arrowhead), adjacent to the left carotid artery.

Selective angiograms of the left carotid artery, with a lateral view. A, A pseudoaneurysm in the right distal common carotid artery is noted (arrow). B, A self-expandable Wallgraft stent is deployed from the right internal carotid artery to right common carotid artery. Three fiber coils in the main trunk and proximal branches of the left external carotid artery are also found (arrowheads).
Four months after the interventional procedure, the patient was sent to a local hospital because of progressive right hemiparesis and fever of 3 days’ duration. He was diagnosed with brain abscesses, and antibiotic therapy was initiated. Blood cultures showed no growth of bacteria. CSF examination revealed numerous polymorphonuclear cells. He was then transferred to our hospital. Radiation necrosis of the soft tissue of the left neck was found. Laboratory tests showed a white blood cell count of 11,900/mm3 (segmented granulocytes, 80%). CT scan showed multiple abscesses in the left cerebral hemisphere just within the junctional territory of the left anterior cerebral artery and left middle cerebral artery (Fig 3A). CT scan of the neck showed thrombosis of the left internal carotid artery with gas collection within the stent-graft (Fig 3B). The stent was extruded and exposed to the hypopharyngeal wall (Fig 3B). Thrombosis of the left common carotid artery was also found (Fig 3C). The abscesses coalesced after intensive antibiotic treatment for 2 months, so surgical drainage was performed. The patient was discharged with only slight right hemiparesis.
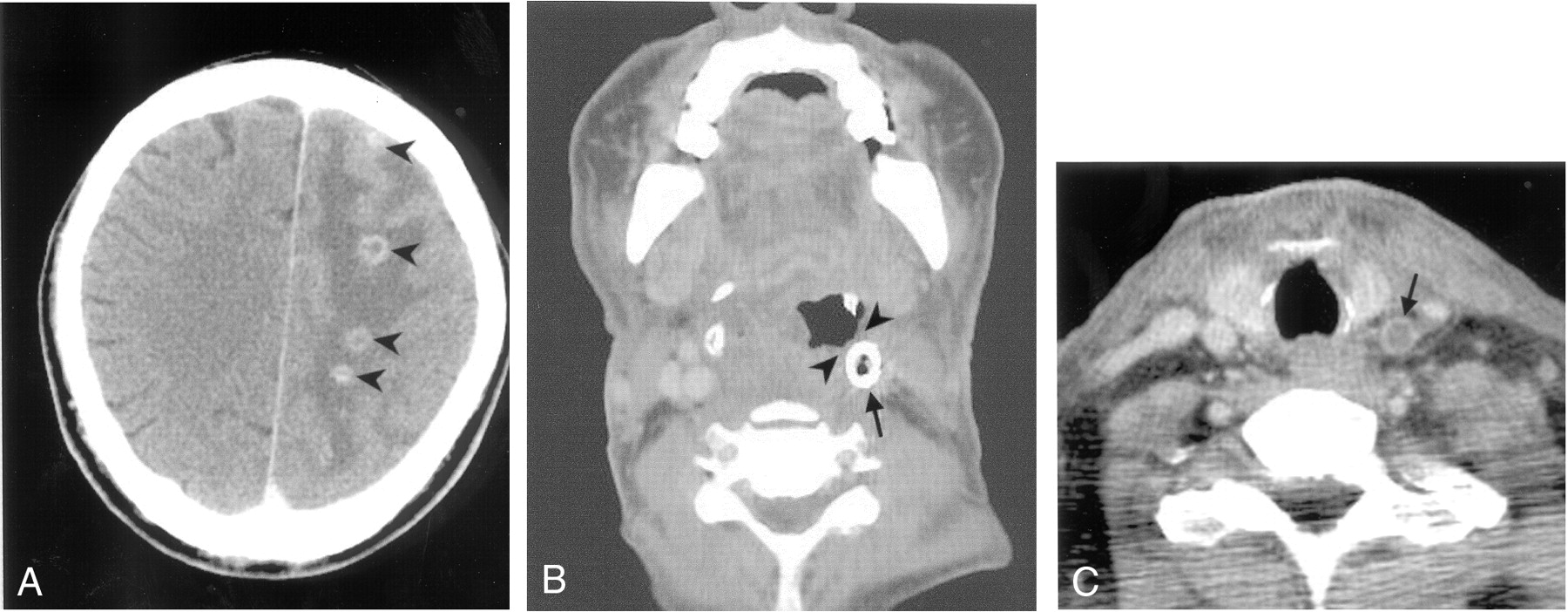
Axial CT scans of the brain and neck performed with contrast medium. A, Multiple brain abscesses are noted in the left centrum semiovale and the left high frontal region (arrowheads), in the junctional zone of the left anterior and middle cerebral arteries. B, Thrombosis with gas collection within the stent-graft is found in the left carotid artery (arrow). The stent has been extruded and exposed to the hypopharyngeal wall (arrowheads). C, Thrombosis of the left common carotid artery proximal to the stent is found (arrow).
Discussion
Carotid blowout is a feared complication of head-and-neck cancer surgery. Surgical management of carotid blowout is usually technically difficult in the previously irradiated field.1 Endovascular techniques have proved very efficient in arresting hemorrhage and have substantially improved outcomes.1,3 For reconstructive management, endovascular stents have been used to treat carotid blowout with preservation of the parent artery.3-6 In one series of 12 patients, CBS was safely managed with stent-assisted endovascular reconstruction without any instances of procedure-related stroke or death.4 These findings suggest that self-expandable stent-grafts may be promising in management of carotid blowout.
For management of carotid blowout with stent-grafts in patients with head-and-neck cancers, the validity of such results is limited by the duration of follow-up. In 2 studies, deployment of self-expandable stent-grafts for CBS in a field with ongoing radiation necrosis and contamination caused thrombosis of the carotid artery or r-bleeding due to the presence of the stent-grafts as a potential nidus for infection.5,6 The use of foreign material in a field with contaminated necrosis may result in localization and persistence of infection as a result of colonization of the foreign material by infective organisms. Persistent infection of a foreign body may also inhibit neointimal formation inside the stent and growth of vascular soft tissue surrounding the stent, both of which ultimately cause thrombosis of the carotid artery. With our patient, deployment of a self-expandable stent-graft achieved initial hemostasis but only short-term preservation of the carotid artery. Septic thrombosis of the carotid artery and stent in a field with contaminated necrosis acts as a source of septic emboli, which cause multiple brain abscesses. This sequence of events favors the conclusion that the stent-graft has a role limited to initial and temporary hemostasis in management of CBS in patients with head-and-neck cancer complicated by necrosis and infection.
Intracranial infection following endovascular therapy for cerebrovascular disease is a rare complication. There are 5 reported cases of cerebral abscess following endovascular therapy in the literature through 2002.7 Infection of peripheral endovascular stents is also rare, but it can have serious consequences.8 These authors have emphasized the need to take extreme precaution in ensuring good aseptic technique during a foreign-body deployment. Because of the risk of infection of endovascular stents in a field with contaminated necrosis, antibiotic prophylaxis was suggested during and after stent deployment in a swine model study.9 Because many postoperative wound infections of head and neck surgery are polymicrobial, antibiotic prophylaxis should target Gram-positive, Gram-negative, and anaerobic organisms. In a study of 212 evaluable patients, the sulbactam-ampicillin is clinically more effective than clindamycin for the prophylaxis of wound infection.10 With our patient, the stent-graft was placed inevitably in a carotid artery in a contaminated field. Because antibiotics were not used during or after the procedure in our case, the stent could be a factor for persistent local infection and septic thrombosis of the left carotid artery for the 4 months after procedural management. This suggests the use of prophylactic antibiotics is wise if endovascular foreign materials are placed in a contaminated field.
Conclusion
Deployment of self-expandable stent-grafts in a field with contaminated necrosis as part of management of CBS is not a safe way to achieve enduring hemostasis in patients with head-and-neck cancer. Stent placement may be complicated by septic thrombosis of the carotid artery and brain abscess formation. Prophylactic antibiotics are recommended in these patients.
References
- Received August 14, 2005.
- Accepted after revision September 10, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}