
Abstract
SUMMARY: Although transcutaneous ultrasound combined with fine-needle aspiration is often used as initial modality for evaluating superficial neck masses, its role in management of deep-seated neck masses is limited. Intraoral ultrasound and guided biopsy helps in obtaining tissue from deep-seated neck masses for an accurate histologic diagnosis, providing useful information in treatment planning. This article discusses the role of intraoral ultrasound and presents 3 cases in which biopsy of deep-seated neck masses under intraoral ultrasound guidance helped in diagnosis and management.
Sonography supplemented by fine-needle aspiration cytology (FNAC) is the initial imaging technique of choice for most superficial head and neck lesions. It is well accepted that deep-seated lesions such as those within retropharyngeal space, parapharyngeal space, and deep portions of parotid space cannot be fully evaluated by transcutaneous sonography. However, large portions of these lesions can be adequately visualized by intraoral sonography and therefore are amenable to a sonography-guided biopsy or FNAC. We present 3 cases to illustrate the role of intraoral sonography for guidance of biopsy in deep-seated head and neck lesions.
Case Reports
Case 1
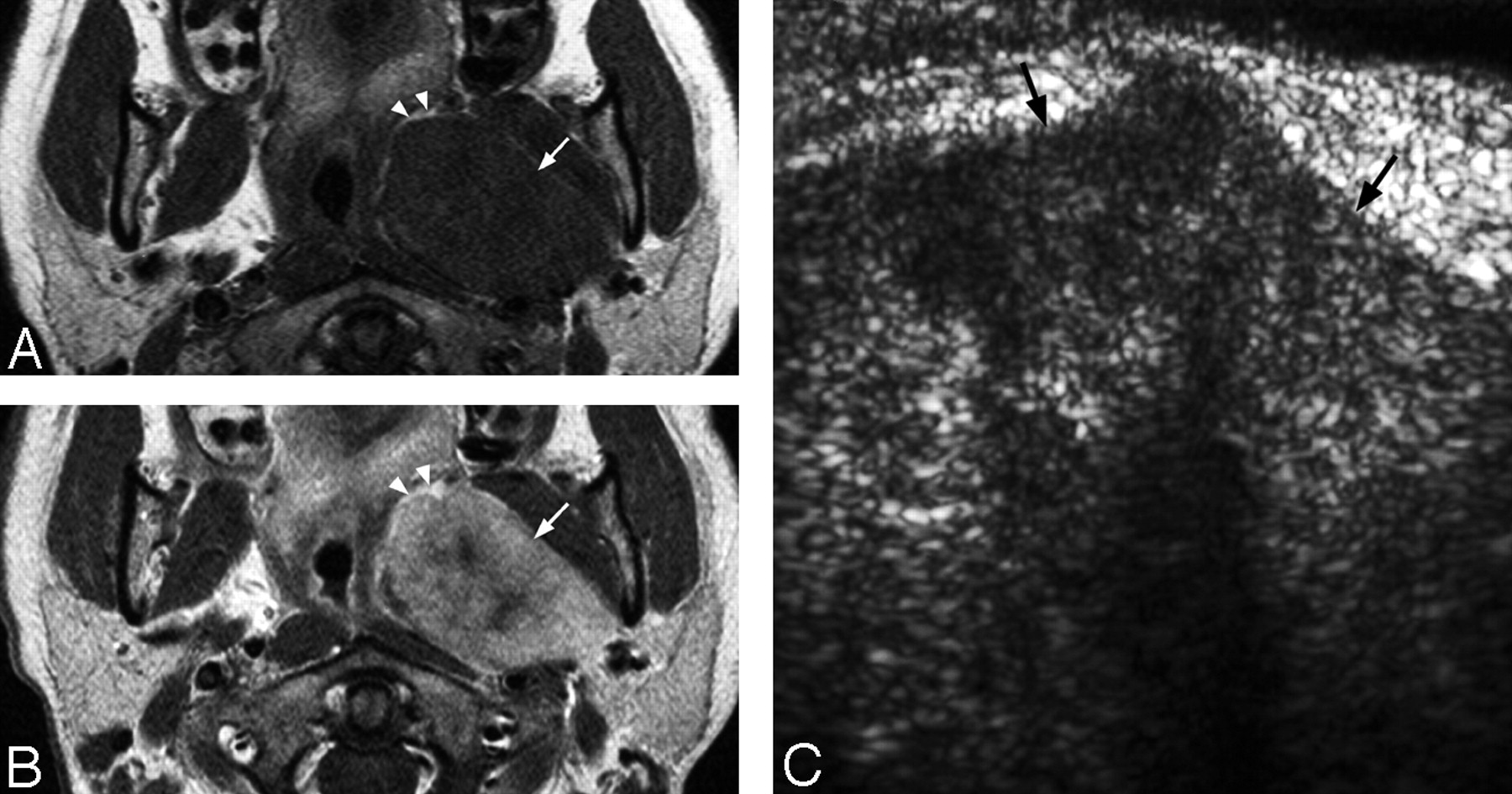
A 63-year-old man, treated for nasopharyngeal carcinoma with combined chemotherapy and radiation therapy 3 years before presentation, was found to have local tumor recurrence at the left lateral wall of the nasopharynx. MR imaging performed (1.5T Gyroscan ACS-NT; Philips Medical System, Best, the Netherlands) for staging of the recurrent disease revealed an enlarged (12 mm in short-axis diameter) left retropharyngeal lymph node at the level of oropharynx located just medial to the left internal carotid artery (Fig 1A). The PET finding was equivocal. To plan further surgical treatment, it was important to determine the nature of the enlarged retropharyngeal lymph node. If it proved to be a metastatic node closely related to the internal carotid artery, complete tumor resection might not be possible.

A 63-year-old man with metastatic left retropharyngeal node from recurrent nasopharyngeal carcinoma.
A, Postgadolinium enhanced, fat-suppressed T1-weighted (repetition time, 550 ms/echo time, 12 ms/number of signal averages, 2) axial MR image at the level of oropharynx shows an enlarged left retropharyngeal lymph node (arrow). Note the close relationship of the lymph node with the left internal carotid artery (arrowhead).
B, Grayscale intraoral sonography in transverse plane reveals a well-defined, solid, round, hypoechoic left retropharyngeal lymph node (arrow) just medial to the left internal carotid artery (arrowhead). The sonographic appearances are suggestive of a malignant node.
Therefore, an intraoral sonography-guided biopsy was performed with a 10-MHz small linear array transducer (Advanced Technology Laboratory, Philips Sonography, Bothell, Wash). On intraoral sonography, the enlarged left retropharyngeal lymph node was identified medial to the left internal carotid artery (Fig 1B); it was solid and round with homogeneous, hypoechoic echotexture. Overall features were suggestive of metastatic lymph node. Biopsy was then performed with the use of a 22-gauge Franseen needle (Medical Device Technologies, Gainesville, Fla) under intraoral sonography guidance. Histologic examination confirmed the node to be metastatic, undifferentiated, carcinoma from primary nasopharyngeal carcinoma. In situ hybridization of the tumor for Epstein-Barr virus–encoded small nuclear RNA was positive. The procedure was uneventful, and the patient was discharged the following day after overnight clinical observation. In view of the histologic result, salvage surgery was not contemplated and palliative chemotherapy was planned.
Case 2
An 82-year-old woman presented with an incidental finding of painless swelling of the right oropharyngeal wall. On physical examination, there was a smooth bulge in the contour of the right oropharyngeal and nasopharyngeal walls. The right tonsil was displaced toward the left. There was no sign of cranial nerve palsy or any palpable neck mass on detailed clinical examination.
MR imaging (1.5T Gyroscan ACS-NT; Philips Medical Systems) showed a large well-circumscribed lesion centered in the right parapharyngeal space (Fig 2A). It was heterogeneous with both cystic and enhancing solid components. The differential diagnoses included accessory salivary gland neoplasm, nerve sheath tumor with cystic degeneration, or large necrotic metastatic cervical lymph node.

An 82-year-old woman with peripheral nerve sheath tumor in the right parapharyngeal space.
A, Postgadolinium T1-weighted (repetition time, 425 ms/echo time, 13 ms/number of signal averages, 2) axial MR image shows a well-circumscribed heterogeneous mass with both cystic and solid enhancing components in the right parapharyngeal space (arrows). The right lateral oropharyngeal wall is pushed toward the midline.
B, Grayscale intraoral sonography in transverse plane confirms the presence of heterogeneous mixed cystic and solid mass (arrows) underneath the right oropharyngeal mucosa.
Intraoral sonography (10-MHz small linear transducer; Advanced Technology Laboratory, Philips Sonography) revealed a mixed cystic and solid mass underneath the right oropharyngeal mucosal surface (Fig 2B). Biopsy was then performed with the use of a 22-gauge Franseen needle under sonography guidance. The histologic features were those of a spindle-cell neoplasm favoring a peripheral nerve sheath tumor. The procedure was uneventful, and the patient was discharged after overnight clinical observation. In view of the histologic result, surgery was recommended; however, the patient refused and preferred regular follow-up because the mass was otherwise asymptomatic.
Case 3
A 40-year-old woman presented with painless left tonsillar swelling of 6 months’ duration. On physical examination, there was a smooth focal bulge over the left lateral pharyngeal wall, and the left tonsil was pushed toward the midline. The overlying mucosa was intact. No palpable parotid mass or enlarged cervical lymph node was detected on clinical examination.
MR imaging examination (1.5T Gyroscan ACS-NT; Philips Medical Systems) revealed a large, well-circumscribed mass centered in the left parotid space displacing the left parapharyngeal fat anteromedially (Fig 3A, -B). The mass was of intermediate signal intensity on T1-weighted sequence with heterogeneous high signal intensity on T2-weighted sequence and heterogeneous enhancement after intravenous gadolinium injection. The differential diagnoses included pleomorphic adenoma or a malignant salivary gland neoplasm.
A 40-year-old woman with a pleomorphic adenoma in the deep left parotid space. T1-weighted (A) and postgadolinium enhanced T1-weighted (B) (repetition time, 450 ms/echo time, 13 ms/number of signal averages, 2) axial MR images show a well-circumscribed heterogeneously enhancing mass (arrows) arising from the left parotid space. Note that the left parapharyngeal fat is displaced anteromedially (arrowheads), which suggests parotid space origin of the mass.
C, Grayscale intraoral sonography in the transverse plane shows a well-circumscribed, homogenous, hypoechoic left deep parotid space mass (arrows) underneath the left oropharyngeal mucosa. Note the deep portion of the lesion is not fully examined by this technique.
Intraoral sonography (10-MHz small linear transducer; Advanced Technology Laboratory, Philips Sonography) confirmed the presence of large homogeneous hypoechoic mass underneath the oropharyngeal mucosa (Fig 3C), and sonography-guided biopsy was then performed with the use of a 22-gauge Franseen needle. The histologic diagnosis was pleomorphic adenoma. The procedure was uneventful, and the patient was discharged after overnight clinical observation. In view of the histologic results and because the mass was otherwise asymptomatic, the patient opted for conservative management with regular follow-up.
Discussion
Although readily available, intraoral sonography is less commonly used than transcutaneous sonography in assessment of head and neck lesions. The reasons include (1) the relatively large size of the commercially available transducer, (2) trismus associated with acute conditions limit patients’ ability to open the mouth, and (3) the small area within the mouth and presence of gag reflex make the examination uncomfortable for the patients.
With the availability of smaller transducers and the use of intraoral local anesthetic spray, the use of intraoral sonography has been increasing. It is a well-tolerated, noninvasive, and accurate technique to differentiate peritonsillar abscess from peritonsillar cellulitis in clinically equivocal cases.1 In addition to its diagnostic role, it serves as imaging guidance for intraoral needle aspiration and can be used to monitor patients’ response after treatment.1–3 Apart from its established role in the management of peritonsillar abscess, intraoral sonography is also useful in delineating tumor extent (particularly tumor thickness) of oral cancers,4,5 monitoring serial change of tongue cancer after radical radiation therapy,6 and evaluating parapharyngeal space tumors.7 To the best of our knowledge, the use of intraoral sonography as a tool for imaging-guided biopsy has not been adequately reported in the literature.
Although CT and MR imaging adequately evaluate deep-seated neck masses, there is often an overlap of imaging appearances among the differential diagnoses being considered. Patients often undergo a surgical biopsy with its potential morbidity to provide tissue diagnosis, which helps in planning the treatment options. The use of intraoral sonography for a guided biopsy provides an alternate technique that is safe, easy to perform, obviates the use of general anesthesia, and can be completed in 10 minutes. Apart from a small intraoral transducer, no additional sophisticated equipment is required to be connected to the sonography machines present in almost all radiology departments. One of the major advantages of biopsy under intraoral sonography guidance is its ability to visualize the major neck vessels, preventing inadvertent vascular injury during the procedure.
Some of the technical aspects of intraoral sonography- guided biopsy warrant special emphasis:
The equipment and procedure of intraoral sonography-guided biopsy are illustrated in Fig 4. The lesion is first localized by intraoral sonography via small intraoral transducer with the patient’s mouth widely open. The needle is then placed intraorally and positioned adjacent to the transducer. The mucosa overlying the lesion is punctured and the needle advanced into the lesion under real-time sonography guidance. In all 3 cases of our series, only a single pass of needle puncture was performed, with repeated to-and-fro needle movement executed within the lesion to maximize the diagnostic yield.
To maximize the acoustic transmission of sonography through the air-mucosal interface and to prevent cross-contamination, the transducer should be coated with sterile gel and covered with a thin rubber or latex sheath.
The procedure can be performed with the patient sitting on the examination table with the neck in a neutral position. Patients have found this to be the most comfortable posture in which to maintain a relatively prolonged period of mouth opening.
The application of local anesthetic spray (10% xylocaine spray) helps to reduce the painful sensation upon needle puncture of the oropharyngeal mucosa and gag reflex.
The use of color Doppler helps to localize major adjacent neck vessels and exclude the presence of large vessels along the expected biopsy pathway.
In our short series, the diagnostic yield was adequate in all 3 cases using the fine (22-gauge) end-cutting biopsy needle, and mucosal bleeding from the puncture site was minimal and stopped after manual compression of the oropharyngeal wall by the patient for 1–2 minutes. The procedures were uneventful, and no major postbiopsy complication was encountered in any of the cases. The patients were discharged after overnight inpatient observation. We believe that (1) the procedure can be safely performed on an outpatient basis without the need of hospital admission and (2) this technique can be used in most patients with a deep-seated neck mass close to the mucosal surface of oropharynx, except in patients with severe trismus with their inability to keep their mouths open for a considerable period of time and those with exaggerated gag reflex.

A, Basic equipment for intraoral sonography-guided biopsy: intraoral sonography transducer (i); 22-gauge Franseen needle (ii); 10% xylocaine spray (iii).
B, Photograph shows the procedure of intraoral sonography-guided biopsy.
C, Schematic diagram illustrates the biopsy needle pathway in relation to positions of the intraoral sonography transducer and the lesion. M = mass; N = needle; OM = oropharyngeal mucosa; T = transducer.
The role of CT8,9 and MR imaging10,11 in guided biopsy of deep-seated head and neck lesions has been reported. However, CT requires the use of ionizing radiation (though the dose involved is minimal for limited scanning volume), whereas an open magnet and MR-compatible biopsy needles are mandatory for MR imaging-guided technique, which makes these procedures expensive and unavailable in most parts of the world. Although biopsy of lesions in our series can be approached via trans-parotid, retromaxillary, and sigmoid notch approaches via CT guidance, intraoral sonography-guided biopsy provides an ideal alternative in that it is quick and safe because it is performed under real-time guidance, does not involve ionizing radiation, and does not require expensive equipment.
In summary, we report the successful use of intraoral sonography-guided biopsy for deep-seated neck masses in retropharyngeal space, parapharyngeal space, and deep parotid space. It is a useful, simple, well-tolerated, and minimally invasive biopsy technique with high diagnostic yield for neck masses in suitable anatomic locations.
References
- Received June 16, 2005.
- Accepted after revision September 30, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.