
Abstract
BACKGROUND AND PURPOSE: Hyperintense CSF in the subarachnoid space (SAS) on fluid-attenuated inversion recovery (FLAIR) imaging has been reported in numerous pathologic conditions, including subarachnoid hemorrhage, meningitis, meningeal carcinomatosis, superior sagittal thrombosis, adjacent tumors, status epilepticus, and stroke. It has also been reported in otherwise healthy patients undergoing anesthesia with supplemental oxygen. We present a series of 11 patients with hyperintense CSF signal intensity in the SAS on FLAIR imaging after previous administration of gadolinium chelate.
MATERIALS AND METHODS: Head MR images of patients who had a prior gadolinium-enhanced body, spine, or brain MR imaging and who had increased signal intensity in the SAS on FLAIR images were prospectively and retrospectively reviewed. Correlation was made with the clinical and laboratory findings.
RESULTS: Eight of the 11 patients had negative findings on lumbar punctures. Seven patients had either chronic renal insufficiency or acute renal failure, but the remaining 4 had normal renal function. Nine patients had no other significant intracranial abnormalities, and 2 patients had acute infarcts remote from the CSF hyperintensity. One patient had follow-up studies at 24 and 48 hours, documenting resolution of the CSF hyperintensities.
CONCLUSION: Given the sharp rise in volume of contrast-enhanced MR imaging studies, it is inevitable that some patients will have undergone a contrast-enhanced MR imaging 24–48 hours before an MR imaging of the brain. The neuroradiologist should be aware that previous administration of gadolinium chelate can cause increased signal intensity in the SAS on FLAIR imaging in patients with or without a history of renal insufficiency and without abnormalities known to disrupt the blood-brain barrier.
Fluid-attenuated inversion recovery (FLAIR) is routinely used in brain imaging due to its high lesion-to-tissue contrast from T2 prolongation with nulling of normal CSF background. It is known to be particularly sensitive for pathologic entities that affect the CSF in the subarachnoid space (SAS). Increased signal intensity in the SAS on FLAIR imaging has been described in numerous conditions, including subarachnoid hemorrhage,1,2 meningitis,1,3–5 stroke,1,6–8 meningeal carcinomatosis,9 leptomeningeal metastasis,10 subdural hematoma,11 adjacent neoplasms,1,12 dural venous thrombosis,13 and status epilepticus.14 It has also been described as a diagnostic pitfall in patients undergoing an MR imaging with supplemental oxygen15 and in those patients who have previously received iodinated contrast material.16 It can be seen as a susceptibility artifact if there is adjacent metal. A few case reports have described increased signal intensity in the SAS on FLAIR imaging in patients with renal failure who had previously received gadolinium.17–19 These findings have also been described in vitro and in animal models.20 No reports to date have reported these findings in patients with normal renal function absent intracranial pathology.
Materials and Methods
We retrospectively and prospectively identified patients who underwent MR imaging of the brain and had a prior gadolinium-enhanced body, spine, or brain MR imaging. Patients with increased signal intensity in the SAS on FLAIR imaging were then reviewed. Patient characteristics, including age, renal function, milliliters per kilogram and rate of gadolinium administered, use of supplemental oxygen during the MR imaging, and any associated intracranial pathology, were then correlated with the MR images. Correlation was also made with the patients’ clinical and laboratory findings, including lumbar puncture.
Results
Eleven patients were identified with increased signal intensity in the SAS on FLAIR imaging who had been administered gadolinium between 1 and 6 days before their scanning (Figs 1–3). No patient received supplemental oxygen or was receiving steroids at the time of imaging. One patient had follow-up studies at 24 and 48 hours documenting resolution of the CSF hyperintensities (Fig 4). After the findings were reported, 8 of the 11 patients had lumbar punctures performed emergently and were negative for subarachnoid hemorrhage, infection, or malignant cells. Three patients had mildly elevated protein in their CSF (patients 3, 4, and 6; Table); however, this was not high enough to produce increased signal intensity in the SAS on FLAIR.21

A 74-year-old man with normal renal function who underwent a gadolinium-enhanced MR imaging of the head and MR angiography (MRA) of the neck because of a transient ischemic attack and who had a follow-up head MR imaging the next day. A, Normal MRA findings of the neck. B, Precontrast axial FLAIR image shows no signal intensity in the SAS on the date of the gadolinium administration. C, Repeat noncontrast coronal FLAIR image 24 hours later shows increased signal intensity in the SAS. The patient had an emergent lumbar puncture, which was negative for subarachnoid hemorrhage, infection, or malignant cells.

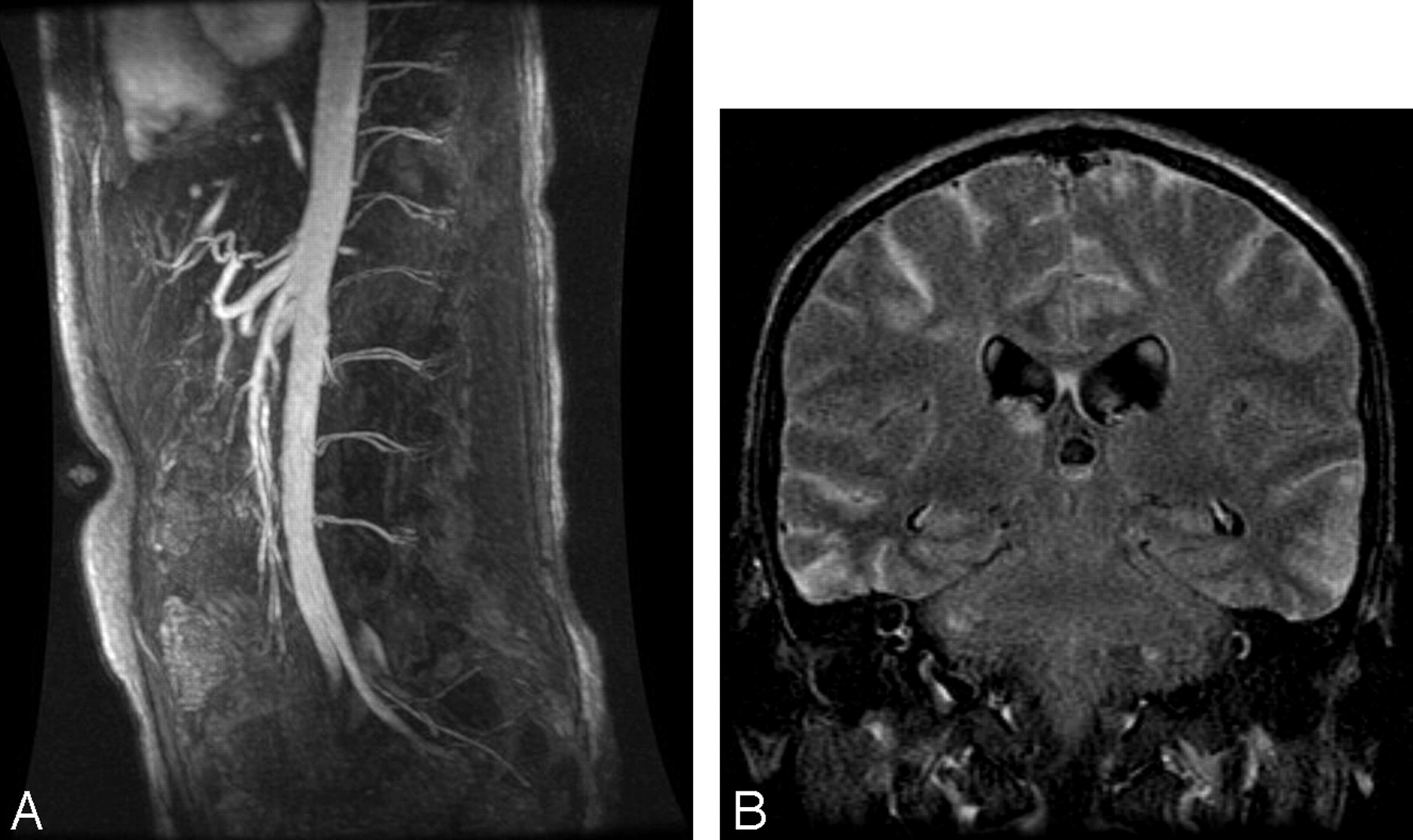
A 21-year-old man with chronic renal insufficiency who underwent gadolinium-enhanced MRA of the abdomen followed by MR imaging of the brain 6 days later to rule out causes of syncope. A, Normal findings on abdominal MRA. B, Precontrast FLAIR image shows diffuse increased signal intensity in the SAS 6 days after the gadolinium injection. The patient had an emergent lumbar puncture, which was as negative for subarachnoid hemorrhage, infection, or malignant cells.
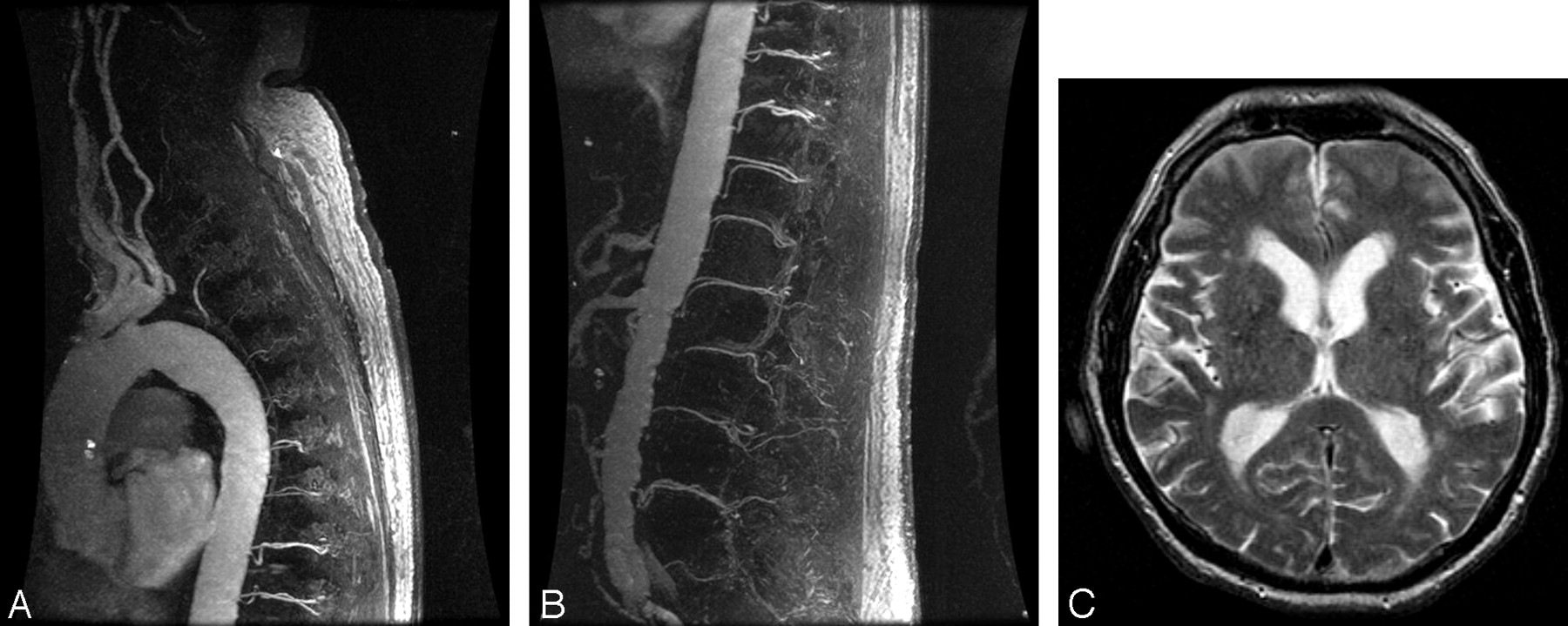
An 81-year-old man with normal renal function who underwent a triple-dose (60 mL) 3D MRA of the spine to exclude a dural arteriovenous fistula, followed by MR imaging of the brain 24 hours later for a syncopal episode. Upper thoracic (A) and thoracolumbar (B) spinal MRA images demonstrate no evidence of a dural arteriovenous fistula. C, Precontrast FLAIR image shows increased signal intensity in the SAS and in the lateral ventricles 24 hours after gadolinium injection. The patient returned to the department and was imaged a second time due to the T2 spin-echo appearance to ensure that there was not a technical error in the initial FLAIR sequence and was found to have similar results.

A 79-year-old man with normal renal function evaluated for a transient ischemic attack. A, Precontrast axial FLAIR image shows no abnormal signal intensity in the SAS. B, Forty-eight hours postgadolinium injection, repeat MR imaging shows diffuse increased signal intensity in the subarachnoid space (SAS) on coronal FLAIR images due to delayed clearance of the gadolinium chelate. C, Repeat MR imaging 72 hours postgadolinium injection shows resolution of the increased signal intensity in the SAS.
Patient characteristics and time interval between gadolinium administration and increased signal in the subarachnoid space on FLAIR
Seven patients had either chronic renal insufficiency or acute renal failure, but the remaining 4 had normal renal function (Table). Nine patients had no other significant intracranial abnormalities seen on MR imaging. Postgadolinium T1-weighted imaging did not show corresponding enhancement in the SAS. Two patients had acute infarcts remote from the hyperintensity seen in the SAS on FLAIR imaging (Fig 3). The age range of the patients was 21–87 years. The rate of gadolinium administered varied between 1 and 2 mL/s, with total doses ranging from 20 to 60 mL/s. The average length of time between gadolinium administration and the increased signal intensity in the SAS seen on FLAIR was 2 days (range, 1–6 days), with the patients with normal renal function at the lower end of the spectrum. One patient had known prostate cancer. No other patient had a known malignancy, and none were found to have leptomeningeal metastasis or carcinomatosis.
Discussion
During the past decade, multiple investigators have shown FLAIR imaging to be sensitive but not specific in demonstrating varied pathologies involving the SAS, such as subarachnoid hemorrhage, meningitis, stroke, meningeal carcinomatosis, leptomeningeal metastasis, subdural hematoma, adjacent neoplasm, dural venous thrombosis, and status epilepticus.1–14 This relies on the fact that FLAIR imaging is designed to null the normal CSF signal intensity, and any alteration in the CSF results in an increased signal intensity in the CSF. Postgadolinium FLAIR imaging has also shown hyperintensity in the SAS in patients with pathologies that are not specific to the SAS but rather disrupt the blood-brain barrier.22,23 Alternatively, increased signal intensity in the SAS can be a diagnostic pitfall in patients receiving supplemental oxygen15 during MR imaging of the brain, in patients with renal insufficiency who have previously received gadolinium,17–19,23,24 and in patients immediately after carotid stent placement.25 Gadolinium has also been reported to diffuse across the choroid plexus and uveochoroid membrane in patients with impaired renal function, resulting in increased signal intensity in the ventricular system and in the vitreous and aqueous humor of the eye on FLAIR imaging.18
This CSF hyperintensity in the SAS and ventricles after prior administration of gadolinium has not been previously reported in patients with normal renal function without intracranial pathology that would otherwise cause a disruption in the blood-brain barrier. To our knowledge, this is the largest series to date of patients with increased signal intensity in the SAS after previous administration of gadolinium.
The direct mechanism by which CSF diffuses into the SAS in patients with or without renal insufficiency is not entirely known. It is postulated that in patients with renal insufficiency, the gadolinium may move across an osmotic gradient at the circumventricular organs in the setting of prolonged elevation of plasma concentrations,18 because it is primarily cleared through glomerular filtration.26
The normal half-life (t ½) of gadolinium chelates is 1.6 hours.26 Although patients with normal serum creatinine levels and renal function should not have prolonged clearance of gadolinium chelates, in those patients with renal insufficiency (glomerular filtration rate [GFR] <20 mL/min), the t ½ can increase up to 30 hours.27 Although the reported rate of gadolinium neurotoxicity in patients with renal insufficiency is <1%,28 this may, in fact, be higher than previously thought. It has been reported that the clinical correlation of increased signal intensity in the SAS on FLAIR imaging in patients with renal insufficiency also appears not to be associated with clinical neurotoxicity.11 This is likely not the case, given the reports of gadolinium-induced nephrogenic fibrosing dermopathy (NFD)29 and gadolinium-induced encephalopathy.19 For these very reasons, in our institution, we have recently instituted withholding gadolinium in patients with a GFR of less than 15 mL/min.
Conclusion
Given the sharp rise in volume of contrast-enhanced MR imaging studies, it is inevitable that some patients will have undergone contrast-enhanced MR imaging 24–48 hours before MR imaging of the brain. The neuroradiologist should be aware that delayed gadolinium chelate clearance can cause increased signal intensity in the SAS on FLAIR imaging in patients with or without a history of renal insufficiency and without abnormalities known to disrupt the blood-brain barrier. Although this represents a diagnostic pitfall, this finding could be clinically relevant in regards to encephalopathy and NFD.
Footnotes
Previously presented at: Annual Meeting of the American Society of Neuroradiology, April-May, 2005; Toronto, Ontario, Canada.
References
- Received January 19, 2007.
- Accepted after revision April 4, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- HARMless: Transient Cortical and Sulcal Hyperintensity on Gadolinium-Enhanced FLAIR after Elective Endovascular Coiling of Intracranial Aneurysms
- Flat Detector Angio-CT following Intra-Arterial Therapy of Acute Ischemic Stroke: Identification of Hemorrhage and Distinction from Contrast Accumulation due to Blood-Brain Barrier Disruption
- Elevated Cerebral Blood Volume Contributes to Increased FLAIR Signal in the Cerebral Sulci of Propofol-Sedated Children
- Isolated Acute Nontraumatic Cortical Subarachnoid Hemorrhage