
Abstract
BACKGROUND AND PURPOSE: Endovascular treatment (EVT) of carotid cavernous fistulas (CCFs) is based on various techniques, mainly those using detachable balloons. Coronary covered stent grafts have been sporadically used in the intracranial arteries and only 2 traumatic CCFs have been reported in the literature; moreover, there is poor information about the long-term follow-up. We present 8 cases of CCFs treated by the placement of a covered stent, 5 of which have a 1-year clinical and angiographic follow-up.
METHODS: Eight patients with posttraumatic CCF were treated by positioning a covered stent in the intracranial internal carotid artery (ICA) to occlude the fistula. They received periodic clinical and angiographic follow-up to evaluate the patency and the stability of clinical results.
RESULTS: In all cases, the symptoms related to the CCF regressed after treatment and did not recur in the follow-up. Two patients presented residual filling of the CCF at the end of the procedure. The angiographic follow-up revealed in 6 patients of 7 a good patency of the ICA; in 1 patient, there was an ICA asymptomatic occlusion. One patient required transvenous coil occlusion of the cavernous sinus.
CONCLUSION: When standard treatments fail, covered stent grafts can be used as a valid alternative in the treatment of CCFs, but more data are needed, especially in the long-term follow-up.
Direct carotid cavernous fistulas (CCFs) are spontaneous or traumatic communication between the internal carotid artery and the cavernous sinus, classified by Barrow et al1 as type A CCFs. Among the various causes are head trauma, surgical trauma, fibromuscular dysplasia, arterial dissection, collagen deficiency syndromes, and rupture of internal carotid artery (ICA) cavernous aneurysms.2–5
Their clinical presentation is related to their size and to the type of venous drainage, which can lead to a variety of symptoms, such as visual loss, proptosis, bruit, chemosis, cranial nerve impairment, intracranial hemorrhage (rare), etc. Direct surgical closure, or ICA surgical ligation, has been now supplanted by endovascular methods, including occlusion of the ostium of the fistula with detachable balloons and transarterial or transvenous catheter coil embolization. Sacrifice of the ICA has been required in certain instances.5–8 In our institution, balloon occlusion of the fistula is the technique most commonly used because of a 30-year experience and because of a series of advantages: the balloon is easily flow-guided to the site of the fistula, repeated inflations and deflations of the balloon may help in understanding the underlying anatomy, and it is very cheap. Despite that, the use of detachable balloons at times suffers technical problems, such as early detachment/deflation of the balloon or occasional rupture of the balloon caused by its contact with bone fragments. It can also dilate the ostium of the fistula or the cavernous sinus itself, as in a procedure of balloon angioplasty, possibly causing a delayed recurrence.
In the 8 cases we present, we were unable to obtain a complete and permanent occlusion of the CCF with balloons alone, so we decided to try the placement of an endovascular stent graft before having to occlude the ICA.
Patients and Techniques
Between March 2002 and August 2005, 8 patients (5 male and 3 female, aged 14–70 years) who presented symptoms related to a posttraumatic CCF after severe head trauma were treated by positioning a Jostent coronary stent graft (previously JoMed, Helsingborg, Sweden; now Abbott Vascular, Redwood City, Calif), after failure at occluding the fistula with detachable balloons (Table).
Treatment of CCFs with covered stents and 6-month and 1-year follow-up
Three patients (cases 3, 4, and 6) presented bilateral CCFs, but only 1 CCF in each patient was treated with a covered stent, whereas the second regressed spontaneously in 1 case (case 4) or was occluded with detachable balloons (completely in case 3 and subtotally in case 6).
In all patients, CT and 4-vessel angiography were performed (Fig. 1). A CT scan revealed traumatic cerebral contusions and intracranial hemorrhages in all patients. Various attempts to exclude their CCFs using detachable balloons were unsuccessful because of technical problems and the characteristics of the fistula itself. Before performing a permanent occlusion of the ICA, we decided to try to deploy a covered stent.

Case 3. A and B, lateral right ICA angiograms show the CCF before (A) and after (B) treatment; arrows point to stent extremities.
C, lateral view showing the stent and 4 detachable balloons previously used; 2 balloons partially inflated were used in an attempt to occlude the right CCF, whereas the 2 deflated balloons occluded the left CCF 2 months earlier.
Case 6 required an urgent treatment during the second day after trauma because he had bilateral CCFs causing a large dilation of the basilar venous plexus, compressing the brain stem. He was referred to our center from a different hospital solely for the treatment of the CCF, and he was then transferred back to his hospital at the end of the procedure. A first attempt to occlude both fistulas with detachable balloons obtained partial results, without resolution of the venous dilation. Therefore, we decided to occlude the larger CCF with a covered stent; the treatment required 2 covered stents because of multiple tears in the cavernous ICA, but it was effective in deflating the basilar venous plexus.
All stent-graft placement procedures were performed via a transfemoral approach under general anesthesia. All procedures were performed in a dedicated monoplane or biplane neuroangiography suite Integris Allura (Philips Medical Systems, Best, the Netherlands).
We obtained angiographic series in all CCF patients, injecting the contralateral ICA and a vertebral artery while hand compressing the neck at the injured side, as part of the preliminary study of the lesion. In all cases in this series, there was very good collateral flow, allowing carotid occlusion, if needed.
Systemic heparinization was administrated intravenously at the beginning of the interventional procedure (a bolus of 5000 IU) and was continued for 48 hours with a flow rate of 1000 IU/h.
Guiding catheters (7F or 8F) were placed in the ICA. In all 8 cases, an Excel 14 microcatheter (Boston Scientific, Natick, Mass) was navigated distal to the fistula into a branch of the middle cerebral artery (MCA). The microguidewire was then replaced with a 0.014-inch, 300-cm exchange guidewire HT-BMW (ACS Guidant, Santa Clara, Calif) or Transend ES (Boston Scientific), so that the Jostent coronary stent could reach the rupture site of the ICA. After careful angiographic confirmation of the correct position, the stent was released, inflating slowly up to 8–10 atm. Postdilation was often needed to completely exclude the lesion using a coronary balloon of a larger diameter. At the end of the procedures, the covered stents were correctly apposed to the ICA wall. In all cases, we had periprocedural spasm of the ICA, because of the stiffness of the system, for which no medical treatment was needed.
According to our protocol for covered stent placement in traumatic CCFs, immediately after the procedure, an anticoagulant and a double platelet-inhibiting therapy (ticlopidine or clopidogrel and aspirin) was prescribed. Anticoagulant therapy (heparin 1000 IU/h) was discontinued after 48 hours, whereas ticlopidine (250 mg twice a day) or clopidogrel (75 mg daily) was discontinued after 3 months, and the patients were left on aspirin alone (100–200 mg daily).
All patients were neurologically evaluated by experienced neurologists in the days before their discharge and than periodically during the follow-up.
Results
Final angiograms at the end of the procedure confirmed total exclusion of the fistula and normal patency of the ICA in all patients (Fig 1) except cases 7 and 8; they had very large ICAs, and the covered stents could not occlude the fistulas despite postdilation with coronary balloons, resulting in a minimal residual filling of the cavernous sinus from the ICA.
No thromboembolic complications occurred in any patients. On the day after the procedure, a confirmatory angiogram was performed in all patients; patient 6 had his confirmatory angiogram 6 days later in the other hospital, confirming complete occlusion of the CCF treated with the grafts.
In case 2, on the second-day confirmatory angiography, there was a residual arterial flow into the cavernous sinus. A 5-mm angioplasty balloon was then inflated to 10 atm to further dilate the stent with complete and persistent occlusion of the fistula and related symptoms.
The patient in case 7 underwent a confirmatory angiography 2 months after the covered stent placement because of a persistent flow into the fistula. Stent dilation with 5- and 6-mm angioplasty balloons resulted in only temporary occlusion of the fistula, so we decided to occlude the cavernous sinus by transvenous coil embolization.
Patient 8, on the second-day confirmatory angiography, presented a remaining flow into the fistula that required dilation of the stent with a 5-mm angioplasty balloon with an improved result but incomplete occlusion of the fistula (Fig 2). Two months later, a confirmatory angiography showed a reduction of flow in the fistula, with normalization of eye chemosis and proptosis.
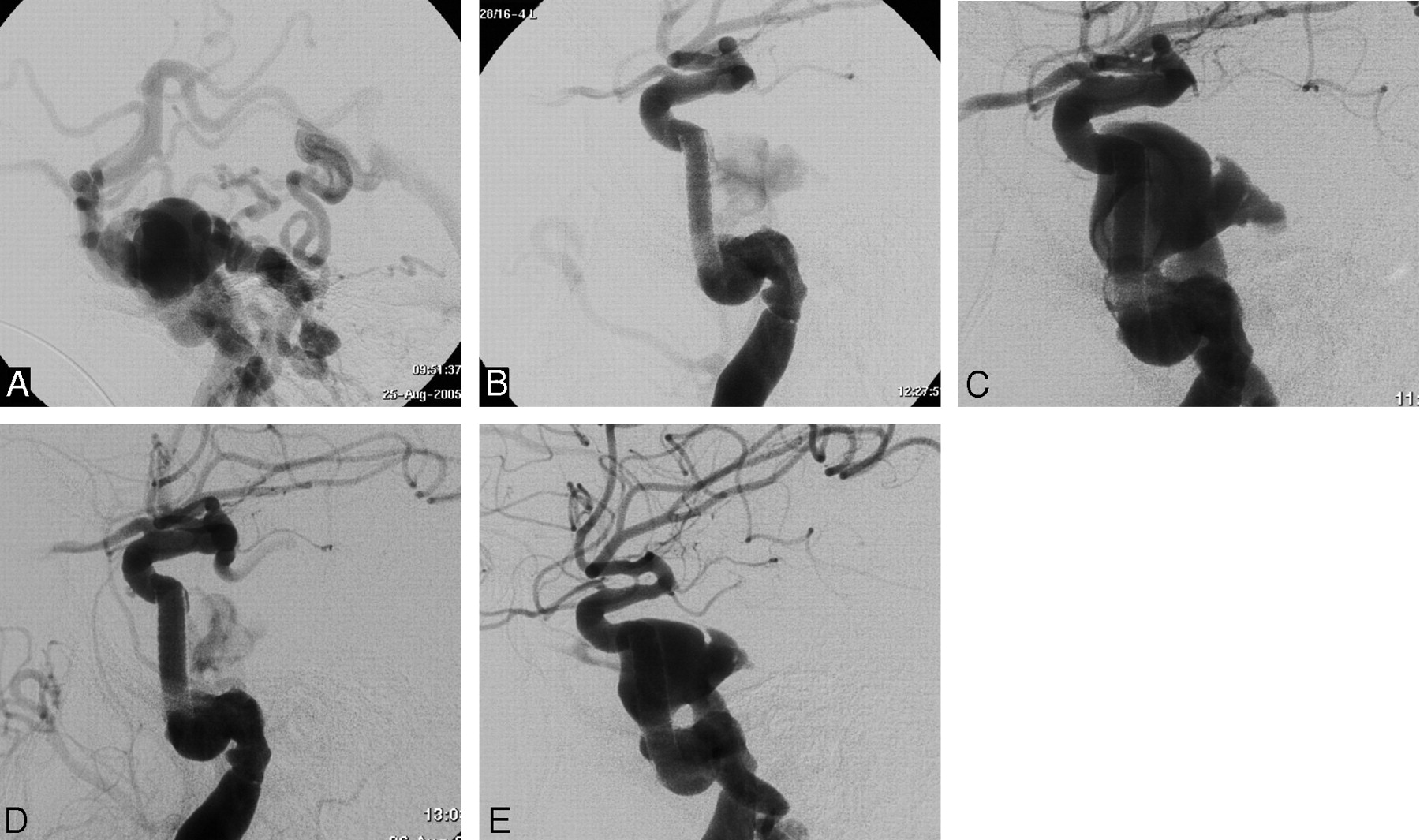
Case 8. A, Lateral angiogram of the ICA showing total steal of the flow toward the cavernous sinus; vertebral and contralateral ICA angiographies (not reported) showed steal also from posterior and contralateral circulation.
B, Lateral ICA angiogram at the end of the stent-graft placement procedure showing nearly complete occlusion of the CCF.
C and D, ICA angiogram in lateral projection of day 2 after treatment showing partial reopening of the fistula (C) and the result after angioplasty with a coronary balloon.
E, Lateral ICA angiogram 3 months later showing persistence of the fistula with regularization of intracranial hemispheric circulation (note different diameter of distal ICA and posterior communicating artery between D and E).
After the procedure, symptoms improved in all patients; CCFs were completely occluded and eventually resolved, with no new symptoms related to possible periprocedural complications. Patient 6 died 2 weeks after the procedure of post-traumatic multiorgan failure. Patient 1 developed an asymptomatic occlusion of the left ICA with optimal collateral blood flow from the contralateral ICA at the 1-month angiographic follow-up.
At the 6-month and 1-year follow-up examinations, there were no changes in the angiographic and neurologic features in the other cases, except an asymptomatic 30% in-stent stenosis caused by intimal hyperplasia in case 5 (Fig 3), which seemed to have improved at the 1-year follow-up. During the follow-up period, no clinical symptoms were related to thromboembolic events caused by the presence of the stent graft.

Case 5. Lateral angiograms show the postprocedural occlusion of the CCF (A) and the intimal hyperplasia causing a 30% reduction of the ICA lumen at the 6-month follow-up (B), with a possible improvement at the 1-year follow-up (C). Arrows point to the stent extremities. The marker of the previously released balloon is visible anterior to the ascending segment of the carotid siphon.
Discussion
Despite the enormous progress in endovascular techniques in the past few decades, the first treatment for CCFs in many centers around the world remains the occlusion of the fistula with detachable balloons.7–14 Transarterial or transvenous coil occlusion of CCFs is also commonly used because many interventional neuroradiologists are more familiar with the use of coils than of detachable balloons and also because balloons are not available everywhere; however, coil treatment is not always safe and effective and has high costs.7, 15, 16
In the past decade, the endoluminal placement of endovascular stent grafts became established as an effective alternative to most surgical repair techniques in the aorta, peripheral and visceral arteries.17–21 Cardiologic covered stents are now commonly used in coronary artery stenosis and bypass ruptures.22, 23 No covered stent is dedicated to intracranial arteries, but there are some sporadic reports that describe the use of coronary covered stents in the neurovascular field.24–35
Stents covered with polytetrafluoroethylene (PTFE) have been used with success in the treatment of pathologic conditions of the coronary arteries because of their low rate of stent-related coronary stenosis and acute stent thrombosis preventing debris protrusion and neointimal proliferation through the stent.36, 37 The main problem in the placement of this type of stent within the ICA is the stiffness of its profile; it is composed of the superposition of 2 stainless steel stents and an ultrathin PTFE layer between them. This rigid configuration does not permit the easy navigation of the stent in the tortuous ICA and can be the cause of periprocedural spasm or dissection. Arterial spasm is a common complication during endovascular procedures, especially when using stiff materials. Other factors in determining vasospasm may be young age and increased arterial reactivity after head injuries. In most cases, the arterial spasm is not clinically relevant, and it resolves spontaneously within a few minutes, but it can also be treated with intra-arterial infusion of nimodipine.
The rigidity of Jostent coronary stent grafts is a well-known limitation of this device among interventional neuroradiologists, but currently no perfect solution for the treatment of CCFs exists. No manufacturer produces covered stents designed or approved for neurovascular use. Cardiovasc Inc (Menlo Park, Calif) has introduced a new coronary stent graft composed of a single steel stent with its extremities folded up to hold the PTFE layer. In our preliminary, unpublished experience with the Cardiovasc Stent Graft, we had the impression of a lower rigidity of the system and an easier progression in the intracranial ICA.
Another important issue with the use of PTFE-covered stents is the short- and long-term patency of the artery. Some reports conclude that PTFE-covered stents reduce the risk of vessel occlusion.22, 23 Although the long-term patency rate of stent grafts in the cerebral arteries remains unknown, some evidence encourages expectation of positive long-term outcome in terms of parent artery patency.30, 33 Moreover, Krings et al38 reported lower in-stent intimal hyperplasia in covered stents than in bare stents in experimentally induced aneurysms. The PTFE layer might reduce the rate of neointimal hyperplasia and stent-related stenosis by inhibiting the migration of inflammatory cells and by attenuating the diffusion of cytokines.35, 36, 39, 40 In contrast, polyethylene terephthalate- and silicone-covered stents have been shown to have poor short-term patency rates because of acute inflammation and exuberant ingrowths of fibrous connective tissue.41–43
When placing covered stent grafts for the treatment of intracranial aneurysms, our anticoagulant and antiplatelet protocol consists of starting double antiplatelet therapy (aspirin and ticlopidine or clopidogrel) 4 days before the procedure and heparin at the beginning of the treatment. Heparin is discontinued 48 hours after the end of the procedure and double antiplatelet is maintained for 2–3 months, followed by aspirin only for 1 year. Similar protocols are used with good results by other authors.30, 33 However in posttraumatic CCFs, we prefer not to start antiplatelet medication before positioning the stent graft because we frequently do a last attempt at occluding the fistula with a detachable balloon during the same session and because a venous drainage through subarachnoid veins is often present with an increased risk of hemorrhage.
We had only 1 case of asymptomatic artery occlusion, in our opinion a result of discontinuation of the antiplatelet therapy. Only 1 case of ICA occlusion after intracranial covered stent placement has been described in the literature so far. Redekop et al35 reported a case of asymptomatic ICA occlusion 1 week after covered stent placement for a posttraumatic petrocavernous ICA pseudoaneurysm. This patient had a distal MCA pseudoaneurysm with high risk of hemorrhage; therefore, after the procedure, heparin therapy was discontinued and single-agent antiplatelet (aspirin 325 mg daily) was initiated.
In case 5, at the 6-month follow-up, we observed an in-stent lumen reduction of 30%, probably due to intimal hyperplasia, that looked improved at the 1-year follow-up and was not responsible for any clinical symptoms. Therefore, we think that an antiplatelet therapy with aspirin and clopidogrel (or ticlopidine) permits good long-term patency results. In-stent stenosis, in intracranial arteries treated with covered stents, has previously been reported in the literature for 2 patients by Islak et al31 and Saatci et al,33 both without any hemodynamic or clinical effect.
In patients 7 and 8, the ICA at the ostium of the CCF exceeded the maximal stent diameter, and there was residual flow between the vessel wall and the stent graft, so we obtained only a slowing of the fistula, not its permanent occlusion. To our knowledge, this is the first report of a similar problem with a covered stent. Moreover, patient 7 required transvenous coil embolization of the cavernous sinus. The largest diameter reached by coronary stent grafts now available is 5 mm; the ICA diameter is usually less than 5 mm, but high-flow, long-standing lesions can widen the ICA. In these situations, endovascular occlusion of CCFs is frequently difficult because large tears of the ICA prevent correct and stable positioning of detachable balloons, and large cavernous sinuses cannot be easily occluded with coils. These CCFs are often treated in various sessions with various devices,7 and stent grafts can be useful in slowing down CCF flow. However larger and self-expandable neurovascular covered stent grafts could be the real solution for high-flow, long-standing CCFs.
Although there are several reports of covered stents used in the intracranial vasculature, only 8 CCFs were reported to be treated with covered stents7, 29, 30, 32, 35; of those, only 2 were posttraumatic.30 Felber et al30 reported the use of a Jostent covered stent in intracranial arteries in 7 patients; of those, 2 had posttraumatic CCFs. For these 2 patients (patients 3 and 4 in their series), they reported the complete occlusion of the fistula without complications and with durable results, respectively, at 14 and 11 months.
We report a series of 8 posttraumatic CCFs treated with covered stents. Our results are in line with those reported in the literature and focus on the anticoagulant and antiplatelet therapy to avoid the in-stent thrombosis. Unfortunately, posttraumatic patients could have a higher risk of hemorrhage, and anticoagulant and antiplatelet therapies might often be contraindicated. On the other hand, CCF symptoms frequently appear not immediately after the trauma but after a few days, when the hemorrhagic risk is decreased. Problems can be encountered in aggressive CCFs that require urgent treatment.
Because of the very small number of reports of posttraumatic CCFs treated with covered stents, larger series are necessary to have more reliable results, while we wait for a stent graft developed for neurovascular use. Our clinical results show good outcome, with no clinical complication; in 2 patients, covered stents did not occlude completely the fistula but slowed down the flow with clinical improvement. Furthermore, with the use of the covered stent, we did not have to overdistend or sacrifice the cavernous sinus, possibly limiting damage to the cranial nerves.
Conclusions
Covered stent grafts can sometimes be used as a valid alternative in the treatment of traumatic CCFs, when more standard treatments fail and the anatomy of the ICA is favorable. We believe that our results and follow-up are encouraging for their further use. This has to be done with caution both because of possible periprocedural complications and because of little understanding of long-term follow-up.
References
- Received September 12, 2005.
- Accepted after revision April 13, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The use of PK Papyrus covered coronary stent for carotid reconstruction: an initial institutional experience
- Use of coronary stent grafts for the treatment of high-flow carotid cavernous fistula
- Recurrence risk factors in detachable balloon embolization of traumatic direct carotid cavernous fistulas in 188 patients
- Combined use of Onyx and coils for transarterial balloon-assisted embolization of traumatic carotid-cavernous fistulas: a report of 16 cases with 17 fistulas
- Use of Onyx for Transarterial Balloon-Assisted Embolization of Traumatic Carotid Cavernous Fistulas: A Report of 23 Cases
- Placement of Covered Stents for the Treatment of Direct Carotid Cavernous Fistulas