
Abstract
SUMMARY: We report 2 cases of traumatic arteriovenous fistulas in the neck treated with transarterial embolization with n-butyl-2-cyanoacrylate (n-BCA). In both cases, covered stent placement across the fistula to preserve the artery was not possible. Detachable coil placement was attempted in one case but was not successful. Both fistulas were successfully treated with n-BCA embolization. To our knowledge, these are the first 2 such cases reported of high-flow cervical arteriovenous fistulas treated with n-BCA embolization.
The spectrum of arterial injury in the setting of penetrating trauma includes dissection, transection, pseudoaneurysm, and traumatic fistula. Traumatic arteriovenous fistulas in the neck present with findings of a thrill or symptoms related to vascular steal phenomenon. The ideal treatment for these lesions is exclusion of the fistula with preservation of the parent vessel. Surgical access can be difficult, and a wide exposure is often needed to obtain proximal and distal control. In addition, access to the vessels at the level of the skull base and of the intraforaminal segment of the vertebral artery is also challenging. As such, endovascular techniques have largely replaced surgical treatments for vertebral artery fistulas,1 and for carotid artery injuries in either zone 1 (below the sternal notch) or zone 3 (above the angle of the mandible).2
The use of covered stents for this application has been described3–5 and is the preferred method when the normal artery distal to the site of the fistula can be safely catheterized. When parent vessel preservation is not possible, endovascular sacrifice of the parent vessel can be performed, and a variety of techniques have been used, including coil embolization, detachable balloons, and covered stent placement.6–8 We present 2 cases of high-output traumatic fistulas in the neck where parent vessel occlusion was performed with the use of the liquid embolic agent N-butyl-2-cyanoacrylate (n-BCA).
Case Reports
Patient 1
A 21-year-old man suffered a close-range gunshot wound to the left neck. He was seen at an outside hospital, where his Glascow Coma Scale score was 7, and he was managed conservatively and discharged to a rehabilitation facility 2 weeks later. At the time of discharge, he had left 7th and 8th cranial nerve palsies because of a temporal bone fracture. Four weeks after the initial event, he had increasing swelling over the left side of the face, and cranial nerve palsies of his left 3rd through 11th nerves. He also developed a large pulsatile mass over the left neck. He was transferred to our facility for further management.
Diagnostic angiography demonstrated 2 arteriovenous fistulas. Because of the extensive injury to the left internal carotid artery (ICA), the artery was not continuous between the distal cervical and cavernous segments. The distal cervical ICA had been interrupted by the injury, and the petrous and cavernous segments were closed to antegrade flow. The cavernous carotid artery segment filled via the left posterior communicating artery (PcomA) and also from the right ICA via the anterior communicating artery. There was a proximal direct fistula between a pseudoaneurysm of the distal cervical left ICA and the left internal jugular vein (IJV). This proximal fistula was also supplied by a branch of the internal maxillary artery communicating with the pseudoaneurysm. This fistula subsequently drained in a retrograde fashion into the left transverse sinus (Fig 1). The second, more distal fistula, a carotid cavernous fistula (CCF) connected the cavernous left ICA and cavernous sinus.
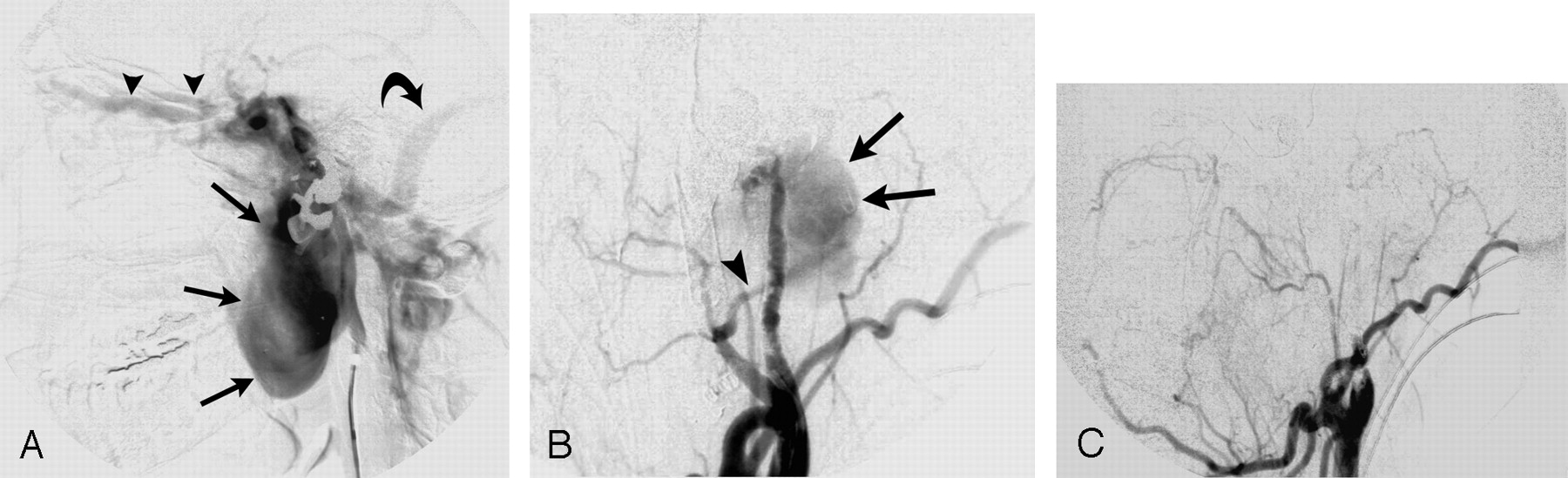
A, Lateral view from a left internal carotid angiogram demonstrates rapid filling of a large pseudoaneurysm (arrows), with subsequent drainage into the ipsilateral sigmoid sinus (curved arrow) and retrograde opacification of the superior ophthalmic veins (arrowheads). Note the lack of any opacification of normal carotid artery distal to the site of the fistula.
B, Lateral view from left common carotid artery angiogram after treatment of the carotid cavernous fistula (data not shown) and after glue embolization of the distal cervical ICA demonstrates a small amount of residual filling of the pseudoaneurysm (arrows) from a branch of the left internal maxillary artery (arrowhead).
C, Lateral view, left common carotid angiogram after embolization of the internal maxillary artery branch demonstrates no further filling of the pseudoaneurysm or the fistula.
The CCF was treated using detachable coil embolization of the cavernous sinus and the cavernous left ICA. This was accomplished by navigating a microcatheter up the left vertebral artery, across the PcomA, into the left ICA, and subsequently into the cavernous sinus.
The fistula between the cervical segment of the left ICA and the left IJV was treated with n-BCA. A Meditech occlusion balloon catheter (Boston Scientific/Meditech, Watertown, Mass) was placed into the proximal cervical ICA, and the balloon was inflated to cause flow arrest. A Prowler 10 microcatheter (Cordis Endovascular, Miami Lakes, Fla) was placed through the central port of the balloon catheter. A 1:1 mixture of n-BCA with Ethiodol (Trufill nBCA; Cordis Endovascular) was injected, and the microcatheter was immediately removed. The glue cast filled the distal ICA adjacent to the site of the fistula. Control angiogram demonstrated near complete occlusion of the fistula. There was continued supply to the pseudoaneurysm from the left internal maxillary artery (IMax), which was treated with detachable coil placement into the IMax. In addition, 2 detachable coils were placed proximal to the glue cast within the proximal left ICA.
After the procedure, the patient did well, with improvement in his swelling and some improvement in cranial nerve function. His chemosis and proptosis also improved, and he was discharged home 3 days after the procedure.
Patient 2
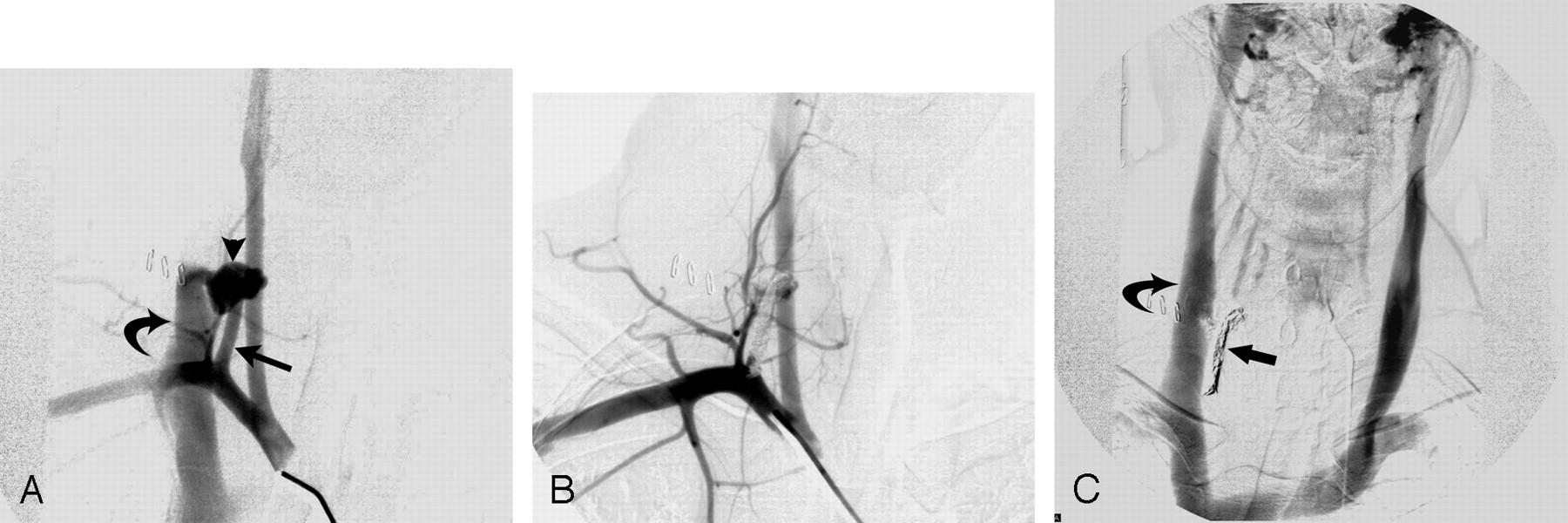
A 27-year-old man had been stabbed in the neck, back, and chest. His neck wound penetrated the right neck and had an oblique course through the right IJV and toward the proximal right vertebral artery (VA). CT angiogram (CTA) demonstrated a fistula between the right VA and IJV. Angiography confirmed these findings and demonstrated transection of the right VA at the fistula site (Fig 2). The distal right VA was supplied by the left VA and filled down to the level of the right posterior inferior cerebellar artery. A 5F guiding catheter was placed in the proximal right VA. A microcatheter was placed into the fistula, and detachable coil placement was attempted with Guglielmi Detachable Coils (Boston Scientific/Target Therapeutics, Fremont, Calif). However, these coils were not stable within the fistula and repeatedly prolapsed down the IJV. n-BCA, opacified with a minimal amount of tantalum powder in a slurry with ethiodized oil, was injected into the right vertebral artery, and the microcatheter was rapidly removed. Control angiograms demonstrated no further flow across the fistula and a widely patent right jugular vein. The patient was discharged home 3 days after the procedure after an uneventful hospital course.
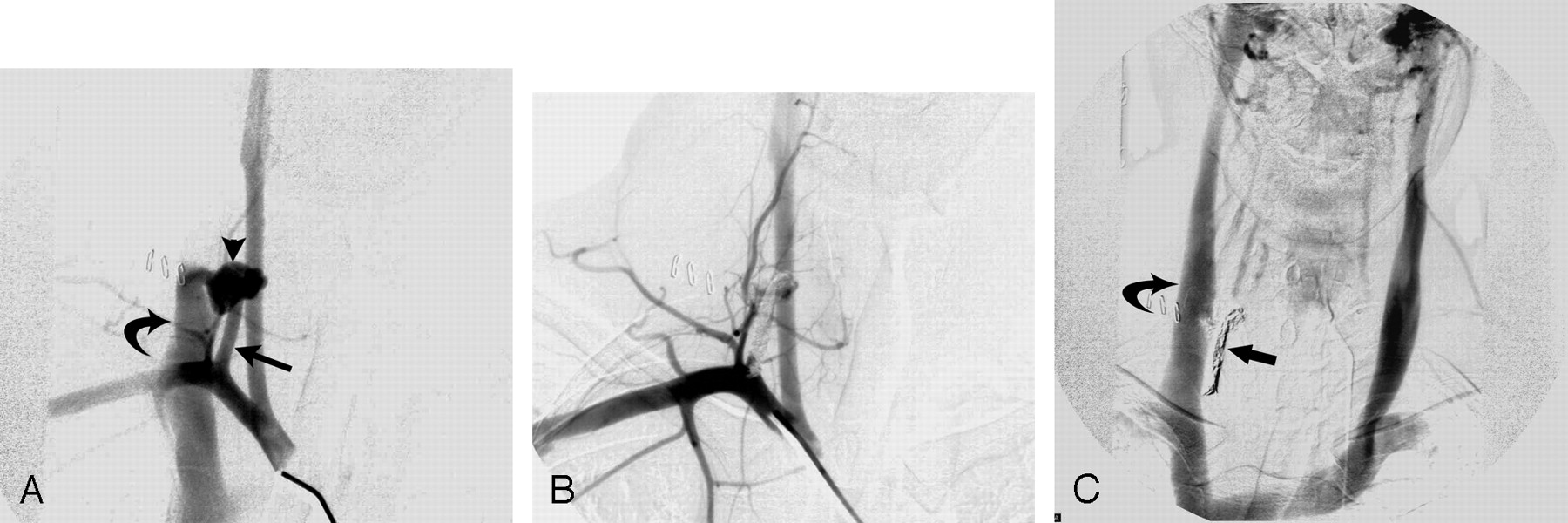
A, Frontal projection from a right subclavian artery angiogram demonstrates a rapidly filling fistula (arrowhead) between the right vertebral artery (arrow) and the right internal jugular vein (curved arrow). Similar to Fig 1, note the lack of filling of the vertebral artery distal to the fistula.
B, Frontal projection, right subclavian artery angiogram after glue embolization demonstrates no further filling of the fistula.
C, Venous phase image from a left vertebral artery angiogram demonstrates a widely patent right internal jugular vein (curved arrow). Note the glue cast in the right vertebral artery (arrow).
Discussion
Traumatic arteriovenous fistula in the neck can occur after either penetrating or blunt trauma. Endovascular therapy for these fistulas was first reported in the 1980s using balloon occlusion techniques.9,10 In the cases in which the vessel distal to the site of fistula is patent, the use of a covered stent allows preservation of the normal arterial flow.3,4,8,11 This technique involves navigating a guidewire into the normal vessel distal to the site of fistula and then spanning the abnormal segment with a covered stent, excluding the fistula from the circulation.
In both of our cases, the artery was transected by the penetrating injury, making preservation of flow in the parent artery impossible. In such cases, parent vessel sacrifice with detachable balloons or coils has been described.7,9,10,12 In both of these cases, coil embolization was believed to be unsuited to the task. In the first case, there was extremely high flow, with rapid filling of a pseudoaneurysm segment and subsequent retrograde filling into the ipsilateral sigmoid sinus. Given the large size of the pseudoaneurysm, placement of coils in the ICA was believed to carry a high risk of distal migration. In the second case, coil placement was attempted, but the coils repeatedly prolapsed into the internal jugular vein. Therefore, a rapidly polymerizing liquid embolic agent was used to provide immediate, complete arterial occlusion at the fistula site.
Cyanoacrylates have been well described for the treatment of high flow pial arteriovenous malformations, and for transarterial embolization of dural arteriovenous fistulas. n-BCA begins to polymerize upon contact with anionic moieties in blood. Varying amounts of lipid soluble contrast (ethiodized oil) can be added to the mixture to prolong polymerization time. In one case, flow-arrest was achieved with use of a balloon occlusion catheter, permitting use of a mixture of 1:1 ethiodized oil/n-BCA. In a second case, a short segment of proximal vertebral artery beyond the subclavian artery did not allow adequate length of artery needed to place a balloon occlusion catheter. Therefore, n-BCA opacified with a small volume of tantalum powder and ethiodized oil was used. This resulted in nearly instantaneous polymerization upon delivery via microcatheter. Potential complications of glue embolization include retained catheter and pulmonary embolism and should be considered before treatment.
Conclusions
The use of a liquid embolic agent for treatment of traumatic cervical arteriovenous fistulas has not been described previously. The use of n-BCA resulted in a rapid, permanent occlusion of these fistulas. This technique should be considered when anatomic factors preclude parent vessel preservation or safe coil embolization.
References
- Received December 6, 2005.
- Accepted after revision January 13, 2006.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}