
Abstract
SUMMARY: Appropriately sized 0.010- and 0.018-inch complex framing coils were placed in a wide-necked silicone aneurysm replica, and their stability was evaluated at variable physiologic flow rates using video recording. After detachment, the 0.010-inch coils demonstrated instability/prolapse that was proportional to flow rate. In contrast, 0.018-inch coils held their 3D configuration regardless of flow rate. The findings support the use of 0.018-inch coils (when possible) in aneurysms with unfavorable geometry, particularly in circulations with higher flow rates.
Endovascular treatment of wide-necked intracranial aneurysms remains a therapeutic challenge because of the risk of coil prolapse into the parent vessel.1,2 The recent introduction of devices (stents specifically designed for intracranial use) and techniques (balloon remodeling) have expanded our ability to treat aneurysms with unfavorable geometry.3–6 However, these measures can add to the complexity, duration, and consequent risk of the procedure. In addition, treatment of acutely ruptured aneurysms can be complicated by the necessity for full anticoagulation and possible need for antiplatelet therapy when these devices/techniques are used, increasing the risk of rehemorrhage.7 With this concern to avoid unnecessary patient risk, and the present increasing variety of coils and devices available to the interventionalist, our study sought to evaluate the effect of primary coil diameter choice (0.010- versus 0.018-inch) upon complex framing coil stability in a wide-necked silicone aneurysm replica at various (physiologic) flow rates.
Materials and Methods
Silicone replicas of wide-necked aneurysms were created using the lost wax technique.8,9 Two 10-mm aneurysm models were created (Fig 1) with sack-to-neck ratios (SNR) of 1.3 (wide-necked geometry) and 1.7 (favorable geometry). The silicone models were placed in a circuit of pulsatile non-Newtonian fluid with rheologic properties similar to those of blood.10 A fluid pump apparatus (Flowtek, San Diego, Calif) cycling at 1 pulse/s provided flow. The flow rate in the device was calibrated to simulate basilar, middle cerebral, and internal carotid artery levels (280, 360, and 420 mL/min, respectively).11 We placed single 10-mm 0.010- and 0.018-inch standard GDC 3D (Boston Scientific/Target Therapeutics, Fremont, Calif), MicroSphere (Micrus Endovascular, San Jose, Calif), and MicroPlex (MicroVention, Aliso Viejo, Calif) coils within 10-mm wide-necked aneurysms. A single 0.010 or 0.018-inch coil from each of the 3 manufacturers was placed in both the 1.3 and 1.7 SNR sidewall aneurysms. Coil stability was visually assessed and recorded with a digital video camera under increasing flow rates (each coil was observed for approximately 60 seconds at each flow rate). Instability was judged as mild (displacement/prolapse of a single loop), moderate (displacement/prolapse of more than one coil loop), or marked (displacement/prolapse of entire coil mass) for each coil type.

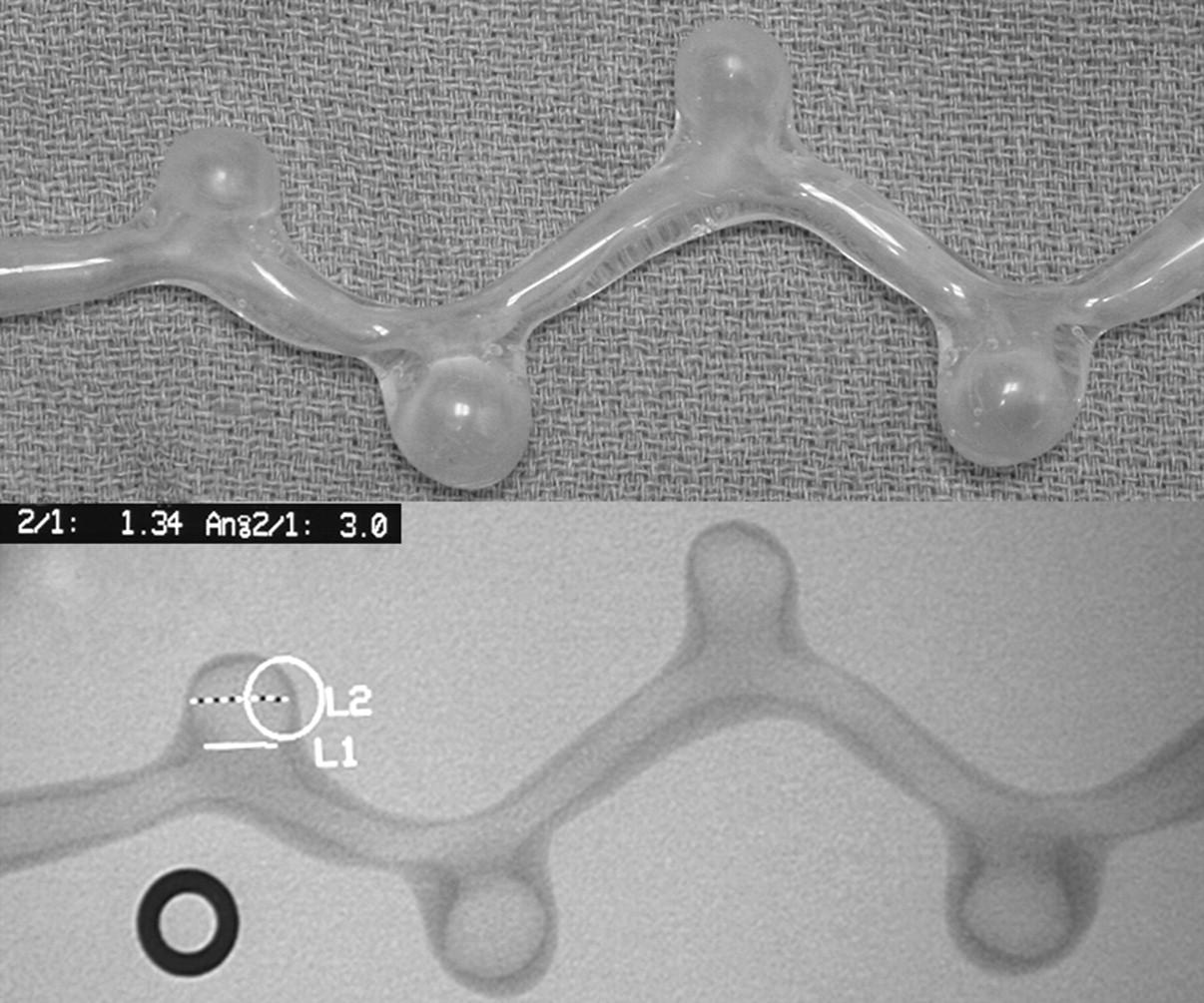
The wide-necked aneurysm replica. Photograph (top) and radiograph (bottom) show the wide-necked (SNR 1.34) sidewall aneurysm (far left on both images) used in the study. The model was placed in a circuit of pulsatile fluid with flow direction from right to left.
Results
The 0.010-inch coils held their 3D configuration in the 1.7 SNR model regardless of flow rate. In the 1.3 SNR model, the 0.010-inch coils were difficult to place, requiring 3 to 7 attempts before a presumed stable configuration was achieved (Fig 2). After detachment in the 1.3 SNR model, the 0.010-inch coils prolapsed (in different manners and to different degrees) into the parent vessel (Fig 3). Instability increased with increasing flow rates (Table 1). In contrast, the 0.018-inch coils held their 3D configuration in the 1.3 SNR model regardless of flow rate (Fig 4). These findings were reproducible and independent of coil manufacturer.

Stable 0.010-inch coil configuration within the wide-necked aneurysm replica after detachment.

A 0.010-inch coil within the replica at increasing flow rates (280, 360, and 420 mL/min, from left to right). Greater coil prolapse into the parent vessel was demonstrated with increasing flow rate.

A 0.018-inch coil within the replica at increasing flow rates (280, 360, and 420 mL/min, from left to right). No significant coil prolapse was demonstrated with increasing flow rate.
0.010-inch coil instability/prolapse versus flow rate
Discussion
In vivo coil stability is influenced both by inherent features of the aneurysm (which are nonmodifiable) and inherent characteristics of the embolization coil (modifiable). Aneurysm features that are known to affect coil stability include neck width and geometry, aneurysm location (neck inflow zone characteristics), and parent vessel flow rate.12,13 Coil characteristics that influence stability include filling versus framing geometry, coil stiffness, and, in light of our results, primary coil diameter.14,15 Our study investigated the in vitro effect of primary coil diameter upon stability; the results showed significantly better stability of the larger, 0.018-inch diameter coils. These results corroborate the findings by Marks et al,15 who demonstrated increased coil stability in a glass aneurysm model by increasing stiffness of the primary coil through modifying metal type and wire diameter used to create the coil. The approach in the current study was to create an aneurysm model that was then placed in a circuit of fluid with the flow dynamics matched as closely as possible to those found in humans. The model was then calibrated for flow velocity and pulsatility to match in vivo conditions. We recognize that there is an inherent difference in coefficient of friction when platinum coils are placed within silicone replicas compared with the lowered friction coefficient of endothelium; this difference is not accounted for in our study. However, the nature and degree of coil prolapse observed in our model closely matched in vivo wide-necked aneurysm coil behavior (before coil detachment) that we have observed. Aneurysm sizes for which both 0.010- and 0.018-inch coils are available are in the range of 6–15 mm, with the softer, 0.010-inch coils generally selected for smaller, ruptured aneurysms. By extrapolating our study to in vivo aneurysm therapy, the results would support the use of 0.018-inch coils in appropriate aneurysms of unfavorable (wide-necked) geometry, particularly in high flow locations (internal carotid artery versus basilar artery) or states (ie, arteriovenous malformation pedicle aneurysms).
Footnotes
Paper previously presented at: Annual Meeting of the American Society of Neuroradiology; May 11–17, 2002; Vancouver, British Columbia, Canada.
References
- Received June 13, 2006.
- Accepted after revision August 23, 2006.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}