
Abstract
BACKGROUND AND PURPOSE: The purpose of this study was to determine the efficacy and rate of complications in patients undergoing percutaneous vertebroplasty (PVP) for vertebral compression fractures as a result of secondary osteoporosis caused by long-term corticosteroid use compared with patients with primary osteoporosis treated with PVP.
MATERIALS AND METHODS: A retrospective review of all patients undergoing PVP was conducted to identify patients who also received long-term corticosteroid therapy. Outcomes including pain, periprocedural complications, and frequency of new fractures in patients receiving corticosteroids were compared with control patients undergoing PVP for primary osteoporosis.
RESULTS: Sixty-eight patients receiving long-term corticosteroid therapy underwent 79 PVP procedures. Patients treated with corticosteroids undergoing PVP were significantly younger and more likely to be male compared with control subjects. Patients receiving long-term corticosteroid treatment experienced significant pain relief immediately postprocedure and at 1 week, 1 month, 6 months, 1 year and 2 years postprocedure (P < .0001 at all time points). Patients receiving corticosteroids experienced similar decreases in pain from baseline compared with control subjects at all follow-up time points (P > .05). The complication rate for patients receiving corticosteroids was 4.4% compared with 3.4% for control subjects (P = .60). Patients on long-term corticosteroid treatment did not have an increased risk of new fractures after PVP compared with control subjects (P = .68).
CONCLUSIONS: Percutaneous vertebroplasty performed for vertebral compression fractures as a result of long-term corticosteroid therapy is as safe and effective in relieving pain as PVP performed in patients with vertebral compression fractures as a result of primary osteoporosis.
Percutaneous vertebroplasty (PVP) has been shown to effectively alleviate pain associated with vertebral compression fractures. Although PVP is widely applied and reported, most cases are in elderly persons with vertebral compression fractures as a result of primary osteoporosis. Long-term use of oral corticosteroids is a common cause of secondary osteoporosis and results in a large number of vertebral compression fractures. It has been estimated that 1 in 6 vertebral compression fractures in the population can be attributed to the use of oral corticosteroids, with doses as low as 2.5 mg per day sufficient to increase the risk of fracture.1 The use of corticosteroids also impairs wound healing and predisposes people to infection, which could lead to increased rates of complications after procedures such as PVP.
To our knowledge there exists no case series detailing long-term outcomes of PVP in long-term users of corticosteroids and comparing those outcomes to control patients with primary osteoporosis. We conducted a retrospective cohort study to investigate the effectiveness of PVP in alleviating pain, the rate of complications, and the risk of new fractures in patients using corticosteroids compared with control patients not using corticosteroids.
Materials and Methods
We performed a retrospective review of all patients undergoing PVP at our institution, a large tertiary referral center, between February 1999 and October 2005, after approval by the Institutional Review Board. During that time, 552 patients underwent 673 PVP procedures. Of these patients, we excluded from further study anyone undergoing PVP for spinal compression fractures as a result of trauma, malignancy, or hemangioma. Data collected on each patient included, but was not limited to, age, sex, indication for PVP, pain levels at rest and with activity before PVP and at 1 week, 1 month, 6 months, 1 year, and 2 years of follow-up, incidence of new fractures, use of corticosteroids, duration of corticosteroid use, and indication for corticosteroid use.
Percutaneous Vertebroplasty Technique
Patients with acute or subacute vertebral compression fracture(s) were treated with PVP unless the pain was improving with conservative management, the pain did not correlate with the level of fracture, or there were technical contraindications such as retropulsed bone, etc. Percutaneous vertebroplasty was performed as described previously2 by neuroradiologists who had a specific interest in spine intervention. In brief, PVP was performed under intravenous conscious sedation or general anesthesia as indicated with the use of biplane fluoroscopy. Transpediculate or parapedicular approaches were used in all cases. A cement mixture containing polymethylmethacrylate (PMMA) powder, gentamicin, and barium sulfate was injected into vertebral bodies with 11- or 13-gauge needles advanced into the central aspect of the vertebral body (for the unipediculate approach) or the midportion of the hemivertebra (for the bipediculate approach). Cement injection was terminated when the cement reached the posterior quarter of the vertebral body on the lateral projection or in the event of epidural, venous, or trans-endplate extravasation. After needle removal, patients were left on strict bed rest for 2 hours before discharge. Preprocedure and follow-up data on patients undergoing PVP included pain at rest and during activity obtained with the use of a verbal analog pain scale (0–10 Likert scale) administered by trained nurses or neuroradiologists before the procedure, immediately after the procedure, and at 1 week, 1 month, 6 months, 1 year, and 2 years after the procedure.
Statistical Analysis
Continuous and ordinal data are presented as median (range). Nominal data are presented as counts (percentage). Change in pain scores at various follow-up time points is presented as mean ± SD. Baseline comparisons and changes between baseline and each-follow-up measurement were calculated for each outcome and compared between patients using corticosteroids and control subjects by using Wilcoxon rank-sum and χ2 tests as appropriate. Multiple linear regression was used to further assess these relationships while adjusting for age, sex, and baseline pain scores. A P value less than .05 was considered significant. All statistical analyses were performed using JMP version 5.1 software (SAS Institute, Cary, NC).
Results
Patient Population
Sixty-eight patients underwent 79 PVP procedures for osteoporotic vertebral compression fractures secondary to long-term corticosteroid therapy during the time period studied (Table 1). These patients were treated with corticosteroids for a median of 43.5 months (range, 2–420 months) at a median dose of 10 mg of prednisone equivalents/day (range, 2–60 mg/day) (Table 2). Most of the patients used prednisone (97.5%), and the remaining patients used methylprednisolone (2.5%). Corticosteroids were used at the time of PVP in 68 of 79 (86.1%) procedures. The most common indication for corticosteroid use was chronic obstructive pulmonary disease (n = 23) followed by rheumatoid arthritis (n = 20) and immunosuppression as a result of organ transplantation (n = 11) (Table 2).
Patient demographics
Patient steroid use and indications
The demographics of patients on long-term corticosteroid therapy were compared with 379 patients who underwent 475 PVP procedures for primary osteoporotic vertebral compression fractures during the same time period (Table 1). Patients undergoing PVP who received long-term corticosteroid treatment were significantly younger (68 vs 77 years; P < .0001) and more likely to be male (2:3 vs 5:14 male/female ratio; P = .01) than control subjects. Patients on corticosteroids had a median of 2 vertebral levels (range, 1–5 vertebral levels) treated, which was significantly greater (P = .009) than the median of 1 vertebral level (range, 1–11 vertebral levels) treated in patients not receiving corticosteroids. Patients receiving long-term corticosteroid treatment experienced a median of 2 months of pain (range, 0.1–60 months) before the procedure, which was similar to patients not receiving corticosteroids, who also experienced a median of 2 months of pain (range, 0.03–15 months; P = .30). The risk of new fractures after PVP was not significantly higher in patients receiving corticosteroids. Twenty of 68 (29.4%) patients receiving corticosteroids experienced a new fracture after PVP, which was similar to 110 of 379 (29.0%) patients not receiving corticosteroids who developed new fractures (P = .68).
Outcomes
Both patients receiving long-term corticosteroid treatment as well as control patients receiving no corticosteroids experienced significantly decreased pain levels at rest and with activity at all follow-up time points (2 hours, 1 week, 1 month, 6 months, 1 year, and 2 years) compared with preprocedural pain levels (P < .0001 for all time points). Patients receiving corticosteroids who underwent PVP experienced median pain levels (0–10 Likert scale) at rest of 1 (0–8, n = 68), 2 (0–10, n = 66), 0.5 (0–8, n = 56), 0 (0–8, n = 45), 0 (0–8, n = 35), and 0 (0–6, n = 28) compared with 0 (0–10, n = 379), 0 (0–10, n = 374), 0 (0–10, n = 368), 0 (0–10, n = 303), 0 (0–10, n = 227), and 0 (0–10, n = 145), respectively, at 2 hours, 1 week, 1 month, 6 months, 1 year, and 2 years after PVP, respectively. Patients receiving corticosteroids undergoing PVP experienced median pain levels during activity of 3.5 (0–10, n = 68), 4 (0–10, n = 66), 4 (0–8, n = 56), 3 (0–10; n = 45), 4 (0–10, n = 35), and 3 (0–10, n = 28) compared with 3 (0–10, n = 379), 4 (0–10, n = 374), 4 (0–10, n = 368), 2.5 (0–10, n = 303), 3 (0–10, n = 227), and 2 (0–10, n = 145) at 2 hours, 1 week, 1 month, 6 months, 1 year, and 2 years after PVP, respectively. There was not a significant difference in absolute pain values at any time point between patients on corticosteroids compared with control subjects (P > .05 at all time points). Change in pain scores from preprocedural levels to each follow-up time point did not significantly differ between the 2 groups at rest or with activity by univariate analysis (Fig 1A, -B) or when using multiple linear regression adjusting for age, sex, and baseline pain scores either. The mean length of follow-up for patients on corticosteroids was 12.1 ± 10.3 months and 13.1 ± 9.3 months for control patients.
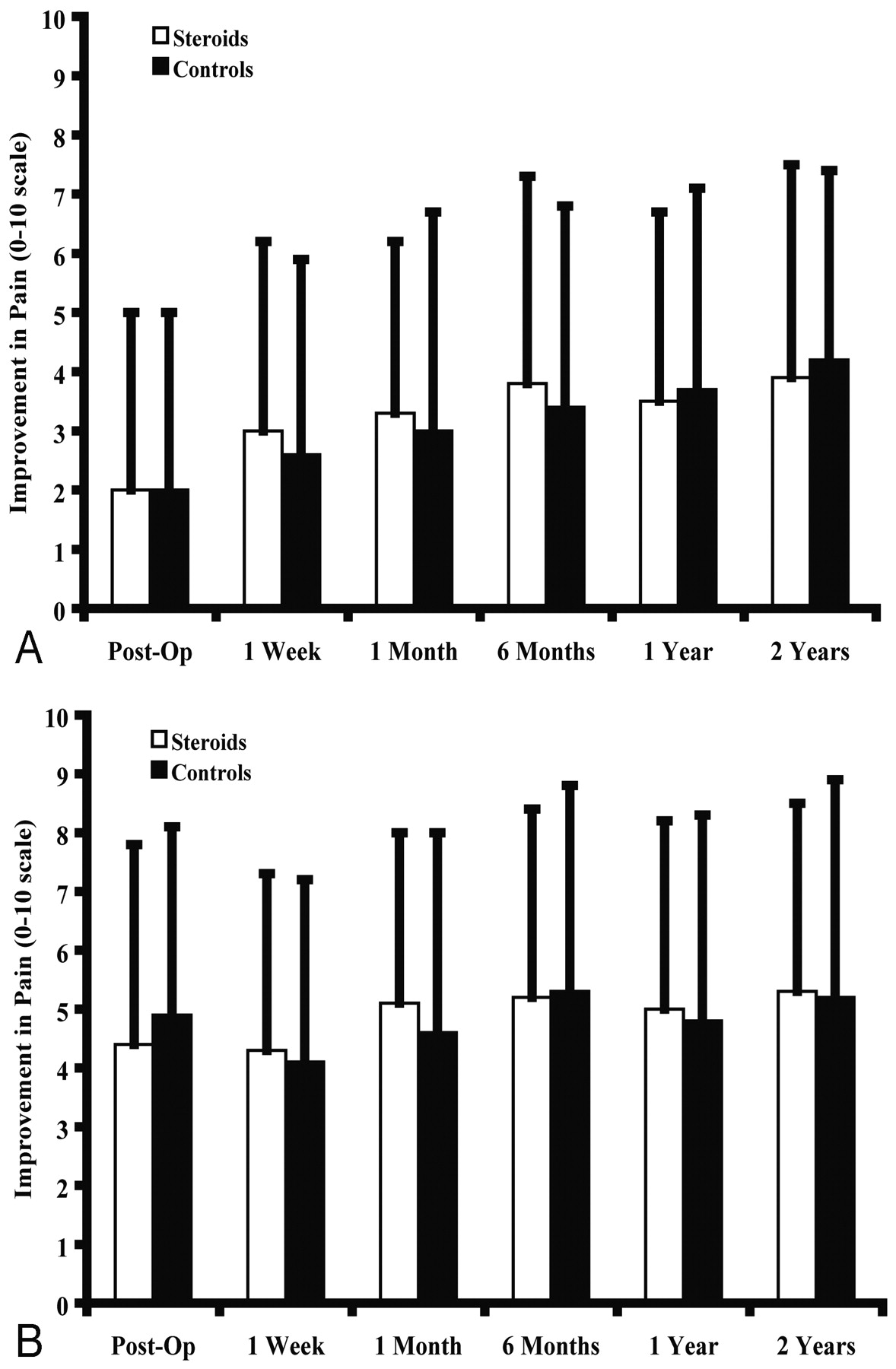
Improvement in pain after vertebroplasty. Patients were asked to rate their pain on a 0–10 Likert scale preoperatively and at the follow-up times indicated at rest (A) and with activity (B). Data are depicted as the mean ± SD improvement in pain from baseline.
Complications
Patients receiving long-term corticosteroid therapy did not experience an increased incidence of clinically significant complications compared with patients not receiving corticosteroids (Table 1). There were 3 clinically significant complications in 79 (4.4%) PVP procedures in patients taking corticosteroids compared with 13 complications of 475 (3.4%) PVP procedures in control subjects. Clinically significant complications in patients receiving long-term corticosteroid therapy included 2 patients who developed radiculopathies after the procedure and 1 patient who suffered a fracture of the transverse process of a vertebra. Complications in the control group included 4 rib fractures, 3 radiculopathies, 2 hypertensive episodes, 2 episodes of respiratory arrest, 1 case of PMMA pulmonary embolus, and 1 case of postprocedural urinary retention. There were no deaths in either group as a result of the procedure, and all patients, except those suffering a radiculopathy, resolved without sequelae.
Discussion
This study retrospectively analyzed the clinical outcomes of a series of patients treated with PVP for osteoporotic vertebral fractures caused by long-term corticosteroid use. We show that PVP can be performed with similar efficacy and safety in patients receiving long-term corticosteroids compared with control subjects who suffered from primary osteoporosis. Patients undergoing long-term corticosteroid treatment experienced significant pain relief after PVP that was similar in magnitude to patients not receiving corticosteroids. The incidence of complications in patients using corticosteroids was similar to the incidence of complications in patients not receiving corticosteroids. In particular, there were no complications related to infection or wound healing, and there was no increased risk of new fractures among patients receiving corticosteroid therapy.
While pain relief and the incidence of complications were similar between patients on corticosteroids and control subjects there were some significant differences between the 2 groups. The frequency of men undergoing PVP was significantly increased in patients receiving corticosteroids. This probably represents the fact that PVP is typically performed to treat vertebral compression fractures as a result of primary osteoporosis, which predominantly affects elderly women, whereas secondary osteoporosis as a result of long-term corticosteroid use is not likely to show a sex bias. In addition, the age of patients receiving long-term corticosteroid treatment was significantly decreased compared with control subjects, which illustrates that osteoporosis induced by corticosteroids is directly dependent on the duration of treatment and not patient age.
Multiple other investigators have published large case series on PVP in patients with vertebral compression fractures as a result of primary osteoporosis with excellent results. For example, Do et al3 prospectively followed 167 patients undergoing 207 PVPs for osteoporotic vertebral compression fractures and found that there was an approximately 70% reduction in pain levels, significantly increased mobility, and significantly decreased analgesic use after PVP. Prather et al4 prospectively followed 50 patients for 1 year after PVP for osteoporotic vertebral compression fractures and found that there was significant improvement in visual analog pain scores and functional scores based on the Roland-Morris questionnaire. These studies, among others, illustrate the effectiveness of PVP in patients with vertebral compression fractures as a result of primary osteoporosis.
It is noteworthy that few series have included results of corticosteroid-induced fractures, even though it is our opinion that PVP is widely applied to this patient population. Mathis et al5 reported a case of PVP performed on a woman with a 10-year history of corticosteroid therapy for systemic lupus erythematosus who was bedridden as a result of multiple vertebral compression fractures before the procedure; after PVP, however, the patient experienced significant pain relief and was able to resume most activities of daily living. Harrop et al6 performed a retrospective review of 115 patients undergoing kyphoplasty for vertebral compression fractures, including 35 patients receiving long-term corticosteroid treatment, and found that 48.6% of these patients developed a subsequent fracture compared with only 11.3% of patients treated for primary osteoporosis. These results contrast with the current report, in which a significant increase in subsequent fractures among patients on corticosteroids was not observed. This might be explained by procedural differences between PVP and kyphoplasty; it is possible that the latter predisposes patients to an increased risk of subsequent fracture, particularly at vertebral levels adjacent to those treated.
Our outcomes are similar to those of Jensen et al2 and Singh et al.7 Jensen et al2 reported that 26 of 29 patients (90%) undergoing PVP experienced significant pain relief after the procedure, though the follow-up period in that study was limited to only several days. Singh et al7 reported that 82% of patients undergoing PVP for primary osteoporotic vertebral compression fractures experienced complete resolution of pain at 2-year follow-up. Although the studies of Jensen et al2 and Singh et al7 illustrate the efficacy of PVP in primary osteoporotic vertebral compression fractures, they do not address the efficacy of PVP in patients with osteoporotic vertebral compression fractures secondary to corticosteroid treatment. In the current study, 89% of patients receiving long-term corticosteroid treatment who underwent PVP experienced significant pain relief at 1 year of follow-up with a low rate of complications. Thus, the results of the current study suggest that the outcomes of patients receiving long-term corticosteroid treatment who undergo PVP are equivalent to those of patients not using corticosteroids.
This study is not without limitations. First, although this is the first report on the outcomes, efficacy, and safety of PVP in patients on corticosteroids, this study is retrospective. Second, patients using corticosteroids in this study were treated for a median of 41 months, with some as long as 420 months, making it difficult to accurately assess the dose of steroid each patient received. Finally, the study was conducted at a tertiary referral center biasing the patient population as well as complicating efforts to assess the frequency of new fractures patients may have suffered that may have been treated at other institutions and not reported at follow-up.
Although our study suggests that patients receiving long-term corticosteroid treatment who undergo PVP have excellent clinical outcomes, a prospective study is needed to confirm these results. In addition, a study comparing the clinical outcomes and complication rate of patients receiving long-term corticosteroid treatment who undergo PVP with those patients on corticosteroids receiving optimal conservative therapy or kyphoplasty is necessary to determine which treatment regimen is preferred in this patient population. Also of interest would be a study investigating the temporal and spatial relationship of new fractures to the initial vertebral fracture treated by PVP in patients treated with corticosteroids. Trout et al8 studied the incidence and location of new fractures after PVP in 432 patients. They concluded that subsequent vertebral compression fractures after PVP were more likely to occur in adjacent vertebral levels and that these adjacent fractures occurred significantly sooner than nonadjacent fractures. A larger population of patients receiving long-term corticosteroid treatment who undergo PVP for vertebral compression fractures is needed to assess whether the correlation between PVP and adjacent fractures exists in this subset of patients as well.
Conclusion
Patients with vertebral compression fractures as a result of secondary osteoporosis as a result of long-term corticosteroid use experience similar levels of pain relief, complications, and new fractures after percutaneous vertebroplasty as patients with vertebral compression fractures caused by primary osteoporosis. These results support the use of percutaneous vertebroplasty to treat vertebral compression fractures unresponsive to conservative management in patients receiving long-term corticosteroid therapy.
References
- Received May 4, 2006.
- Accepted after revision June 7, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Asymptomatic and Unrecognized Cement Pulmonary Embolism Commonly Occurs with Vertebroplasty
- Subsequent Fracture after Percutaneous Vertebroplasty Can Be Predicted on Preoperative Multidetector Row CT
- Clinical Outcomes with Hemivertebral Filling during Percutaneous Vertebroplasty
- Efficacy of Percutaneous Vertebroplasty for Multiple Synchronous and Metachronous Vertebral Compression Fractures
- Vertebroplasty for the Treatment of Traumatic Nonosteoporotic Compression Fractures