
We discuss a unique case of a congenital glioependymal cyst arising from the left middle cranial fossa with extension into the left orbit causing severe proptosis, a presentation that has not been reported previously. A female neonate at 38 weeks’ gestational age was diagnosed with severe left proptosis on a prenatal sonography at 35 weeks’ gestation. The sonogram was performed to determine the size of the infant due to a maternal history of macrosomia in a previous pregnancy. The infant's prenatal history was otherwise unremarkable. The patient was delivered by an uncomplicated cesarean birth.
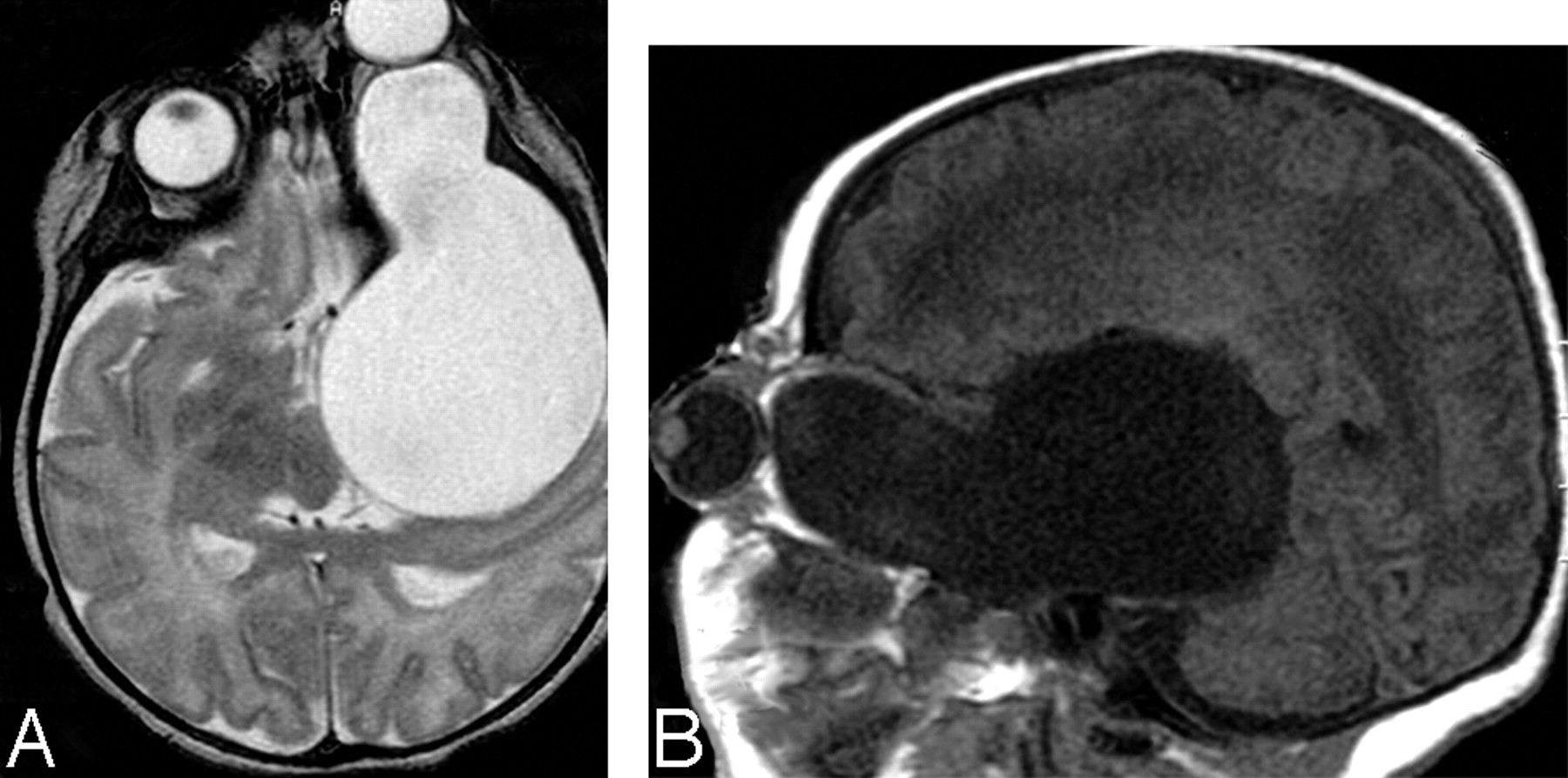
Physical examination showed severe left proptosis with intact extraocular movements. The right eye and findings from the remaining physical examination were unremarkable. The results of chromosome studies were normal. Noncontrast enhanced CT demonstrated a cystic structure occupying the left middle cranial fossa and extending into the left orbit. MR imaging verified the CT findings and showed no associated brain abnormalities (Fig 1).
On the patient's second day of life, a cyst-to-peritoneum shunt was placed without complications. The left proptosis rapidly improved, and a sonogram showed only a small cyst on the fifth day of life. The patient was discharged but was returned on the 15th day of life because of recurrent left proptosis. After a failed shunt revision, a left temporal craniotomy was performed with removal of the lateral wall of the cyst and fenestration of the cyst to the subarachnoid space. No brain parenchymal abnormalities were identified. Since that time, the child has had an uneventful clinical course, and a noncontrast CT 1 year later showed that only a small cyst remained.
Upon gross examination, the pathologic specimen contained multiple fragments of fibrous tissue in loose aggregates (not photographed). Microscopic examination revealed that the specimen consisted of a thick layer of glial/connective tissue lined by a single layer of cuboidal or columnar epithelium with cilia. In certain areas, papillary structures resembling the choroid plexus were identified. No goblet cells were seen in the specimen. The epithelium was diffusely positive for S-100 protein and glial fibrillary acidic protein, and focally positive for cytokeratin in the areas resembling the choroid plexus. The epithelial cells were negative for epithelial membrane antigen and carcinoembryonic antigen. Focal acute inflammation was noted, consistent with previous surgical intervention. The histologic and immunophenotypic findings were most consistent with a glioependymal cyst.
Based on the imaging features, the differential diagnoses included a glioependymal cyst, ependymal cyst, arachnoid cyst, enterogenous cyst, dermoid cyst, encephalocele, and congenital dysplasia of the sphenoid wing in neurofibromatosis type I. The diagnosis of a glioependymal cyst requires correlation of clinical, radiologic, and histologic findings. Glioependymal cysts, also known as neuroepithelial cysts, are thought to arise from ectopic rests of primitive neuroglial tissue and therefore can arise anywhere in the neuraxis.1 On imaging, they appear as nonenhancing CSF containing thin-walled cysts.2,3 Our case is unique because of the unusual clinical presentation of severe proptosis. To our knowledge, neither this presentation nor the imaging appearance has been reported previously in a neonate with a glioependymal cyst.

Noncontrast MR imaging of axial T2 (A) and sagittal T1 (B) images show the cystic structure after CSF signal intensity on all sequences. Note proptotic left globe.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.