
Abstract
BACKGROUND AND PURPOSE: Endoaneurysmal implantation of fibroblasts may promote healing of aneurysms and reduce recanalization after therapeutic embolization. The purpose of our study was to develop a device for delivery of fibroblasts with use of current microcoil technology.
MATERIALS AND METHODS: Cell carrier devices and cell-free devices were fabricated by associating collagen gels (with or without fibroblasts) with platinum microcoils. During the propagation of control cell carrier devices for 1 week in culture, cell-mediated gel contraction (CMGC) occurred. Modified cell carrier devices created by glutaraldehyde cross-linking, ascorbate coculture, or extended CMGC were also characterized in vitro. Devices were deployed through microcatheters (533 μm lumen, 160 cm length). Gel retention, cell retention, cell death, and the ability to support local cell migration were analyzed in vitro.
RESULTS: Cell viability was reduced by glutaraldehyde cross-linking but not by microcatheter transit. During microcatheter transit, cell carrier devices liberated minimal particulate matter and cellular DNA. Liberated particulate matter was reduced by glutaraldehyde cross-linking (P < .05) and extended CMGC (P < .04). Only cell carrier devices treated with glutaraldehyde cross-linking did not exhibit cell migration after microcatheter transit. Passage of cell-free devices through microcatheters sheared off most of their collagen gel.
CONCLUSION: Collagen gel-platinum microcoil complexes can mediate efficient transmicrocatheter delivery of viable, migration-capable fibroblasts. CMGC is a necessary component of the process of gel stabilization that enables successful microcatheter transit. Although extended CMGC and glutaraldehyde cross-linking enhance gel stabilization, glutaraldehyde cross-linking decreases cell viability and migratory potential.
In recent years, coil embolization of cerebral aneurysms has gained widespread acceptance as a safe and efficacious alternative to open surgical repair.1,2 Its main limitation is its inconsistency to produce permanent occlusion of an aneurysm.3–5 An emerging strategy to improve the durability of aneurysm occlusion has focused on enhancing biologic processes that lead to the formation of an endovascular scar. Promising applications include embolic materials modified with biologically active proteins and endoaneurysmal implantation of living cells.6–13 In animal studies, fibroblasts implanted into carotid arteries or experimental aneurysms with platinum microcoils, and vascular smooth muscle cells implanted into experimental aneurysms with collagen sponges accelerated thrombus organization and enhanced endovascular healing.11,12,14
Although cells can be grown on platinum microcoils, experimental studies13,14 have shown that cells on the coil surface (not within the coil interstices or inner lumen of the coil) are often sheared off when the coil is passed through a microcatheter or through the plastic housing assembly in which detachable coils are typically packaged. The quantitative efficiency of cell delivery with this approach can be debated because a variable number of cells are retained in the interstices and inner lumen of the coil, and effective cell transplantation has been demonstrated in animal models.14 However, the shearing effect, in addition to decreasing the efficiency of cell delivery, also has the potential for thromboembolic complications. To address these points, we constructed a bioengineered device by associating platinum microcoils with collagen gels containing fibroblasts. The device profile and gel stability required for microcatheter transit was achieved through cell-mediated gel contraction (CMGC).15 Investigations were performed to augment gel stability, modifications consisting of glutaraldehyde cross-linking, ascorbate coculture, and extended CMGC. Glutaraldehyde cross-linking is known to increase the mechanical strength of collagen gels, and ascorbate is known to enhance formation of intermolecular cross-links in collagen.16,17 The effects of microcatheter transit on cell viability, liberation of particulate matter, and cell loss were evaluated. Our study assessed the feasibility of fibroblast delivery with current microcoil technology and established the foundations to develop bioengineered microcoil-collagen-cell systems that enable efficient microcatheter delivery of functional cells for aneurysm therapy.
Methods
Cell Culture
Neonatal human dermal fibroblasts (Clonetics-Biowhittaker, Walkersville, Md) were subcultured, preserved in liquid nitrogen, and propagated for 5 to 10 passages before harvesting. Cells and cell-containing constructs were cultured at 37°C in Dulbecco modified Eagle's medium supplemented with L-glutamine, penicillin-streptomycin, and 10% fetal bovine serum.
Collagen Gel Mixtures
Solutions of type I rat tail collagen in 0.02 n acetic acid (Collaborative Biomedical Products, Bedford, Mass) were used to prepare collagen gel mixtures for cell-free CFDs and cell carrier devices CCDs. Collagen gel mixtures were a combination of collagen, fetal bovine serum, Dulbecco modified Eagle's medium, and neonatal human dermal fibroblasts. Fibrillogenesis was then induced by neutralizing with 0.1 n NaOH. Except for gel contraction studies, collagen gels with neonatal human dermal fibroblasts contained 107 cells/mL.
Device Fabrication
Straight MicroPlex platinum microcoils (0.0017-inch core wire; 0.0095-inch helix diameter) (MicroVention, Aliso Viejo, Calif) were placed into modified polyvinyldine diflouride hollow fiber tubes (1-mm diameter, 20–30 mm length) (Spectrum, Rancho Dominguez, Calif). Straight coils were used because their configuration facilitated transfers. The helical diameter of the coil was determined by availability. These tubes were then loaded with collagen gel mixtures (2 mg/mL collagen with or without neonatal human dermal fibroblasts) and cultured for 30 minutes to induce gelation. Rubber caps on the tubes kept them suspended in a medium of tissue culture.
After gelation, we removed the devices from the modified polyvinyldine diflouride tubes and cultured by using a suspension technique that kept the surface of the collagen gel bathed in tissue culture medium and prevented cell migration. To achieve CMGC, we propagated the devices in culture for 7 days with media exchanges every 2 days; the effect of an extended 14-day culture is described below. Constructs were 2 cm in length, unless indicated otherwise.
Collagen Gel Modifications
In extended CMGC modified CCDs, the gel contraction culture was increased from 7 to 14 days. We accomplished glutaraldehyde cross-linking by submerging devices in 0.3% or 1% glutaraldehyde, then rinsing with phosphate-buffered saline. In ascorbate coculture modified CCDs, the medium used during the gel contraction culture was supplemented with ascorbate (50 μg/mL) for the first 3 days of the 7-day culture. We used unmodified CCDs as controls for modified cell carrier devices.
Characterization of CMGC
We characterized collagen gel contraction as a function of neonatal Human Dermal Fibroblasts (nHDF) attenuation to determine optimal cell attenuation for device fabrication. We constructed CCDs with different cell densities (2 × 107, 1 × 107, 1 × 106, and 1 × 105 cells/mL) by using a 7-day gel contraction culture (T.T.). Identical devices devoid of cells were used as controls. During the gel contraction culture, we measured the diameter of each device daily under a light microscope with an ocular lens scale (TT). Longitudinal gel contraction was minimal and similar at all nHDF densities (data not reported).
Deployment of Transcatheter
We manually loaded the CCDs and CFDs with fine forceps into the hubs of Renegade microcatheters (length 160 cm, lumen diameter 533 μm) (Boston Scientific, Fremont, Calif). We deployed the devices into tissue culture dishes by perfusing microcatheters with normal saline at 300 mm Hg (2 mL saline/device). Contents of each microcatheter were then flushed into the dish with an additional 1.0 mL normal saline. The effluent was centrifuged and supernatant discarded to a residual volume of 0.5 mL. The 0.5-mL samples and pellets were stored at −20°C for subsequent determination of cellular DNA or trypan blue-stained particles. Each CCD and CFD was examined by light microscopy before and after deployment of the transmicrocatheter. We performed duplicate trials for each type of device.
Live and Dead Cell Staining and Confocal Microscopy
We performed live and dead cell staining using calcein-AM/ethidium homodimer 1 (CE) stain (Molecular Probes, Eugene, Ore) to examine the distribution of cell death caused by glutaraldehyde cross-linking or microcatheter transit.18 We incubated the CCDs at 37°C in the CE stain for 45 minutes, rinsed them with phosphate-buffered saline, and imaged them on a Zeiss LSM 510 confocal microscope (Carl Zeiss, Thornwood, NY).
MTT Cell Viability Measurements
We performed MTT (3-[4,5-dimethylthiazol-2-yl]-2,5-diphenyl tetrazolium bromide) assays on CCDs 3 cm long immediately after CMGC or glutaraldehyde cross-linking modification.19 Briefly, each CCD was incubated at 37°C in 1 mL of 0.5 mg/mL MTT (Sigma, St. Louis, Mo) for 2 hours. After exchange of the MTT solution for 1 mL of isopropanol, optical density (OD) was measured at wavelengths of 560 and 700 nm in a microplate reader (Bio-Tek Instruments, Winooski, Vt). We used the differences in OD (OD560 nm − OD700 nm) to estimate viable cells/CCD by using a standardized curve established with known numbers of neonatal human dermal fibroblasts.
Trypan Blue Assays
We estimated the protein debris released from CCDs during microcatheter transit by analyzing microcatheter samples of effluent. Briefly, the samples were thawed and centrifuged. The recovered pellets were suspended in 1 mL trypan blue (0.4%) solution and vortexed. We then counted the trypan blue-stained particles under a light microscope with a hemocytometer.
DNA Assays
We estimated cell loss from the CCDs during microcatheter transit by measuring DNA in microcatheter effluent samples using a Hoechst-33342 (Sigma) DNA binding dye.20 The cell carrier devices analyzed were those that released the most debris in trypan blue assays (control and ascorbate coculture). Briefly, microcatheter effluent samples were thawed and centrifuged. Recovered pellets were suspended in Hoechst dye (0.05 mg/mL) and loaded into a microplate reader (VWR, Suwane, Ga). After a 15-minute incubation in the dark at room temperature, we performed analysis on a fluorescence-based plate reader (Molecular Devices, Sunnyvale, Calif) by using a 360-nm excitation wavelength and a 460-nm emission wavelength. Calf-thymus DNA standards (Sigma) were analyzed in parallel. To estimate the total DNA per CCD, we vigorously vortexed the control CCDs in phosphate-buffered saline and centrifuged for 3 cycles. The resulting pellets were analyzed as above.
Evaluation of Cell Migration
The CCDs recovered after microcatheter transit were studied by placing CCDs on the surface of a 35-mm tissue culture plate in 2 mL Dulbecco's Modified Eagle's Medium and culturing for 3 days. After the 3-day culture interval, we examined the plates by light microscopy.
Statistical Analysis
Quantitative data are expressed as mean ± SD. We carried out statistical analyses by using the Student t test (Microsoft Excel, Microsoft, Redmond, Wash) (P < .05). Differences in the degree of collagen gel contraction produced by specific nHDF densities as well as differences between modified versus control devices were tested for statistical significance relative to specific end points. Specific end points evaluated included the percentage change in cell viability affected by the modification, the amount of particulate matter liberated during microcatheter transit, and amount of cell loss (estimated by DNA loss) caused by microcatheter transit.
Results
Characterization of CMGC
Collagen gel contraction increased with nHDF attenuation up to 107 nHDF/mL. At each nHDF attenuation tested, gel contraction increased rapidly during the first 4 days and slowly during the following 3 days (Fig 1). At 7 days, gel contraction was significantly greater with 107 nHDF/mL than with 105 nHDF/mL (P = .003) or 106 nHDF/mL (P = .008).

Dependency of collagen gel contraction on fibroblast attenuation and time. Collagen gel diameter measured at time point (Dm) plotted as percentage of the initial gel diameter (Di) over a 7-day period for cell carrier devices of varying initial fibroblast (cell) attenuation. Initial gel collagen concentration was 2 mg/mL for all cell carrier devices and control devices containing no cells. Each data point is an average of triplicate samples (except for cell attenuation of 2 × 107 cells/mL) (n = 2); error bars are SDs for each data series. Day 7: 107 cells/mL construct versus 106 cells/mL construct (P < .08); 107 cells/mL construct versus 105 cells/mL construct (P < .003); 107 cells/mL construct versus 2 × 107 cells/mL construct (P > .25) (printed with permission from the Mayfield Clinic).
Glutaraldehyde Cross-Linking and Ascorbate Coculture Effects on Cell Viability by MTT Assay
In preliminary tests, cell carrier devices cultured for 3 days were exposed to 0.3% glutaraldehyde for 10 seconds, 30 seconds, or 2 minutes and to 1% glutaraldehyde for 10 seconds, 30 seconds, or 2 minutes. All treatments resulted in viable cell loss, with the highest loss observed after 1% × 30 seconds and 1% x 2 minutes. Subsequent experiments were performed with CCDs subjected to the most aggressive remaining treatments (ie, 0.3% × 2 minutes and 1% × 10 seconds).
Relative to control CCDs, 0.3% × 2 minutes reduced viable cells by 80% (P = .0008), and 1% × 10 seconds reduced viable cells by 62% (P = .0021) (Fig 2). Ascorbate coculture had no effect on cell viability relative to control CCDs (P = 0.32) (Fig 2).

Effect of gel modifications on cell viability as determined by MTT assays. Remaining percentage of viable cells in modified cell carrier devices relative to control cell carrier devices (control) with result for each condition reported (average of triplicate experiments). Error bars indicate the SD for each triplicate series. Cell carrier devices are modified by exposure to the following: glut 0.3% (0.3% glutaraldehyde for 2 minutes); glut 1% (1% glutaraldehyde for 10 seconds); and ASC (ascorbate coculture) (printed with permission from the Mayfield Clinic).
Distribution of Cell Death by Microcatheter Transit and Glutaraldehyde Cross-Linking by Live and Dead Cell Examinations
No evidence of cell death was found in control CCDs recovered after microcatheter transit and control CCDs not passed through microcatheters. Widely distributed areas of cell death were concentrated in regions near the outer surfaces in CCDs modified by 0.3% glutaraldehyde × 2 minutes (n = 3) or 1% glutaraldehyde × 10 seconds (n = 3) (Fig 3A, B).

Fluorescence confocal micrographs of live and dead cell-stained control cell carrier devices. Images are argon-laser fluorescence confocal micrographs (original magnification × 20) of control cell carrier devices recovered after microcatheter transit (A) and those not passed through microcatheters (B) obtained after staining for live (green fluorescence) and dead cells (red fluorescence) (printed with permission from the Mayfield Clinic).
Effects of Microcatheter Transit on Device Structure by Light Microscopy
Before microcatheter transit, control CCDs had a semitransparent gel layer interdigitating between windings of the microcoil. The gel was uniform in thickness with some minor variations. The surface of the gel was rough with diffuse irregularities consisting of linear, amorphous, or globular excrescences. After microcatheter transit, control CCDs demonstrated increased surface irregularity, without segmental or geographic foci of gel loss (Fig 4).

Photomicrograph showing effect of control cell carrier device after microcatheter. Notice linear (arrows) and amorphous (arrowheads) surface irregularities (printed with permission from the Mayfield Clinic).
Before microcatheter transit, the CFDs were microscopically similar, except that their gel layer was thicker and completely transparent. During microcatheter transit, the CFDs lost most of their gel.
Before microcatheter transit, the gel layer of glutaraldehyde cross-linking modified CCDs (0.3% glutaraldehyde × 2 minutes) was distinguished by a smooth surface. The CCDs modified by ascorbate coculture and extended CMGC were similar to control CCDs before microcatheter transit. After microcatheter transit, only CCDs modified by glutaraldehyde cross-linking (0.3% glutaraldehyde × 2 minutes) and extended CMGC were distinguished from the control CCDs by preservation of pretransit surface topography. The CCDs modified by ascorbate coculture were similar to the controls in that they demonstrated an increase in surface irregularities, without segmental or geographic foci of gel loss or disruption.
Particulate Matter Released during Microcatheter Transit by Trypan Blue Assay
All modifications examined reduced the amount of particulate debris liberated during microcatheter transit relative to the control CCDs (Fig 5). Reduction was significant for glutaraldehyde cross-linking (P = .04 for 0.3% and P = .02 for 1%) and extended CMGC (P = .039) but not for ascorbate coculture.

Particulate matter released from cell carrier devices during microcatheter transit measured by the number of trypan blue staining particles per device (average of triplicate experiments). Error bars indicate the standard deviation for each triplicate series (printed with permission from the Mayfield Clinic).
Quantification of DNA Lost from CCDs during Microcatheter Transit
Relative to the estimated total DNA per CCD in positive controls, microcatheter transit caused less than 5% DNA loss from all devices examined. Cell retention was greatest for ascorbate coculture modified CCDs, followed by control CCDs. Differences in cell retention compared with the control CCDs were significant for ascorbate coculture (P = .005).
Regional Cell Migration from CCDs after Microcatheter Transit
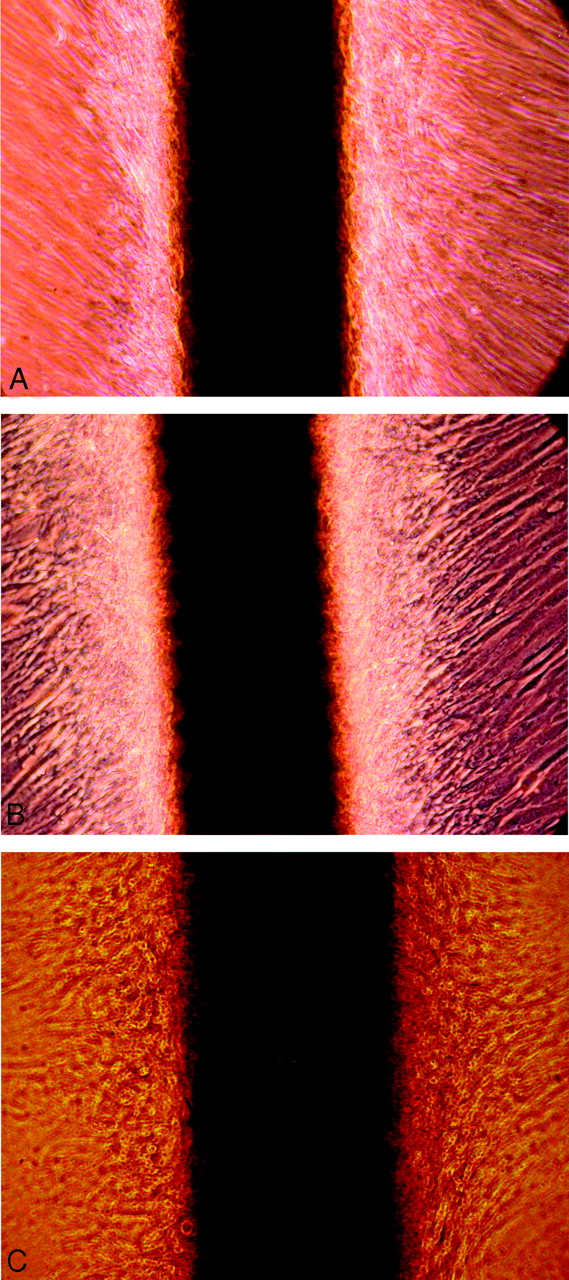
The CCDs modified by glutaraldehyde cross-linking (0.3% × 2 minutes and 1% × 10 seconds) demonstrated no cell migration. In contrast, the control CCDs and CCDs modified by ascorbate coculture or extended CMGC demonstrated cell migration with confluent cell growth after 3 days (Fig 6); results were identical in duplicate trials.

Regional cell migration from cell carrier devices (CCDs) after microcatheter transit. Photomicrographs of unmodified and modified CCDs recovered from microcatheter transit and incubated in culture medium for 3 days. Regional cell growth has reached confluence for control CCDs (A), and CCDs modified by ascorbate coculture (B) or extended CMGC (C). (printed with permission from the Mayfield Clinic).
Discussion
Adaptation of Cell Therapy to Repair of Aneurysms
This study lays the foundations for adaptation of endovascular cell therapy to microcoil-microcatheter technology (outer diameter ≤1 mm). Compared with other agents, detachable microcoils have several unique and indispensable advantages, including radio-opacity, anchorage, positional stability, remote tactile feedback, and retrievability. Although efficient microcatheter delivery of functional cells with particle-type embolization devices has been reported, adaptation of cell therapy to endovascular repair of aneurysms requires devices that can be delivered with more precise spatial and temporal control.18
Platinum microcoils with fibroblasts cultured on their surface have been used to successfully deliver cells to experimental aneurysms with prolonged survival of implanted cells.14 Although the efficacy of cell delivery with this simple construction device has been shown, we believe that a bioengineered coil design can improve the efficiency of cell delivery. Studies have shown that fibroblasts grown on microcoils are loosely associated with the coil, and only cells trapped inside the coil or residing in troughs between coil loops are effectively retained after microcatheter transit.14 This limits the efficiency of cell delivery and may create an unnecessarily large burden of embolic debris.
Role of CMGC in Stability of the Devices
In previous studies, microcoils with fibroblasts cultured directly on their surface were stripped of cells on the outer surfaces during passage through microcatheters or plastic housing assemblies.13,14 In contrast, the CCDs in our study remained intact after microcatheter transit. The ability of CCDs to withstand the stress of microcatheter transit and remain intact largely depends on the gel strengthening effect of CMGC because CFDs do not retain gel after microcatheter transit. This conclusion is further supported by reduced particulate release by extended CMGC-modified CCDs during microcatheter transit. The only other gel modification to enhance gel strength and decrease particulate release during microcatheter transit was glutaraldehyde cross-linking. This beneficial effect was counterbalanced by a negative effect on cell viability. The negative effect of glutaraldehyde cross-linking on cell viability was expected.21–23 This finding emphasizes that many modifications that enhance gel strength or viscoelasticity, or both, may not serve the ultimate goals of cell therapy.
Gel Stability and Liberation of Embolic Debris
Maintenance of structural integrity during microcatheter transit is an important requirement for clinically useful CCDs because liberated embolic debris could cause complications. Gel modifications shown to reduce this phenomenon include glutaraldehyde cross-linking and extended CMGC. The clinical significance of the levels of particulate release observed in this study is unknown. Similar levels of particulate release may occur during aneurysm embolization with use of microcoils modified with synthetic polymers (Matrix; Boston Scientific; HydroCoil; MicroVention). Further refinement of CCDs for clinical application may require greater reduction of particulate release.
Stability of the Devices versus Migratory Activity
Although glutaraldehyde cross-linking reduced debris released from CCDs during microcatheter transit, it significantly impaired migration of the cells, which may interfere with some mechanisms of cell therapy. In a model of endovascular cell therapy, implanted cells remain in the embolization vector and influence healing by release of mediators. Alternatively, implanted cells infiltrate the endoaneurysmal matrix and directly modify it. In the latter, effective cell therapy depends on migratory activity of implanted cells, and gel modifications that inhibit cell migration are detrimental. Because cell migration strongly depends on reorganization of the extracellular matrix by proteinases, the benefit of modifications that increase gel stability by inhibiting collagenases or creating intermolecular crosslinks may be counterbalanced by impaired cell migration.24–26
Effect of Microcatheter Transit on Cell Viability in CCDs
The undetectable effect of microcatheter transit on cell viability in this study contrasts with the results of previous studies with alginate microspheres.18,27 Examinations of live and dead cells may not have revealed areas of cell death in CCDs recovered from microcatheter transit because cell death was restricted to the most superficial layers of the collagen gel; these layers were denuded in the process of microcatheter transit. Evidence for loss of cells or cellular material from CCDs during microcatheter transit is found in the results of our DNA assays.
Theoretic Disadvantages of Collagen Gel-Based Devices
The collagen gel of CCDs increases their contact surface area, stiffness, and susceptibility to fragmentation. To be clinically useful, microcoils must advance through microcatheters with minimal friction, exit the tip of the microcatheter atraumatically, and fold easily to fill the sac of an aneurysm. Folding of CCDs within the lumen of an aneurysm may cause gel cracking, fragmentation, and embolization. Retrieval and repositioning of microcoils during embolization of an aneurysm are frequently performed and are often essential. CCD gels may not be stable to such manipulation.
Gel modifications that increase viscoelasticity and decrease stiffness may overcome these problems. Embolization devices on the basis of the association of platinum microcoils with acrylic polymer gels (HydroCoil) are currently used in clinical cases of treatment of cerebral aneurysms.28 Some acrylic gels have been successfully used to encapsulate cells.29 Further investigation is needed to determine whether acrylic gels will provide a suitable matrix for cell growth, cell delivery, and cell migration while retaining the technical performance characteristics needed for embolization of an aneurysm.
Our study focused on collagen gels because these materials have been thoroughly characterized as tissue engineering matrices, and embolization coils modified with collagen have enhanced endoaneurysmal healing in animal studies.6–8,10,16,30–32
Limitations of the Study
One theoretic advantage of the bioengineered coil design is that it limits cell loss during microcatheter transit. Because we did not use coils with cells cultured directly on their surface as a control group, the efficiency of cell delivery of the bioengineered design was compared with historical controls. In future studies, quantitative differences in cell retention between bioengineered coils and coils with cells cultured directly on their surface should be assessed to demonstrate this advantage of a bioactive coil design more clearly.
The method of microcoil deployment used in our study involved pushing the microcoils through the microcatheters with a fluid column under pressure. This method was used to minimize coil-microcatheter friction, which precluded the possibility of the pusher device over-riding the coil in the microcatheter and disrupting the coil-collagen gel association. Although this method has been used previously for transcatheter cell delivery with microcoils, it differs markedly from the method used in the clinical endovascular repair of cerebral aneurysms.12 Clinical methods, which involve advancing a microcoil through a microcatheter with a pusher wire, may disrupt the microcoil-gel association in CCDs more so than the pressurized fluid column method we used. Because our investigational method of microcoil delivery was neither sufficiently controlled nor reversible for clinical application, future evaluation of CCDs should focus on the effects of clinically used mechanisms of deployment.
Practical Applications
We have demonstrated that a bioengineered platinum microcoil-collagen gel complex can efficiently deliver functional fibroblasts through a microcatheter conduit. This technology may empower endovascular devices for the treatment of cerebral aneurysms with the advantages of cell therapy. On the basis of experimental studies, cell therapy has the potential to promote aneurysm healing and increase the probability of cure by endovascular means.11,12,14 Although our study focused on the engineering of suitable delivery systems, the future of cell therapy for intracranial aneurysms will depend on its benefits for promoting healing of the aneurysm and preventing recurrence. Proof of this benefit will require animal studies (eg, canine terminal bifurcation vein pouch model) with use of models that have a high frequency of aneurysmal recanalization after embolization of the coil.33
In consideration of immunologic issues, there are numerous potential approaches to cell therapy for aneurysms. Therapies may be based on the implantation of autologous cells or allogeneic cells (differentiated cells, mesenchymal stem cells from adult bone marrow or fat, and embryonic stem cells). In the case of autologous cells, issues of immune rejection are avoided. However, significant complexities in manufacturing and the time for preparation of devices containing autologous cells may limit access to elective therapeutic procedures planned far in advance. In the case of stem cells, issues of immune rejection are not avoided because even these cells will presumably differentiate at the implantation site.34 Although in vitro work suggests that mesenchymal stem cells are nonimmunogenic even after differentiation, there is no in vivo evidence that these cells persist after transplantation into a fully immunocompetent host.35 The undifferentiated state of stem cells, whether transient or persistent, theoretically brings with it an added risk of tumorigenesis.36 Furthermore, stem cell resources are limited, and significant ethical controversies exist regarding the use of human embryonic tissue. The viability of transplanted allogeneic fibroblasts in the absence of immunosuppression or immune-isolation is controversial. Although survival of human skin allografts in the nonimmunosuppressed host has been reported, some authors37 have suggested that donor skin cells are destroyed by immune effector cells and replaced by host cells in those cases. Although some evidence indicates that allogeneic fibroblasts are immunogenic and stimulate proliferation of peripheral blood mononuclear cells, animal studies38,39 have demonstrated that they remain viable for at least 3 weeks after transplantation. Immune-isolation cell encapsulation is an alternative solution to the problem of immune rejection.40 Because this approach is based on entrapment of cells in bioartificial implants that shield them from the host immune system, therapeutic efficacy will likely be limited to therapeutic paradigms in which the implanted cells influence healing of aneurysms by the release of mediators.
The clinical evolution of cell-based therapies for the treatment of human disease is an ongoing process that faces challenges of safety and efficacy. Complex implants composed of metallic vectors (platinum microcoil or stent), biomolecular hydrogels (collagen), and living cells must be evaluated as medical devices, biologic products, and transplantable tissues.41 Many of these challenges have been recognized by federal regulatory agencies such as the Food and Drug Administration (FDA), in which guidelines for evaluation of cell therapies are being developed at its Center for Biologics Evaluation and Research. FDA-approved autologous cell therapy systems in which a patient's own cultured cells are used to repair defects of articular cartilage (Carticel) and burn wounds (Epicel) are currently marketed by Genzyme Biosurgery (Cambridge, Mass). FDA-approved tissue-engineered implants that contain allogeneic human fibroblasts are currently marketed for certain types of clinical wound repair (Apligraft; Organogenesis, Canton, Mass, and Dermagraft; Smith and Nephew, London, United Kingdom).42,43
Unlike traditional pharmaceuticals, cell-based therapies must meet a unique set of manufacturing and distribution requirements that comply with federal regulatory standards and accommodate their limited biologic shelf life. Cell therapy products must be rigorously assessed to exclude the presence of transmissible agents, whereas manufacturing standards must ensure product sterility and therapeutic potency. Implanted cells must also be evaluated for tumorigenic potential and the ability to produce harmful or nonessential products. These end points may change over time and space (location of cell implantation) for a given donor cell line and vary significantly from 1 donor cell line to another. Furthermore, the delivery implant and its contents may also have variable effects on these end points.
The complexity of regulatory hurdles that new technologies of cell therapy must address may prove to be too costly for medical device companies. Nevertheless, there are many examples of cell therapy technologies in industry-sponsored clinical trials today. Notable examples include injectable gels that contain cultured mesenchymal stem cells for regeneration of periodontal tissue (Osteogenesis, Chuo-ku Kobe, Japan), intramyocardial stem cell injections for chronic myocardial ischemia (Baxter Healthcare, Deerfield, Ill), carrier vehicles loaded with mesenchymal stem cells for the treatment of distal tibial fractures (Teva Pharmaceuticals, Petach Tikva, Israel), and retinal pigment epithelial cells for the treatment of Parkinson disease (Titan Pharmaceuticals, South San Francisco, Calif).44–47
Conclusions
In this study, bioengineered devices consisting of collagen gels associated with platinum microcoils efficiently mediated transmicrocatheter delivery of functional fibroblasts without extensive liberation of debris. After microcatheter transit, migrations of cells from these devices proceeded readily. CMGC plays a necessary role in the process of gel stabilization that enables successful microcatheter transit. Although glutaraldehyde cross-linking, ascorbate coculture, and extended CMGC enhanced the gel stabilization process, only glutaraldehyde cross-linking compromised cell viability and migratory potential. Further development of CCDs should emphasize modifications of the gel that increase flexibility, elasticity, and coherence without compromising cell viability or migratory potential.
Footnotes
This study was funded by a grant from the Emory University/Georgia Institute of Technology Biomedical Research Center.
References
- Received October 23, 2006.
- Accepted after revision January 23, 2007.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}