
Abstract
BACKGROUND AND PURPOSE: Embolization of meningiomas has emerged as a preoperative adjuvant therapy that has proved effective in mitigating blood loss during surgical resection. Arterial supply to these tumors is typically identified by diffuse areas of parenchymal staining after selective x-ray angiograms. We investigate the benefits that selective injection of MR contrast may have in identifying vascular territories and determining the effects of embolization therapy.
MATERIALS AND METHODS: Selective intra-arterial (IA) injection of dilute MR contrast media was used to assess the vascular distribution territories of meningeal tumors before and after embolization therapy. Regions of the tumor that experienced loss of signal intensity after localized contrast injections into the external and common carotid as well as vertebral arteries were used to quantify the specific vessel's volume of distribution. Assessments were made before and after embolization to reveal changes in the vascular supply of the tumor. MR findings were compared with radiographic evaluation of tumor vascular supply on the basis of conventional x-ray angiography.
RESULTS: MR proved to be an excellent means to assess tissue fed by selected arteries and clearly demonstrated the treated and untreated portions of the neoplasm after therapy. In some instances, MR revealed postembolization residual enhancement of the tumor that was difficult to appreciate on x-ray angiograms. Very low contrast dose was necessary, which made repeated assessment during therapy practical.
CONCLUSION: MR perfusion imaging with selective IA injection of dilute contrast can reveal the distribution territory of vessels. Changes in tumor vasculature could be detected after embolization, which reveal the volumetric fraction of the tumor affected by the therapy.
Meningiomas are highly vascular brain neoplasms that are often associated with substantial blood loss during surgical resection. Embolization of meningeal tumors1,2 has emerged as a preoperative adjuvant therapy that has proved to be particularly effective in mitigating blood loss during surgical resection.3,4 Embolization involves selective micro-catheterization of arteries feeding the neoplasm and subsequent injection of microspheres5,6 or other embolic agents. The vascular bed of a meningioma is identified with conventional angiography by the presence of parenchymal staining after super-selective intra-arterial (IA) contrast injections. Embolization therapy is not appropriate for all arteries because of the potential for unintended ischemia in nonneoplastic tissue. Determination of whether embolization will be appropriate is based on a complete angiographic assessment of the neurovasculature. Neurologic deficits have been reported after embolization,7 presumably as a result of improperly identified vascular territories, reflux of embolic agents, or tumor swelling after embolization.
Dynamic susceptibility contrast (DSC) perfusion imaging8 is an MR technique that has primarily been applied to the categorization of stroke9 but also can provide useful information about neoplasms.10 DSC perfusion studies are performed with systemic administration of a paramagnetic gadolinium-based chelate through intravenous (IV) access. This method is convenient and minimally invasive, but quantitation is challenging partly because of difficulties in determining the arterial input function (AIF).11 Moreover, the volume of contrast agent used to elicit a substantial response is typically double the recommended dosage, making repeated measures undesirable. IA contrast administration would have several potential advantages, including the ability to visualize the distribution territory of the vessel, decreased broadening of the AIF, and dramatically reduced volumes of contrast agent for effects comparable to IV studies.
This feasibility study explores the possible benefits of MR guidance in embolization of meningiomas. It is specifically hypothesized that DSC perfusion imaging during selective injection of MR contrast media may offer better definition of arterial distribution territories with respect to the lesion and surrounding structures. A combined x-ray fluoroscopy/MR suite is used to augment conventional practices of meningioma embolization with selective IA DSC perfusion MR data.
Patients and Techniques
Patients
A total of 6 patients undergoing embolization of a meningioma before surgical resection were studied. The local Institutional Review Board and the Cancer Center Oversight Committee approved the study protocol, and patients provided informed consent. Patients ranged in age from 36 to 65 years (mean, 49 years) and included 4 women and 2 men. All patients underwent a conventional cerebral angiogram with subsequent embolization dependent on whether this adjuvant therapy was deemed potentially efficacious on the basis of the x-ray angiographic findings. Baseline MR acquisitions were performed the day before catheterization in all patients, and IA MR perfusion imaging was performed immediately before and after the delivery of embolic agents.
Combined X-Ray and MR Suite
We performed angiographic assessment, embolization of the meningiomas, and MR imaging in a combined “XMR” suite consisting of an x-ray catheterization laboratory (Integris V5000; Philips, Best, the Netherlands) and adjacent MR scanner (Intera; Philips). The 2 units can be connected, which enabled rapid transfer of the patients via a tabletop that floated between the 2 systems. The x-ray system was single plane with a 12-inch image intensifier. The MR system was 1.5T and equipped with 30 mT/m amplitude and 150 mT/m/ms slew rate gradients.
MR before Catheterization
An 8-element phased array head coil was used for all MR imaging before the procedure. The patients were positioned supine, and IV access was obtained.
Conventional MR Acquisitions
MR imaging performed the day before embolization included diffusion-weighted imaging (DWI; TR/TE/flip angle, 3749 ms/81 ms/90°; epi factor, 77; b-value, 1000 s/mm2; FOV, 24 cm; matrix, 128 × 77; sections, 24–5 mm; number of signal intensity averages [NSA], 3; axial plane; acquisition time, 48 s), turbo-fluid-attenuated inversion recovery (FLAIR) (TR/TE/TI/flip angle, 11000 ms/140 ms/2800 ms/90°; turbo factor, 47; FOV, 22 cm; rFOV, 75%; matrix, 256 × 179; sections, 30–5 mm; NSA, 2; axial plane; acquisition time, 3 min 18 s), and precontrast and postcontrast T1-weighted acquisitions (T1; TR/TE/flip angle, 511 ms/12 ms/90°; FOV, 22 cm; matrix, 256 × 205; sections, 24–3 mm; NSA, 2; axial plane; acquisition time, 2 min 38 s). IV perfusion, as described below, was also performed as part of this preintervention assessment.
Perfusion Imaging
Perfusion-weighted DSC imaging was performed with a single-shot echo-planar T2*-weighted acquisition (TR/TE/flip angle, 2000 ms/50 ms/90°; epi factor, 89; FOV, 24 cm; matrix, 128 × 89; sections, 12–5 mm; number of dynamics, 60; axial plane; acquisition time, 2 min 6 s). The acquisition was designed to acquire a minimum of 20 seconds of baseline data before arrival of contrast and to continue for approximately 1 minute after arrival. Gadolinium-based contrast (Omniscan; GE Healthcare, Princeton, NJ) was injected intravenously, either through an antecubital or hand vein. IV injections commenced 10 seconds after the start of the first dynamic scan to permit the acquisition of baseline data. Contrast was injected at either 4 mL/s (antecubital) or 3 mL/s (hand) to a dose of 0.2 mmol/kg (typically ∼20 mL). The contrast was followed by a 15-mL saline push at the same injection rate.
Angiographic Procedure
All patients received 2000 units of heparin via IV injection before the procedure to reduce the risk of clot formation. Vascular access was achieved with a transfemoral approach by the Seldinger technique. Vascular anatomy was determined by digital subtraction angiography (DSA) in combination with selective injection of iodinated contrast into the external and internal carotid arteries as well as into the vertebral arteries. This was performed bilaterally for all patients, irrespective of the location of the meningioma. Superselective angiograms of vessels such as the middle meningeal artery were performed as warranted by these initial findings. The interventional radiologists (R.H., V.H., C.F.D.) then established a qualitative assessment of their impression of fractional contributions of all vessels feeding the tumor. This assessment was done without knowledge of MR findings.
Embolization was performed in patients who demonstrated substantial tumor vascular supply through dural branches arising from either the external carotid or vertebral arteries in which a safe distal position of the catheter was achievable. Patients who were receiving embolization had an MR-compatible unbraided 5F catheter (Cook, Bloomington, Ind) placed into the vessel, through which the therapy was to be delivered. They were then transferred to the MR suite for IA MR perfusion imaging. Details of this imaging will be described below. After MR imaging, the patients were returned to the angiography suite for administration of therapy. Embosphere (BioSphere Medical, Rockland, Mass) was used as the embolic agent, and particle sizes ranged from 300 to 500 μ. A microcatheter was inserted into vessels that were associated with the tumor and appropriate for therapy. Embolization was administered until tumor parenchymal staining was obliterated. After completion of the embolization, the MR-compatible 5F catheter was returned to the same position used for preembolization therapy. The patients were then moved back to the MR suite for repeat IA MR perfusion imaging. After MR imaging, the patients were returned to the angiography suite.
Intra-Arterial MR Perfusion
To preclude the need for movement of patients during catheterization, a 2-element surface coil array consisting of two 20-cm circular loops was applied for all IA imaging. These coils were placed laterally against the patient's head and secured in place with tape. IA contrast injections were performed with dilute contrast. The contrast agent was diluted in physiologic saline to 0.05 mol/L (1/10 stock strength) for all studies. IA injections were performed through a catheter preloaded with the appropriate solution; injection rates varied between 1.0 mL/s (external carotid artery [ECA] and vertebral) and 3.0 mL/s (common carotid artery [CCA]). No saline push was necessary because the solution was released directly into the artery. A 5-second duration of injection was maintained to provide a bolus width comparable with IV injections and in balance with the temporal resolution of the whole-brain perfusion acquisition (2 s). These injection rates are also comparable with, but less than, those used for x-ray angiographic purposes. IA injections commenced 20 seconds after the start of the first dynamic scan because there was very little delay between injection and arrival of the contrast agent in the distal tissues. Patients receiving therapy via the ECA had perfusion scans performed in both the ECA and, subsequently, in the CCA. This was accomplished by initially placing the catheter in the ECA and then blindly retracting the catheter approximately 5 cm to enter the CCA.
Perfusion Analysis
Perfusion image data were fit to a standard gamma variate function on a pixel-by-pixel basis, and the following parameters were extracted: relative cerebral blood volume (rCBV), mean transit time (MTT), time to arrival (T0), and time to peak (TTP). The volume of tumor experiencing alteration in signal intensity during bolus passage was also quantified before and after embolization. We performed region-of-interest analysis on the tumors by dividing the lesion into the ECA, ICA, and whole-tumor sections. We obtained ECA territories on the IA ECA perfusion study and demarcated them from the image demonstrating peak signal intensity attenuation as well as from the calculated perfusion maps. The region of interest circumscribed the entire territory experiencing loss of signal intensity on the first pass of the contrast agent. These regions of interest were then copied to the CCA perfusion study, and the ICA territory was defined as the region of tumor experiencing signal intensity attenuation but external to the defined ECA territory. Finally, we copied the ECA and ICA territories to the IV study to investigate differences in perfusion properties of the ECA and ICA territories against the whole tumor. The IA segmentations were repeated after embolization to determine the effectiveness of the therapy and compared with changes evident on selective x-ray angiographic runs. All volumes were measured by an imaging scientist (A.J.M.) without knowledge of the radiologists’ impressions of the fractional contribution of vessels.
Results
All patients received preintervention MR assessment including IV perfusion. Any patient experiencing even a mild reaction to IV injection of gadolinium-based contrast would have been excluded from further study, but this did not occur. One patient was not considered a good candidate for embolization therapy at the time of catheterization because of the predominant tumor supply coming from the internal carotid artery. This patient did not undergo any additional MR examinations. The remaining 5 patients received embolization therapy and additional MR examinations including IA DSC perfusion.
Embolization was performed via a distal branch of the ECA (4/5) or vertebral artery (1/5) in all patients. One patient exhibited reflux into the ICA during an ECA injection and was excluded from further analysis. The IA injection rates were set to be compared with, but less than, those used for conventional angiography. The purpose of this strategy was to minimize the potential for streamlining effects and avoid reflux in any vessel. In this study, we used an injection rate of 3 mL/s into the common carotid artery and 1 mL/s into the external or vertebral arteries. Concentration of the injectate was initially estimated based on the anticipated flow in the carotid (5% to 6%) and vertebral (∼2%) arteries12 as a fraction of cardiac output (assumed to be ∼5 L/min). Therefore, an IV-injected bolus is anticipated to deliver the indicated fraction of the injectate to the corresponding territory. The prescribed injection rates were further anticipated to result in approximately a 1:1 dilution of the injectate in blood. Thus, to approximate arterial concentrations similar to those obtained with IV injections, we diluted the injected gadolinium solution to 1 part contrast in 9 parts saline (0.05 mol/L). This amount was initially tested in a set of 4 patients who received only postembolization IA perfusion imaging and proved to be a reasonable compromise. Therefore, each ECA and CCA perfusion scan requires only 2.5% and 7.5%, respectively, of the contrast used in conventional IV perfusion to create a similar effect.
Patient Findings
Patient 1.
This patient (Fig 1) had a large right posterior meningioma that was determined on angiograms to have a significant pial supply. On the basis of complete angiographic evaluation, radiographic impression estimated that the right ICA contributed 85% of tumor blood supply, with the right ECA contributing the remainder. Superselective embolization of the right middle meningeal artery was performed, resulting in angiographically determined complete stasis. IA MR perfusion imaging was performed through the right external and common carotid arteries before and after embolization. ECA injections revealed the portion of the tumor associated with the vessel before embolization. The lack of changes in signal intensity after embolization supports the angiographic finding of obliteration of nonpial supply to this tumor.
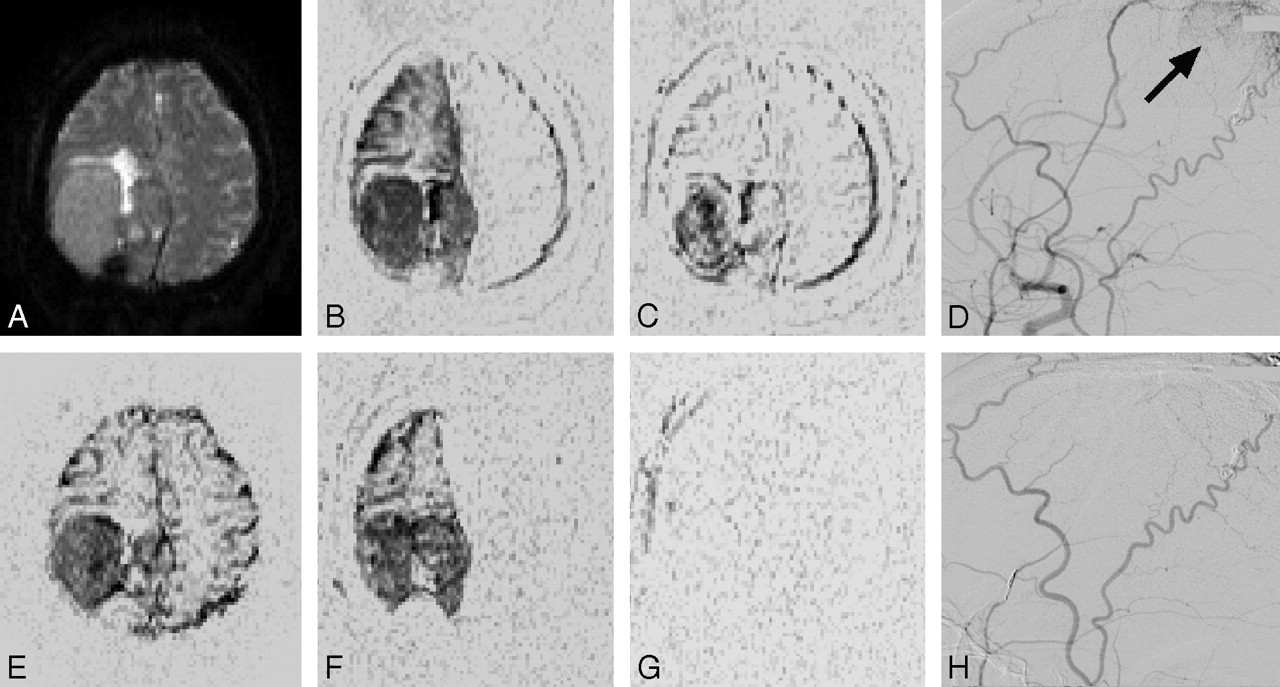
Patient 1. This large right temporal meningioma was treated via embolization of the right middle meningeal artery. Perfusion MR images and x-ray angiograms are shown before (A–E) and after (F–H) embolization. The baseline MR perfusion image (A) reveals the tumor before administration of contrast. Difference images between this baseline and peak signal intensity attenuation after IV (E), IA CCA (B, F), and IA ECA (C, G) contrast injection are also shown. The ECA injection images reveal the portion of the tumor fed by this vessel before (C) and after (G) embolization. The x-ray angiograms were obtained with an ECA injection and revealed characteristic tumor blush (arrow) originating from the middle meningeal artery. The delivery of embolic agents through this vessel successfully obliterated this portion of the tumor vascular supply, which can be appreciated with both MR (G) and x-ray (H).
Patient 2.
This patient had a large meningioma in the right posterior cranial fossa (Fig 2). A complete angiographic assessment led to a radiographic impression of blood supply from the following arteries: the right vertebral (50%), left vertebral (30%), right external carotid (15%), and left occipital (5%). Superselective embolization was performed via the right and left posterior meningeal arteries and resulted in a marked reduction of flow. There was residual supply from the right posterior inferior cerebellar artery (PICA) as well as the untreated right external carotid and left occipital arteries. MR perfusion imaging was performed via the right vertebral artery and revealed the portion of the tumor fed by this vessel before and after embolization. The residual enhancement after embolization likely reveals the distribution territory of the untreated right PICA.

Patient 2. A large meningioma in the posterior fossa is evident on precontrast MR perfusion (A). Difference images between this baseline and peak signal intensity attenuation after IV (D) and IA right vertebral (B) contrast injection are shown. Selective x-ray angiograms obtained during a right vertebral injection reveal the pattern of the tumor (C). Embolization was administered more distally to this injection site (right posterior meningeal), and obliteration of the posterior component of the right vertebral distribution territory can be appreciated on the MR (E) and x-ray (F) images after embolization.
Patient 3.
This patient had a large right frontal meningioma (Fig 3). A complete angiographic assessment led to a radiographic impression of blood supply from the following arteries: the right ECA (75%), right ICA (15%), and left ECA (10%). Superselective embolization was performed via the right and left middle meningeal arteries and produced a good angiographic result. IA MR perfusion imaging was performed through the right external and common carotid arteries before and after embolization. This revealed substantial involvement of the tumor in the right ECA before embolization, which was markedly reduced after treatment. However, MR perfusion provided evidence of residual supply from this artery after embolization that was difficult to appreciate on the postembolization right ECA angiographic run.

Patient 3. The figure summarizes the effects of embolization of a large right frontal meningioma. The upper row depicts the lesion before embolization and includes a precontrast perfusion source image (A), perfusion difference images between baseline and peak enhancement after right CCA (B) and ECA (C) injection, and a lateral view x-ray angiogram with a right ECA injection (D). Preembolization peak perfusion contrast after IV contrast administration is revealed (E). After embolization, the CCA (F) and ECA (G) perfusion studies and lateral view x-ray angiogram with a right ECA injection were repeated. Contrast injection into the right ECA demonstrates some residual attenuation (G) but is substantially reduced compared with the baseline state. The blush pattern in the proximity of the lesion that was evident on x-ray angiograms is no longer appreciable after treatment (H).
Patient 4.
This patient had a large meningioma in the posterior right parietal-occipital lobe that was heavily calcified. A complete angiographic assessment led to a radiographic impression of blood supply from the following arteries: the left occipital (70%), left ECA (20%), and right ECA (10%). Superselective embolization of the left and right middle meningeal arteries was performed with a good angiographic result. Heavy calcification produced signal intensity void on MR perfusion images that encompassed 85% of the volume of the tumor. The signal intensity void precluded assessment of bolus passage in this portion of the tumor, which greatly limited the information obtained from MR perfusion. IA MR perfusion was performed through the left ECA, and evidence of bolus passage was evident on MR-visible portions of the tumor. Changes in signal intensity during bolus passage were not evident after embolization, consistent with a good angiographic result in this territory.
Perfusion Analysis
IA assessments before and after embolization provide insight into the portion of tumor affected by embolization therapy. Table 1 summarizes tumor vascularity on the basis of angiographic impression and MR perfusion imaging. Tumor volume was established from IV perfusion data acquired the day before embolization. X-ray data in this table are based on qualitative radiologic impressions of all vessels involved with the tumor but binned into the coarser arterial distributions assessed with IA MR techniques. The portion of the tumor fed by a specific vessel was quantitatively evaluated before and after embolization with IA MR perfusion methods. This was possible in only a limited subset of vessels, and vessels not interrogated by MR were marked with a dash. There were substantial differences in the portion of the tumor predicted to be fed by a specific artery, on the basis of angiographic impression versus MR perfusion. Many factors may affect these differences. For example, the MR-determined distribution territory of a vessel does not exclude that other vessels may also feed portions of this same region. The spatial extent of the region of signal intensity attenuation after selective ECA or vertebral injection was reduced in all patients after embolization. The tissue affected by embolization can be delineated by the region that experiences signal intensity attenuation with selective injection before, but not after, therapy. The effectiveness of embolization is reflected in the reduced fraction of the tumor volume associated with the vessel through which embolic agents were administered.
Arterial involvement with tumor
Perfusion analysis was performed on all IV and IA contrast injections (Table 2). Patient 4 was excluded from this Table because the portion of the tumor that provided some signal intensity still provided substantially less than normal tissue. Therefore, extraction of meaningful contrast dynamics was severely compromised. For the remaining patients, whole tumor assessments were determined from IV injections because several tumors were at least partially fed by contralateral circulation or a combination of carotid and vertebral sources. Thus, injection into the CCA would not necessarily highlight the entire lesion. Although the duration of injections was kept constant between the IV and IA techniques, the significant differences in bolus width and contrast concentration made direct comparison between these 2 groups difficult without improved techniques of quantitation. All relative measures of cerebral blood volume were normalized to the value obtained in white matter. Tabulated measures of ICA and ECA perfusion were extracted from the appropriate regions of interest on the CCA injection. rCBV within the lesion was substantially higher than the white matter in all patients. The white matter-normalized rCBV values increased in 2 patients after embolization. The significance of this finding is unclear because many factors in this study that were not controlled for (including cardiac output), could affect the arterial concentration of gadolinium. Thus, it is not clear whether this change was meaningful or reproducible.
Perfusion findings for vessels ipsilateral to lesion
MTT was an average of 18% shorter with IA delivery compared with IV techniques with identical duration of injections. This comparison is directly attributable to a broadening of the input function as the bolus moves from the IV injection site to the target tissue. The MTT through the portion of the lesion assigned as part of the ECA territory was, on average, 6% (IA measures) or 1.5% (IV measures) longer than the ICA territory. This discrepancy may be related to differences in the blood-brain barrier between these 2 vessels but does not seem sufficient to demonstrate appreciable contrast on MTT maps. There was a substantial elongation in the MTT for patient 2 after embolization; the cause of this is unknown. This prolongation also seems to be largely responsible for the higher rCBV measure noted in this patient after therapy.
Discussion
MR techniques have some significant advantages in their ability to correlate soft tissue with the vessels providing its vascular supply. The ability to independently visualize tumor and normal tissue in a volumetric sense, coupled with dynamic imaging during localized injections of contrast, provides a powerful enhancement over the x-ray angiographic techniques that are currently used. The improved visualization of where a contrast agent is deposited after superselective contrast injection can allow a more complete embolization of tumors without increasing the risk to nonneoplastic tissue. These data should provide a more detailed preoperative map of tumor vascularity compared with conventional imaging techniques and, by identifying regions of persistent hypervascularity, provide a target for further embolization or a map of sites of potentially significant intraoperative bleeding. The potential of embolizing meningiomas without subsequent surgery has already been proposed,13 and this should only become more appropriate with better definition of vascular territories. Moreover, it is not unreasonable to expect that an increasing number of asymptomatic meningiomas will be discovered as a result of unrelated diagnostic procedures. This is because the prevalence of meningiomas at autopsy14 is substantially greater than that in current clinical incidence. The increasing use of MR and CT to evaluate an assortment of unrelated conditions should increasingly reveal meningiomas at an earlier stage, when minimally invasive therapy may be more appropriate.
The principal limitation of MR in the evaluation of vascular territories is that it is currently impractical to manipulate catheters under MR guidance. This greatly limits the number of vessels whose vascular territory can be explored because the catheter manipulations must be made under x-ray guidance, requiring shuttling of patients between the MR and x-ray systems for each independent vessel selection. Moreover, there are safety concerns about the presence of braided catheters in patients during MR scanning. This concern relates to the conductive nature of the metallic braid that is virtually ubiquitous with clinically used neurovascular catheters. This braiding provides the necessary mechanical properties to navigate neurovascular structures but may cause localized hot spots when exposed to the radio-frequency energy of an MR system.15,16 Thus, we used an unbraided catheter in this study, which often required that the selected vessel be accessed initially with a conventional neurovascular catheter and then changed for the MR-compatible catheter by temporarily leaving a guidewire to maintain position. Evaluation of more distal vessels becomes increasingly difficult to access with MR-safe catheters. Therefore, we limited our injections to relatively proximal vessels. A simple blind pullback procedure proved effective at broadening the distribution territory within the MR scanner, but under ideal conditions branch vessels would be studied with independent injections. We are currently exploring the possibility of using braided catheters in these studies, given that the specific absorption rate associated with DSC perfusion imaging is extremely low.
Other potential methods can determine the vascular supply to meningeal tumors. A combination of conventional angiography and CT has been proposed.17 Placement of the catheter must again be performed in the catheterization laboratory, but CT evaluation of superselective injections provided more definite visualization of tumor perfusion in nearly half the cases studied. This benefit was largely because of the tomographic capabilities of the CT system, which revealed distribution territories beyond what could be appreciated with DSA. The heightened sensitivity of MR to the spatial extent of the tumor as well as the presence of contrast should only improve on these findings. However, all these methods require catheterization that may prove to be unnecessary if the evaluation of the tumor vasculature reveals that it is not amenable to embolization therapy. The use of arterial spin labeling methods18 to selectively label specific vessels19 is an intriguing idea that may provide a useful initial evaluation of tumor vasculature. This method could serve to screen out patients whose dominant supply is clearly from the ICA and potentially prevent catheterization without subsequent therapy. Improvements in the labeling specificity of these techniques will likely be necessary to realize this objective, however.
Not surprisingly, the benefit of embolization therapy is greatest when a high degree of tumor vascularity has been obliterated.20 Techniques that serve to improve the portion of tumors that can be embolized without affecting the surrounding tissue will only improve the efficacy of the technique. The interventional MR methods described here represent a step toward this goal and clearly demonstrate the correlation that can be achieved between tumor volume and vascular distribution territories.
Conclusions
Selective IA injection of dilute MR contrast media is an excellent means to assess the distribution territory of arteries feeding highly vascular lesions. Very low contrast dose is required, which makes repeated assessment during therapy practical. MR seems to be very sensitive for depicting tissue fed by a selected vessel and can also provide a volumetric assessment of both the tumor and distribution of vascular territories. These advantages, when coupled with conventional x-ray angiographic techniques, provide novel insight into tumor vascularity and the impact of embolic therapy.
References
- Received December 20, 2006.
- Accepted after revision February 11, 2007.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}