
Abstract
SUMMARY: We report the finding of restricted diffusion in an isolated abscess of the clivus and discuss the imaging differential diagnosis, with an emphasis on the usefulness of diffusion-weighted imaging.
The clivus is an uncommon location for intracranial lesions. Chordoma, chondrosarcoma, plasmocytoma, giant cell tumors, lymphangioma, adenocystic and nasopharyngeal carcinomas, and metastases are lesions known to develop in the clivus.1,2 Secondary clival involvement from sphenoid sinus abscesses and mucopyoceles have been reported and documented by CT and conventional MR imaging.3,4 We describe the diffusion-weighted imaging (DWI) findings of a primarily clival abscess.
Case Report
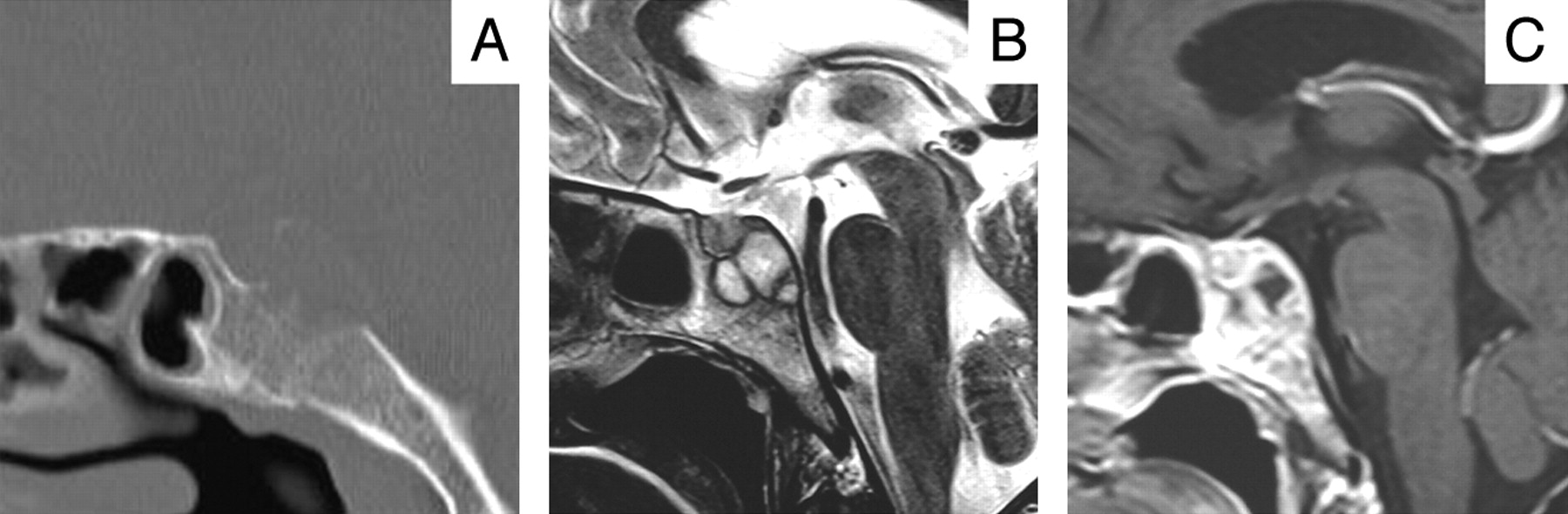
A 44-year-old woman presented with a 1-month history of progressively worsening hemifacial and hemicranial headaches, nausea, and vomiting. There were no visual complaints or previous history of sinusitis. At examination, the patient was awake and alert, afebrile, with no signs of meningeal irritation. Sensation in the face was intact. Hess screen chart examination revealed incomplete left sixth nerve palsy. CT showed a midline mass lesion with bone erosion, involving the upper clivus and sellar floor (Fig 1A). MR imaging (1.5T scanners, Symphony and Avanto; Siemens, Erlangen, Germany) demonstrated a cystic-necrotic lesion, with a hypointense rim on T2-weighted turbo spin-echo images and thick peripheral enhancement (Fig 1B, -C). DWI and apparent diffusion coefficient (ADC) maps demonstrated central restricted diffusion (Fig 2). DWI parameters were as follows: coronal plane, TR = 170 ms, TE = 94 ms, b = 1000 s/mm2, section thickness = 3 mm with a 0.5-mm gap, matrix = 218 × 256 ms, and FOV = 20.9 cm. Laboratory analysis failed to reveal leukocytosis (9.7 × 109/L), elevated C-reactive protein (5.3 mg/L), or increased tumor markers. No primary malignancy was detected on cervical, chest, abdominal, or pelvic CT. After 3 weeks of treatment with high-dose clindamycin and gentamicin without clinical improvement or imaging findings change, the patient underwent a pretemporal-transsylvian approach to the mass. A smoothened upper clivus due to an abscedated collection was found. No communication between the abscess and the sphenoid sinus was demonstrated. Pathologic examination revealed inflammatory cells but no organisms. Bacterial, mycobacterial, and fungal cultures were obtained, but no organism was cultured, presumably because of administered antibiotics. After surgery, there was resolution of the patient's complaints. Antibiotherapy was administered for another 4 weeks. Imaging follow-up at 3 months showed partial clival bone reconstitution.

A, A 2-mm section of sagittal CT reformation (bone window) shows destruction of the upper clivus and sellar floor. Only slight mucosal thickening is seen in the sphenoid sinus, and its bone walls are intact. B, Sagittal T2-weighted image reveals a moderately expansile cystic lesion with a peripheral low-signal-intensity rim. C, Sagittal postgadolinium T1-weighted image delineates the cystic or necrotic center and thick peripheral enhancement.

A, Oblique coronal DWI shows high signal intensity in the center of the clival lesion (white arrow). B, Apparent diffusion coefficient map demonstrates corresponding decreased signal intensity confirming restricted diffusion (black arrow).
Discussion
Infectious lesions of the clivus are rare, mainly arising from the sphenoid sinus. Sphenoid mucopyoceles can expand posteriorly, eroding the posterior wall of the sphenoid sinus, and present as a clival mass entrapped by sphenoidal mucosa. The wall defect can be demonstrated either by imaging or by surgery.3 Clival infection can also result from aggressive sphenoid sinusitis.4 Accurate preoperative diagnosis of infection is important, because transsphenoidal drainage would be considered the best approach, avoiding contamination of the CSF and providing a route for prolonged drainage of the infected area. In this case, diagnostic challenge was increased by the lack of contiguity between the lesion and sphenoid sinus on thin CT reformats and by the absence of significant sphenoid sinusitis. Therefore, we had to consider neoplasms in our differential diagnosis.
Clival metastases can present as destructive lesions, but the primary neoplasm is often known at the time of presentation.1 DWI is helpful in detecting lytic skull metastasis of the skull base.5 Lytic metastases are hyperintense on DWI because of the attenuated cell packing in highly malignant tumors and T2 shinethrough effect once they are typically hyperintense on T2-weighted imaging.5 The clival abscess presented as a cystic/necrotic mass lesion, which is atypical for a metastasis. In addition, DWI hyperintensity in this case was due to truly restricted diffusion, because the ADC map showed low signal intensity.
Clival chordoma and chondrosarcoma cause osteolysis, but bone CT usually also shows high attenuation foci. In chordoma, those foci represent fragments of destroyed clivus, whereas in chondrosarcoma they are due to chondroid matrix calcification.1,6 Additionally, chondrosarcoma more likely originate in the petrooccipital fissure. Plasmacytomas are typically homogeneous lytic masses, isointense to gray matter on T2-weighted images because of their dense cellularity.1 Giant cell tumor is more common in women in the third and fourth decades, presenting as an expansile mass surrounded by a low-signal-intensity incomplete cortical shell. Only 1 case of clival lymphangioma has been described,2 presenting high signal intensity on T1- and T2-weighted images. Chondrosarcoma typically shows high ADC values.7 The behavior of the remaining primary tumors of the clivus on DWI/ADC has not been addressed.
The use of DWI in skull base infection has not been reported previously, to our knowledge. As in brain abscesses, a possible explanation for restricted diffusion is that hypercellularity and the presence of macromolecules in pus reduce water diffusivity. Another similarity with brain parenchymal abscesses is the presence of a T2-hypointense rim due to paramagnetic free radicals.
Elsewhere, the usefulness of DWI in bone infection is controversial. Increased signal intensities on DWI have been reported, both in tuberculous and pyogenic spondylodiskitis.8 In contrast, increased tissue diffusivity in patients with aggressive osteomyelitis of the femur has been described.9
The origin of the osteomyelitic process is unclear: the patient's recent history did not include any sinus infection that could have spread to the clivus. Nevertheless, the sphenoid sinus remains the most likely origin of the organisms, because there were no other clinical or laboratory signs of systemic infection. We cannot exclude a secondary infection in a previously existing lesion, such as an ecchordosis physaliphora, an intradural posterior clival notochordal remnant found in 2% of random autopsies.10 Intradural chordoma, epidermoid, and dermoid cysts are less likely primary lesions, all of which occur at the same location as ecchordosis.11
Based on this case, the finding of a purely lytic, cystic-necrotic lesion of the clivus, with a T2-hypointense rim, peripheral enhancement, and central restricted diffusion is suggestive of an abscess, irrespective of the absence of clinical or laboratory signs of infection.
Acknowledgments
We thank Drs Jaime F. Rocha and Zita Magalhães (Department of Neuroradiology, Hospital de S. Marcos, Braga) and Dr José M. Dias-da-Costa (Department of Neuroradiology, Hospital de S. João, Porto).
Footnotes
Paper previously presented at: Fourth Congress of the Portuguese Society of Neuroradiology, June 29–30, 2007; Ponta Delgada, Azores, Portugal.
References
- Received July 18, 2007.
- Accepted after revision July 24, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.