
Abstract
SUMMARY: We report the unusual transformation of a lipomyelocele to a rhabdomyosarcoma in a 3-year-old boy. A lipomyelocele is not considered pre-malignant, but the possibility of developing such a tumor may represent another reason for close neurological follow-up in patients with spinal dysraphism.
Alipomyelocele is an intraspinal lipoma that is tightly attached to the dorsal surface of an open spinal cord.1 The spinal cord remains within the spinal canal unlike a lipomyelomeningocele, in which the thecal sac herniates through the spina bifida. Lipomyeloceles are associated with tethering of the cord but not with malignancy.2
Case Report
A spinal sonography was performed on the first day of life in a full-term neonate with a complex hemangioma over the sacrum (Fig 1). This showed the spinal cord ending in a sacral lipoma. The diagnosis of a lipomyelocele was confirmed by MR imaging at 3 months of age (Fig 2). The baby was managed conservatively with frequent neurosurgical assessment. At 3 years of age, he presented with an unwillingness to walk and general malaise. He had developed a large sacral bulge with a superimposed hematoma. Spinal MR imaging demonstrated a new large mass arising from the lipoma and distal spinal cord within the sacral canal (Fig 3A). There was surface enhancement of the cord (Fig 3B) and brain stem (Fig 3C) consistent with meningeal seeding of the tumor. These findings were confirmed at surgery, and pathologic examination of the partly excised tumor revealed a rhabdomyosarcoma. Histology showed a pleomorphic malignant spindle cell tumor (Fig 4) positive for muscle markers.

Photograph of a complex ulcerating hemangioma over the sacrum in a full-term neonate on day 1.

Sagittal T1-weighted MR image obtained at 3 months confirms the sonographic finding of the tethered spinal cord (arrowhead) ending in a lipomyelocele (arrow).

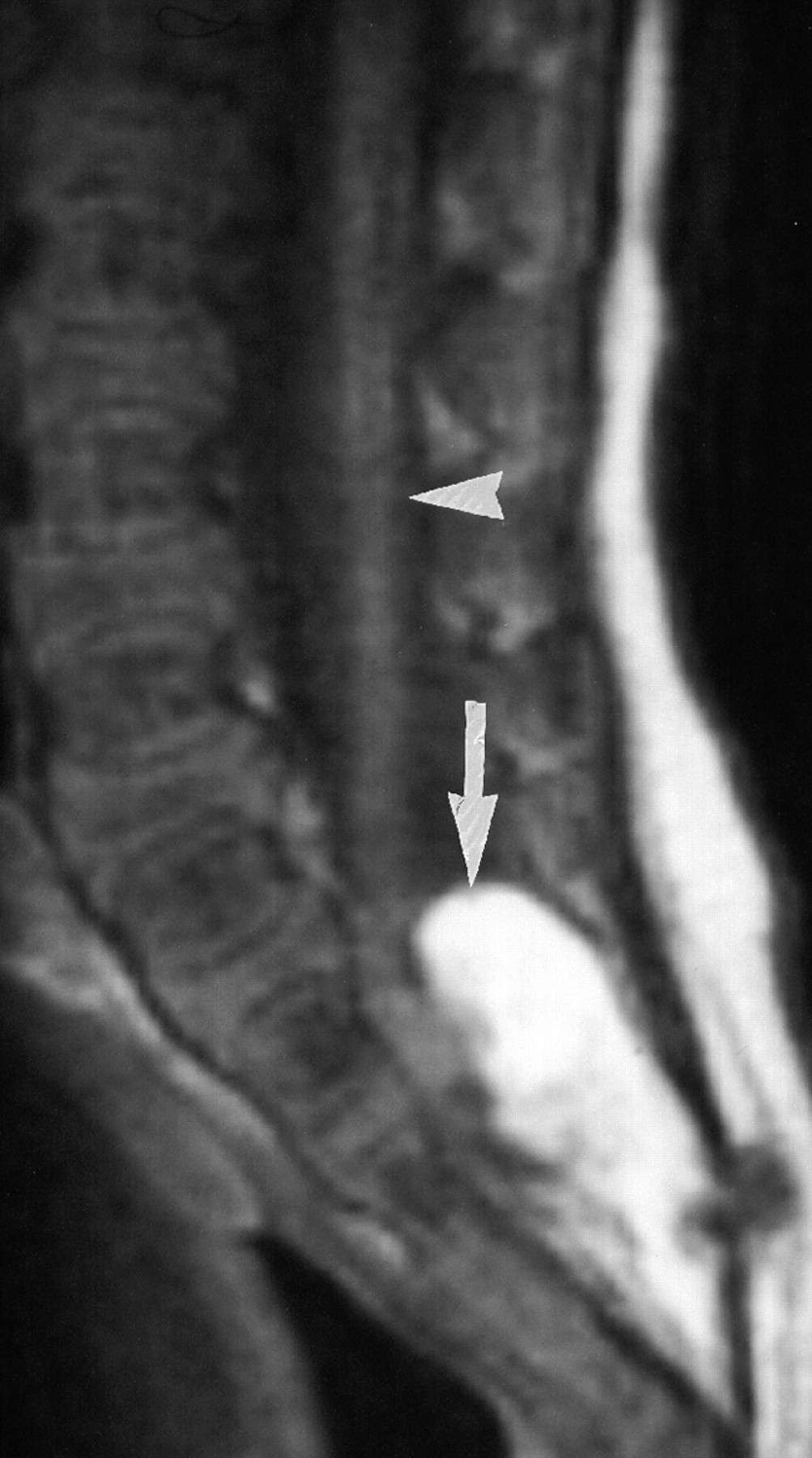
A, Sagittal T1-weighted MR image at 3 years shows a new large homogeneous mass of low signal intensity (arrow), apparently arising from the lipomyelocele and distal spinal cord within the spinal canal. B, Postcontrast T1-weighted sagittal MR image shows multiple foci (arrowheads) of high signal intensity in the distal thoracic and lumbar spinal cord consistent with metastatic seeding. C, Sagittal postcontrast T1-weighted MR image demonstrates multiple foci (arrowheads) of high signal intensity in the brain stem and cervical and upper thoracic spinal cord, consistent with metastatic seeding.

Resection of this sacral mass revealed a pleomorphic malignant spindle cell tumor at pathology, consistent with a rhabdomyosarcoma (hematoxylin-eosin).
Discussion
The clinical finding of sacrococcygeal cutaneous stigmata, such as that seen in this baby, has been clearly linked with occult spinal dysraphism. Screening spinal sonography is indicated in these babies, and positive findings can be confirmed by MR imaging. Management is usually conservative. Follow-up assessments are focused on the detection of any possible evidence of neurologic complications of the tethered cord and, in particular, of any sign of neurologic deterioration. Such findings may be indications for surgical untethering of the cord and resection of the lipoma.
The possibility of development of tumors in neural tube defects has been described.3–6 Lipomyeloceles are not, however, considered premalignant conditions. To our knowledge, the development of a rhabdomyosarcoma within a lipomyelocele has not been previously described. It has, however, been described originating from the central nervous system (CNS). There are no skeletal muscle cells in a lipomyelocele, but it is tightly attached to the dorsal aspect of the open spinal cord.
Primary intracranial rhabdomyosarcoma is a rare tumor in infancy and childhood, which is found in various locations in the CNS.7 The clinical course worsens rapidly, and the final outcome is poor, with a median survival time of 8–10 months.7 Invasion of the meninges, spontaneous intratumoral bleeding, spinal leptomeningeal CSF spreading of tumor cells, and early recurrence of the mass are the distinctive features of rhabdomyosarcoma.7
Intracranial rhabdomyosarcoma has also been described in association with subdural hematoma. The authors propose the possibility of sarcoma development secondary to chronic inflammation and proliferation in subdural collection.8 The coexistence in this instance seems coincidental, however, and subdural hematoma was known to be secondary to a fall.
The development of a rhabdomyosarcoma in this case report is likely embryonal. Although originating from a benign lesion such as a lipomyelocele has not been described previously, to our knowledge, unlike CNS origin, it may represent a very rare transformation.
The possibility of development of such a tumor, however rare, presents another reason for close neurologic follow-up of children with spinal dysraphism. It emphasizes the importance of early neuroimaging of the spinal canal when any new neurologic signs or symptoms develop.
- Received October 27, 2007.
- Accepted after revision October 31, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.