
Abstract
BACKGROUND AND PURPOSE: Elevated protein levels have been reported in perilymph of patients with vestibular schwannoma. Fluid-attenuated inversion recovery (FLAIR) imaging is sensitive to high protein contents in fluids. The purpose of this study was to investigate if in patients with unilateral vestibular schwannoma, cochlear FLAIR signal intensity on the affected side is increased compared with the unaffected side and control subjects.
Materials and METHODS: Fifteen patients with unilateral vestibular schwannoma and 25 age-matched control subjects (without a history of hearing loss) were retrospectively evaluated. All patients and controls had routine 5-mm FLAIR and T1- and T2-weighted imaging of the brain. The signal intensity of both cochleae was evaluated by placing a small region of interest on FLAIR images. The signal intensity of the brain stem was also determined by placing a second region of interest. A ratio of cochlear signal intensity to brain stem signal intensity (CIBI ratio) was determined. A t test was used to compare the CIBI ratios.
RESULTS: In patients, the mean CIBI ratio of the affected side was 0.89 ± 0.18, and that of the unaffected side was 0.57 ± 0.12. In control subjects, it was 0.51 ± 0.07. The CIBI ratio of the affected side was significantly higher compared with the unaffected side (P < .001) and compared with control subjects (P < .001).
CONCLUSION: Patients with vestibular schwannoma have increased cochlear FLAIR signal intensity on the affected side compared with the unaffected side and healthy subjects.
Elevated protein levels have been reported in cochlear perilymph of patients with vestibular schwannoma.1,2 In the past, labyrinthine tap was advocated as a diagnostic test to differentiate hearing loss caused by vestibular schwannoma from other causes of hearing loss.3 However, because of a small but definite associated risk of deafness, labyrinthine tap was infrequently performed and has since been completely abandoned due to widespread availability of MR imaging and CT for the evaluation of patients with hearing loss.4 Nevertheless, the pathogenesis and clinical implications of high perilymph protein in patients with vestibular schwannoma have remained unresolved.
Fluid-attenuated inversion recovery (FLAIR) images are sensitive in detecting high protein contents of fluids such as CSF.5 We hypothesized that increased protein content in cochlear perilymph of patients with vestibular schwannoma may be detectable by FLAIR imaging. We believe that detection of cochlear signal intensity changes by MR imaging may help in further determination of the pathogenesis and clinical value of perilymph protein levels in patients with vestibular schwannoma. The purpose of this study was to investigate if in patients with unilateral vestibular schwannoma, cochlear FLAIR signal intensity on the affected side is increased compared with the unaffected side and control subjects.
Methods
Subjects
Institutional review board approval was obtained for this retrospective study.
Fifteen consecutive patients with unilateral vestibular schwannoma who presented to our hospital for a 3-year period between 2003 and 2006 and 25 age-matched controls without hearing loss were included. Ten of the 15 patients had histopathologic confirmation of the diagnosis, and 5 were diagnosed on the basis of typical MR imaging appearances and went on to have gamma knife radiosurgery. Patients with prior surgery or those with a history of gamma knife radiosurgery were excluded if imaging before the therapy was not available. We selected a higher number of controls than patients to better validate our statistical analysis. The controls had head MR images for conditions such as headache, memory loss, transient ischemic attack, or stroke. None of the controls had hearing loss or posterior fossa symptoms, and none had clinically significant findings on their scans. Patients with prior cranial surgery or a history of meningitis, subarachnoid hemorrhage, or renal failure were excluded from the control group because these conditions may affect CSF or perilymph protein contents.
MR Imaging
Both patients and control subjects had FLAIR and T1-/T2-weighted imaging of the brain as part of their clinical imaging protocol performed on a 1.5T Symphony scanner (Siemens, Erlangen, Germany). FLAIR images were obtained with a TR = 9130 ms, TE = 122 ms, TI (time inversion) = 2500 ms, flip angle = 150°, section thickness/section gap = 5/0.5 mm, and matrix = 256 × 256 (reconstructed 512 × 512). Spin-echo T1-weighted images were obtained with a TR = 750 ms, TE = 14 ms, flip angle = 90°, section thickness/section gap = 5/1 mm, and matrix = 256 × 256. Turbo spin-echo T2-weighted images were obtained with a TR = 5400 ms, TE = 14 ms, section thickness/section gap = 5/0.5 mm, and matrix = 256 × 256 (reconstructed 512 × 512). An FOV of 23 cm2 was used for all the sequences. In addition, patients had T1-weighted focused pre- and postgadolinium axial images of the internal auditory canals (IACs) with a TR = 650 ms, TE = 17 ms, flip angle = 90°, thickness/section gap = 3/0.9 mm, matrix = 256 × 256, and 2 signal intensity averages. An FOV of 19 cm2 and flow compensation were used for focused IAC images.
Image Analysis
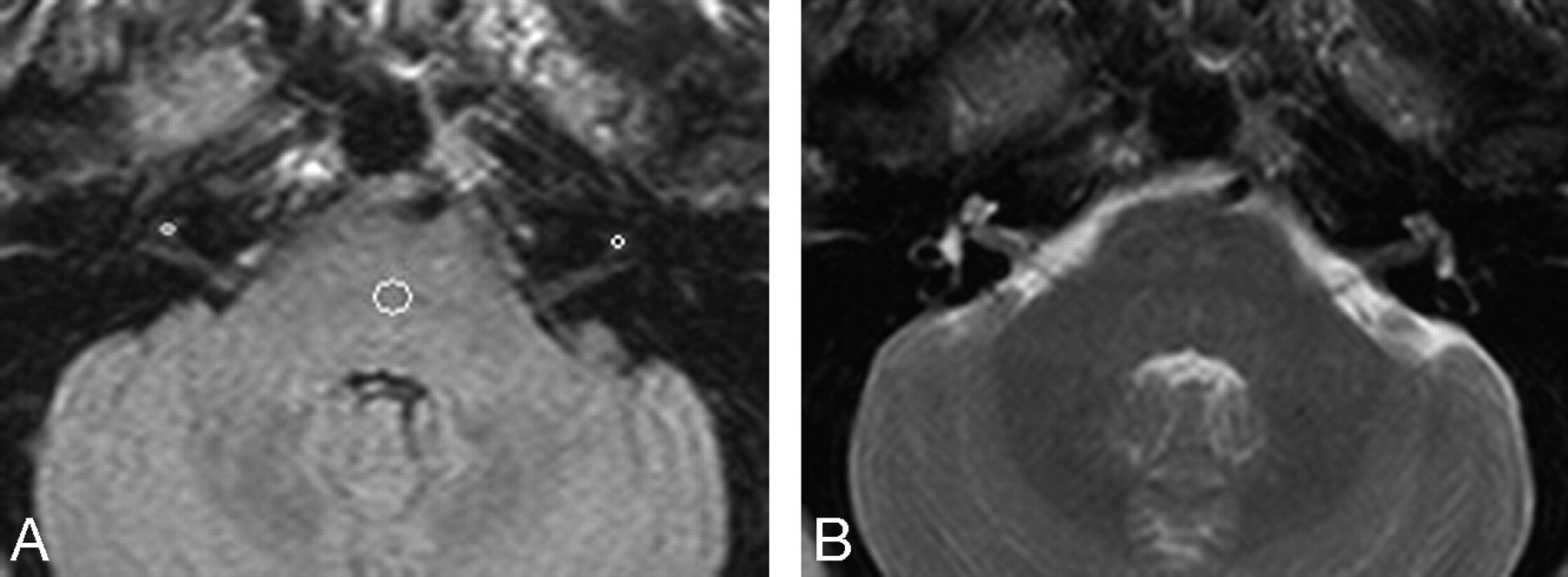
Image analysis was performed on a Centricity PACS workstation (GE Healthcare, Milwaukee, Wis). The location of vestibular schwannoma was noted in relation to the IAC. Accordingly, tumors were classified into canalicular (when entirely within the IAC), extracanalicular (when almost completely outside the IAC), and mixed canalicular and extracanalicular (when both within and outside the IAC). The maximal linear dimension of the tumor was also measured on postgadolinium focused 3-mm images through the IAC. In both patients and controls, 2 regions of interest were placed on FLAIR images. First, a small 2- to 3-mm2 region of interest was placed in the region of the basal/middle turn of the cochlea. Second, a larger 6- to 8-mm2 region of interest was placed in the brain stem on the same image. The placement of the cochlear region of interest was confirmed on T2-weighted images, which showed the cochlea with greater detail due to high fluid signal intensity (Fig 1). In patients, regions of interest were placed on the side of tumor (affected side) as well as on the opposite side (unaffected side). In control subjects, an attempt was made to place regions of interest in both cochleae, but in 5 subjects, the evaluation was unilateral because the opposite cochlea was not well seen on FLAIR images due to partial volume averaging of the surrounding structures. In addition, FLAIR images were used to determine if other structures of the membranous labyrinth such as the semicircular canals or vestibule were visualized. T1- and T2-weighted images were analyzed to exclude high T1 or low T2 signal intensities, which may suggest cochlear hemorrhage or fibrosis. All evaluations were performed by 2 Certificate of Added Qualification–certified neuroradiologists (with clinical experience of 12 and 9 years), who determined region-of-interest placements by consensus.

FLAIR (A) and T2-weighted (B) images in a patient with a intracanalicular vestibular schwannoma showing region-of-interest placements in the cochlea and brain stem on the affected and unaffected sides.
Statistical Analysis
A ratio of cochlear signal intensity to brain stem signal intensity (CIBI ratio) was determined for each cochlea. CIBI ratios from 15 affected cochleae, 15 unaffected cochleae, and 45 control cochleae were available for analysis. An unpaired t test was used to compare the ages of patients and controls. A paired t test was used to compare CIBI ratios of the affected and unaffected sides in patients. An unpaired t test was used to compare CIBI ratios of patients' affected sides and control subjects. An unpaired t test was used to compare CIBI ratios of affected sides in intracanalicular and mixed intra- and extracanalicular tumors.
Results
The average age of 15 patients (9 women, 6 men) was 56 ± 17 years with a range of 26–80 years. The average age of 25 controls (15 women, 10 men) was 51 ± 16 years, with a range of 25–78 years. The t test showed no significant difference between the ages of patients and those of control subjects.
The mean size of the vestibular schwannomas was 17 mm. Tumors ranged from 4 to 41 mm. Six of the 15 tumors were intracanalicular, 8 of 15 tumors were intra- and extracanalicular, and 1 tumor was predominantly extracanalicular.
In patients, the mean CIBI ratio for the affected side was 0.89 ± 0.18, and that for the unaffected side was 0.57 ± 0.12. For controls, it was 0.51 ± 0.07.
The cochlear signal intensity on the affected side in patients was observed to be higher compared with that on their unaffected side (Fig 2). This was confirmed by a paired t test showing significantly higher CIBI ratios on the affected side compared with the unaffected side (P < .001). There were no significant differences in CIBI ratios of the affected side in patients with intracanalicular and mixed intra- and extracanalicular tumors. In addition to the cochlea, 8 of the 15 patients also showed increased signal intensity in other portions of the membranous labyrinth, such as the semicircular canals and vestibule on the affected side. None of the patients showed signs of cochlear hemorrhage on T1- or T2-weighted images on the affected or unaffected sides.

FLAIR images of cochleae on the affected side of a patient with vestibular schwannoma (A), a control subject (B), and the unaffected side of same patient as see in A (C) clearly show increased cochlear signal intensity on the affected side compared with controls and the unaffected side.
The cochlear signal intensity on the affected side in patients was observed to be higher compared with that in controls (Fig 3). This was confirmed by an unpaired t test showing a significantly higher CIBI ratio on the affected side in patients compared with control subjects (P < .0001).

Scatterplot of CIBI ratios of affected and unaffected sides in patients and in controls.
Finally, Fig 3 shows a scatterplot of CIBI ratios on affected and unaffected sides of patients and of controls. The plot shows that most of affected sides had higher CIBI ratios than the unaffected sides and controls.
Discussion
The results presented here suggest that in patients with unilateral vestibular schwannoma, cochlear FLAIR signal intensity on the affected side is significantly higher than that on the unaffected side. The results also show that cochlear FLAIR signal intensity on the affected side in patients with vestibular schwannoma is significantly higher than that in control subjects. None of our patients had evidence of hemorrhage on T1- and T2-weighted images. Therefore, the increased cochlear FLAIR signal intensity in patients with vestibular schwannoma is most likely due to increased protein content of the cochlear perilymph, as reported previously.
In 1966, Silverstein and Schuknecht6 reported that in patients with vestibular schwannoma, total perilymph protein was approximately 9 times more than that in normal perilymph.6 On the basis of perilymph protein analysis from a large number of patients with vestibular schwannoma, Silverstein proposed the labyrinthine tap as a diagnostic test for vestibular schwannoma.7 The labyrinthine tap was performed by obtaining a sample of inner ear fluids through a hole in the stapes footplate by using a micropipet. Rapid determination of fluid protein concentration was then performed by using a yellow tetrabromophenol-indicator paper. Silverstein proposed that the risk for further deterioration of hearing loss was small and that the test was safe to use in cases where Pantopaque cisternography was equivocal for the diagnosis of unilateral sensorineural hearing loss. However, others warned against using the labyrinthine tap as a routine diagnostic test, given a small but significant reported incidence of hearing loss with the procedure.4
The pathogenesis of increased inner ear perilymph protein has been a matter of considerable investigation in the past.4,6–9 However, to date, no one agrees on a satisfactory explanation for this phenomenon. Furthermore, it has also remained unclear if protein levels in perilymph correlate with the degree of hearing loss and abnormal eighth nerve action potentials in patients with vestibular schwannoma.
Various explanations for increased cochlear perilymph protein in vestibular schwannoma have been proposed. The most plausible explanations suggested are the following: 1) blockage of neuroaxonal transport of proteins by tumor-related compression of the cochlear nerve, 2) cochlear membrane damage by arterial stasis resulting in increased permeability, and 3) cell-mediated immune reaction in the inner ear to antigenic properties of vestibular schwannomas.4,6–10 Although higher perilymph protein levels have been reported with larger vestibular schwannomas, this effect has not been related to cochlear aqueduct obstruction.4 Moreover, cerebellopontine angle meningiomas, which can easily obstruct the cochlear aqueduct by virtue of their location, usually have less elevation of perilymph protein than vestibular schwannomas.2 Therefore, most investigators have concluded that cochlear aqueduct obstruction is not a likely cause of increase in perilymph protein in patients with vestibular schwannoma.
Although a large number of investigations were focused on the pathogenesis of perilymph protein, only a few studies have looked at the relationship between hearing loss and perilymph protein level.2,7,8 These studies have not found a relationship between perilymph protein levels and the degree of hearing loss or abnormalities of eighth nerve action potentials. Given the likelihood of contamination of perilymph with blood and other fluids during the surgical procedure and the small quantities of the fluid obtained during the procedure, these relationships have not been thoroughly investigated. If the high perilymph protein levels in patients with vestibular schwannoma are due to impairment of axoplasmic protein transport from the cochlea to the brain stem nuclei as suggested by Thomsen et al,4 then there is a good possibility that the degree of cochlear nerve compression and the level of perilymph protein are related. We believe that noninvasive assessment of perilymph protein by MR imaging in various parts of the cochlea and membranous labyrinth may help in further investigating the relationship between protein levels and abnormalities on hearing tests.
FLAIR imaging is well known to be sensitive to high protein contents of the fluids.5,11 Melhem et al5 used volunteers and phantoms to demonstrate the effect of varying protein concentration of saline solutions on FLAIR signal intensity. They also altered the TE during FLAIR imaging to determine the protein concentration threshold above which the solution became hyperintense. Their findings have 2 implications regarding our study. First, the higher cochlear FLAIR signal intensity on the affected side demonstrated by us is most likely due to elevated protein levels of perilymph. Second, although we could not alter the FLAIR sequence in this retrospective study, a prospective study using different TEs may help noninvasive determination of actual protein levels. We believe that MR imaging determination of perilymph protein levels can be better correlated with hearing tests because MR imaging may allow determination of protein levels in different parts of the membranous labyrinth, such as the apical, middle, and basal turns of the cochlea, semicircular canals, and vestibule.
FLAIR has previously been used to diagnose pathologic conditions affecting the inner ear.12–14 However, to our knowledge, this is the first report of FLAIR signal-intensity abnormalities of the cochlea in patients with vestibular schwannoma. Our study has limitations due to its retrospective design. We used a higher scanning thickness than most of the other studies by using FLAIR for inner ear signal-intensity analysis. This may give rise to the potential problem of partial volume averaging effect in evaluation of cochlear signal intensity. In our study, this was less of a problem in patients with vestibular schwannoma because the cochlea was markedly hyperintense and regions of interest could be placed without difficulty within the cochlea. However, evaluation of the unaffected sides and control subjects was difficult due to the small size of the cochlea. We believe that by using T2 images as a guide for region-of-interest placement and by using small regions of interest, we have minimized the partial volume averaging effects in determination of cochlear FLAIR signal intensity on the unaffected side and in control subjects. An additional limitation of our retrospective study was our inability to compare CIBI ratios to hearing impairment because standardized hearing test results were not available in all the subjects. This limitation could be addressed in future prospective studies.
In conclusion, patients with vestibular schwannoma have increased cochlear FLAIR signal intensity on the affected side compared with the unaffected side and healthy subjects. The observed high FLAIR signal intensity in the cochlea is likely due to the elevated protein content of the cochlear fluid. Future prospective studies by using FLAIR with various TEs and thinner sections than those in our study can help noninvasive determination of perilymph protein levels and their diagnostic or prognostic utility in patients with vestibular schwannoma.
Footnotes
Paper previously presented at: Annual Meeting of the American Society of Neuroradiology, June 9–14, 2007; Chicago, Ill.
References
- Received August 7, 2007.
- Accepted after revision October 2, 2007.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}