
Abstract
BACKGROUND AND PURPOSE: Endovascular treatment of vascular lesions has revolutionized the treatment of arterial pseudoaneurysms. We describe our experience in treating carotid or vertebral pseudoaneurysms with covered stents.
MATERIALS AND METHODS: Ten patients with carotid or vertebral pseudoaneurysms treated with self-expanding or balloon-expandable covered stents were retrospectively reviewed after we obtained institutional review board approval. Distal protection devices were not used. All patients except 1 received anticoagulation therapy. Antiplatelet therapy was used in 8 of 10 patients. Follow-up was performed from 5 days to 25 months. Patients were followed with digital subtraction angiography, CT angiography (CTA), and/or sonography (US).
RESULTS: Pseudoaneurysm occlusion was obtained in all 10 patients. None of the pseudoaneurysms recanalized during the follow-up period. One patient had a distal embolization to the middle cerebral artery despite anticoagulation and antiplatelet therapy. One patient who did not receive any anticoagulation had stent occlusion at 4.5 months. Anticoagulation was stopped after 6 months in 2 patients with persistent stent patency and no neurologic complications for >1 year. Both US and CTA were useful for extracranial stent surveillance. CTA was helpful for intracranial stent surveillance.
CONCLUSION: In this small series, the use of covered stents allowed safe and effective treatment of pseudoaneurysms occurring in the cervical and cephalic segments of the carotid and vertebral arteries.
Carotid and vertebral pseudoaneurysms are uncommon vascular lesions that may occur following trauma, tumor invasion/radiation necrosis, or mycotic infection. Left untreated, they are associated with adverse outcomes, including hemorrhage, enlargement, vessel occlusion, and distal thromboembolism.1 Historically, most of these pseudoaneurysms have been treated surgically if the lesion was accessible. Nonaccessible lesions were treated with anticoagulation and antiplatelet therapy, which rarely brings about resolution.2,3 However, with advances in technology, endovascular therapy is becoming a common first-line treatment, with multiple reports showing placement of covered stents to be both effective and safe.1,4–6 We describe our experience with the placement of covered stents for the treatment of carotid and vertebral pseudoaneurysms secondary to trauma, tumor invasion/radiation necrosis, or mycotic infection in 10 patients.
Materials and Methods
After receiving institutional review board approval, we retrospectively reviewed the records between October 2004 and December 2006 of 10 patients (8 males and 2 females), ages 15–81 years (mean age, 38.3 years) who were treated for pseudoaneurysm of a carotid or vertebral artery with self-expanding or balloon-expandable covered stents. The on-line Table provides the individual information regarding presentation, location of the pseudoaneurysm, type of stent, complications, anticoagulation regimen, and duration of follow-up. The etiologies were blunt trauma (n = 5), penetrating trauma (n = 2), tumor invasion/radiation necrosis (n = 2), and mycotic infection (n = 1). Seven of the procedures were emergent and 3 were elective. The arteries involved were the common carotid artery (CCA) or cervical internal carotid artery (ICA) (n = 7), the cavernous carotid artery (n = 2), and the vertebral artery (n = 1). The stents were placed by using a transfemoral percutaneous technique in all 10 patients. We used the following 10 covered stents: 6 Fluency stents (Bard Peripheral Vascular, Tempe, Ariz), 2 Jostent GraftMaster stents (Abbott Laboratories, Abbott Park, Ill), 1 GORE VIABAHN (W.L. Gore & Assoc, Newark, Del), and 1 iCast (Atrium Medical, Hudson, NH). Institutional review board authorization was obtained prospectively for the 2 cavernous carotid stents. Two uncovered stents were used to supplement covered-stent placement: 1 Driver (Medtronic, Minneapolis, Minn) and 1 S.M.A.R.T. Control (Cordis, Miami Lakes, Fla). The stents ranged in diameter from 3.5 to 9 mm. Eight stents were self-expanding, and 4 were balloon-expandable. Distal protection devices were not used in any of the cases.
Three of the 10 patients (on-line Table, patients 4, 5, and 9) were given a loading dose of 300-mg clopidogrel before the procedure and then were placed on 75 mg daily. Patient No. 6 was pretreated with 325 mg aspirin (ASA) and 75 mg clopidogrel for 3 days before the procedure, and patient No. 8 was pretreated with 81 mg ASA and 75 mg clopidogrel for 5 days before the procedure. Nine of the 10 patients received unfractionated heparin during the procedure to maintain an activated clotting time 2.0–2.5 times above baseline, and 8 patients received antiplatelet therapy with ASA and clopidogrel. To avoid bleeding complications from other extensive traumatic injuries, we excluded patient No. 2 from heparinization and antiplatelet therapy and patient No. 3 was excluded from postprocedural antiplatelet therapy. Patient No. 10 was placed on ASA and clopidogrel postprocedure, which was continued for 9 days; then the patient was returned to heparin alone for 10 days (target partial thromboplastin time, 40–60 seconds) in preparation for a tracheostomy and ventriculoperitoneal shunt placement. After the procedures, the heparin was discontinued, and the patient was restarted on ASA and clopidogrel. The patients were followed with sonography (US) or CT angiography (CTA) along with clinical examination.
Results
The covered stents were deployed successfully with the exclusion of the pseudoaneurysms in all 10 patients (on-line Table). Six cases were straightforward and uneventful. Four cases were not and are described in greater detail.
Patient No. 2 had a laceration and pseudoaneurysm of the right vertebral artery origin following a motor vehicle crash. Due to multiple traumatic injuries, the patient was not placed on anticoagulation or antiplatelet therapy. Catheterization of the right vertebral artery was not possible. A 7 × 4 mm Fluency stent was placed in the right subclavian artery across the vertebral artery origin. Immediate right subclavian and left vertebral arteriography showed patency of the right subclavian artery stent and no antegrade or retrograde opacification of the pseudoaneurysm.
Patient No. 3 was found to have a right ICA laceration and a pseudoaneurysm at the level of C1 after being hit by a truck while riding a bicycle. A VIABAHN 7 × 50 mm stent was deployed across the laceration with successful occlusion of the pseudoaneurysm. However, severe stenosis in the proximal petrous portion of the right ICA persisted, most likely from a dissection. An unsuccessful attempt was made to dilate this stenosis with a 5 × 40 mm balloon angioplasty. An uncovered Driver 4 × 15 mm stent was then placed in the petrous portion of the right ICA and was inflated to a diameter of 4.3 mm. However, the segment between the Driver stent and the VIABAHN stent remained stenotic. A S.M.A.R.T. 7 × 40 mm stent was then deployed between the Driver and VIABAHN stents, partially overlapping both. Completion angiography demonstrated wide patency of the artery.
Patient No. 5, with a history of metastatic thyroid cancer, radiation therapy, and multiple surgical resections, presented with bleeding from his tracheostomy site. The patient was found to have a left CCA pseudoaneurysm, which was occluded with a Fluency 8 × 40 mm stent (Fig 1). Despite procedural heparin and loading with 300-mg clopidogrel, the immediate poststenting cerebral angiogram showed occlusion of the left middle cerebral artery M1 segment. Fifteen milligrams of intra-arterial recombinant tissue plasminogen activator (tPA) was administered into the occluded segment; however, the clot did not resolve acutely. Eleven days after the procedure, a noncontrast CT showed only small infarcts on the left in the globus pallidus and peripheral parietal/occipital lobes, suggesting partial restoration of the middle cerebral artery perfusion. At discharge, the patient exhibited 3/5 strength of the right upper extremity and mild imbalance on physical examination.

An 81-year-old man (patient No. 5) with metastatic thyroid cancer, treated with radiation therapy, presented with bleeding from his tracheostomy. A, A left CCA angiogram demonstrates a large pseudoaneurysm at the tracheostomy. B, Following placement of a covered stent (Fluency, 8 × 40 mm), there is exclusion of the pseudoaneurysm. C, An aortic arch angiogram demonstrates no evidence of atherosclerotic disease.
Patient No. 8 had a bilobed mycotic pseudoaneurysm in his right cavernous carotid artery, discovered because of ophthalmoplegia 11 days after sinus surgery. The original plan was to treat the pseudoaneurysm with a covered stent after a 12-week course of intravenous antibiotics; however, the pseudoaneurysm was increasing in size on sequential imaging studies. After 22 days of antibiotics, with the patient having negative blood cultures and being afebrile for 21 days, we believed that the benefits of stent placement outweighed the risks of an infected covered stent. A GraftMaster 4 × 16 mm stent was placed successfully without complication. The patient was discharged and completed his 12-week course of intravenous antibiotics.
Follow-Up
Eight patients underwent follow-up imaging ranging from 5 days to 25 months with no evidence of pseudoaneurysm recanalization or enlargement. Two of the 10 patients died from causes unrelated to their carotid lesions before follow-up imaging could be performed.
Patient No. 1 had a left ICA pseudoaneurysm at the level of C2 after penetrating knife injury. The pseudoaneurysm was occluded by a Fluency stent. Follow-up US at 15 days showed continued occlusion of the pseudoaneurysm with a patent left ICA.
Patient No. 2, with multiple traumatic injuries sustained during a motorcycle-versus-automobile crash, had a laceration of the right vertebral artery origin with a pseudoaneurysm. The patient was not placed on anticoagulation or antiplatelet therapy, and the Fluency stent placed in his right subclavian artery (Fig 2) was found to be occluded on follow-up US at 4.5 months. However, the US revealed collateral reconstitution of the distal right subclavian and distal right vertebral arteries, as well as continued occlusion of the pseudoaneurysm. Patient No. 3 was not followed up, because he died 4 days postprocedure due to multiple trauma. Patient No. 4 was found to have a pseudoaneurysm at the proximal anastomosis of an interposed vein graft at the left CCA/ICA junction, which had been placed for a prior bullet injury. With US, the patient was found to have a patent left CCA/ICA Fluency stent with occlusion of the pseudoaneurysm at 25 months. The patient is currently neurologically intact on clinical examination and has been off all anticoagulation medications for >1 year.
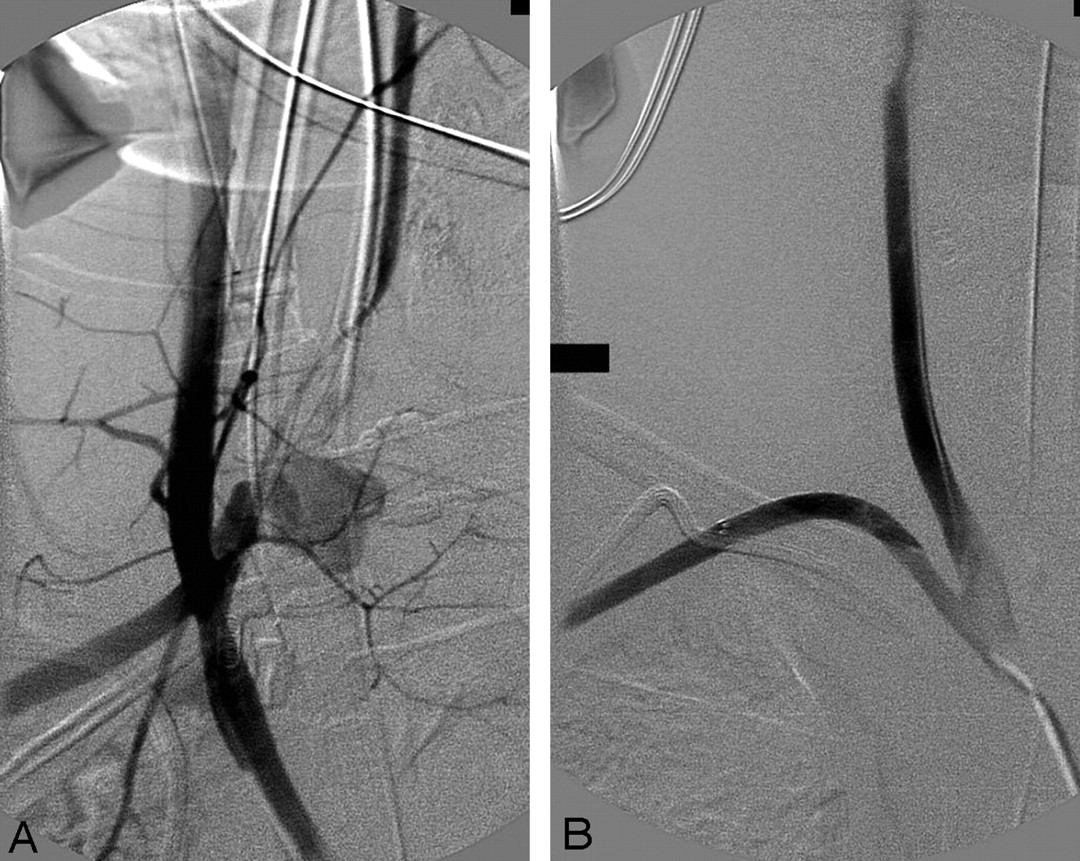
A 15-year-old adolescent boy (patient No. 2) after a motor vehicle crash. A, A right subclavian artery angiogram demonstrates a large pseudoaneurysm and laceration at the origin of the right vertebral artery. B, Following placement of a covered stent (Fluency, 7 × 40 mm), there is exclusion of the pseudoaneurysm.
Patient No. 5, who had an M1 occlusion, was not followed up because he died shortly after hospital discharge to a skilled nursing facility.
Patient No. 6 presented with transient paresthesias and was found to have a pseudoaneurysm in her distal cervical ICA, approximately 3 months after an automobile crash. An iCast stent was used to occlude the pseudoaneurysm and was found patent, with persistent occlusion of the pseudoaneurysm, by using both CTA at 18 days and US at 20 months poststent placement. The patient is currently neurologically intact on clinical examination and has been off all anticoagulation medications for >1 year.
Patient No. 7, with a history of hypopharyngeal carcinoma, radiation therapy, and multiple surgical resections, presented with hemoptysis and bleeding from his tracheostomy site. The patient was found to have a left CCA pseudoaneurysm, which was occluded with a Fluency stent. The patient had a nondiagnostic US (due to large body habitus) performed 3 days after stent placement. Five days after placement a CTA showed a patent stent and occlusion of the pseudoaneurysm. The patient died 15 days postprocedure due to carcinomatosis and bacteremia. With CTA, Patient No. 8 was found to have a patent right cavernous carotid artery GraftMaster stent with occlusion of the pseudoaneurysm at 7 months. The patient is currently neurologically intact on clinical examination.
Patient No. 9 was found to have a lacerated proximal left CCA with a pseudoaneurysm from a bullet injury, which was successfully occluded with a Fluency stent. CTA at 13 days postprocedure showed occlusion of the pseudoaneurysm and stent patency. Patient No. 10 was found to have a right carotid cavernous fistula with a large venous pseudoaneurysm secondary to a skull base fracture acquired during an automobile crash. A GraftMaster stent successfully occluded the pseudoaneurysm. The stent was found to be patent with occlusion of the pseudoaneurysm by using CTA 22 days postprocedure.
Discussion
Carotid and vertebral pseudoaneurysms are uncommon lesions that may occur as sequelae of blunt trauma, cancer/radiation necrosis, or mycotic infection. Historically, treatment of pseudoaneurysms has been primarily surgical.1 However, surgery of pseudoaneurysms located near the skull base is technically challenging and has been associated with high morbidity/mortality rates.6,7 More recently, endovascular techniques have become more appealing as multiple studies have provided encouraging results.1,4–6 Coldwell et al8 describe 14 patients with traumatic ICA pseudoaneurysms treated with self-expanding bare metal stents. Two of these patients had persistent pseudoaneurysms at 2-month follow-up, which eventually resolved after an additional 2 months. The pseudoaneurysms remained occluded in all 14 patients, with 13 stents remaining widely patent (follow-up, 6–21 months) and 1 showing mild narrowing at 3 months. Marks et al9 reported continued opacification of an ICA pseudoaneurysm 8 months after bare stent deployment; this was believed to have resulted from the porous stent structure.
Bush et al10 reported the treatment of ICA pseudoaneurysms due to blunt carotid injury by placing bare stents and adding coil embolization of the excluded pseudoaneurysm in 5 patients; occlusion of all 5 pseudoaneurysms resulted. At follow-up (mean, 11.7 months) all 5 pseudoaneurysms remained occluded, with 4 of 5 stents remaining widely patent; 1 of the 4 had developed a 60% focal stenosis. However, even with secondary coiling through a bare stent, Layton et al5 showed that an ICA pseudoaneurysm can continue to opacify and enlarge. Patel et al11 believe there is always potential for pseudoaneurysm recanalization when using bare stents, even with secondary coiling of the pseudoaneurysm.
There are 2 primary types of stent-deployment systems: balloon-expandable and self-expanding. Self-expanding stents are preferred in the carotid artery because of the potential for permanent collapse of the stent from extrinsic pressure.12 In our series, we used 3 balloon-expandable stents for primary treatment: 2 were used because the lesion was intracranial and 1 because it was the only correctly sized stent available in our inventory. In 1 patient (No. 3), a balloon-expandable uncovered stent was placed for residual stenosis in the cervical ICA at the cranial end of a self-expanding stent. Follow-up imaging on this extracranial balloon-expandable stent was not available because the patient died 4 days after the procedure.
Intraprocedural complications from carotid stent placement are attributable to thromboembolism. McCready et al13 describe 2 of 4 patients who developed transient ischemic attacks secondary to thromboembolism in middle cerebral artery branches following covered-stent placement for an ICA pseudoaneurysm. Distal protection was not used in their cases, for patients were believed to be at low risk because there was no obvious thrombus within the pseudoaneurysms on arteriography. May et al14 reported 1 patient who had an embolic stroke during covered-stent placement for an ICA pseudoaneurysm. At 6 months follow-up, the aneurysm and the stent were occluded. The previously mentioned article about a series of 14 patients treated with bare stents for ICA pseudoaneurysms describes the use of only procedural heparin without distal protection or antiplatelet therapy, and none of the patients developed stroke symptoms.8
We had 1 patient (No. 5) develop a thromboembolic occlusion of the left M1 segment despite a loading dose of clopidogrel and procedural heparin. The patient had no significant atherosclerotic disease or evidence of thrombus in his pseudoaneurysm on diagnostic imaging. It is possible that occult thrombus within the pseudoaneurysm was dislodged when a guidewire inadvertently entered the pseudoaneurysm. Alternatively, distal embolization may have been related to his hypercoagulable state (thyroid cancer); this possibility raises the question as to whether distal protection should be used in all patients with hypercoagulable diseases. Because a platelet aggregate is unlikely to embolize without associated fibrin, we believed that infusing tPA into the embolus was indicated. It is possible, however, that the addition of an antiplatelet receptor IIb/IIIa inhibitor may have been useful.
Consensus does not exist as to the ideal anticoagulation/antiplatelet regimen with stent placement for carotid artery pseudoaneurysms. Bare metal ICA stents were found to be patent in 14 of 14 patients on warfarin (Coumadin) after a mean follow-up of 6 months.8 In another study, a covered stent placed for delayed pseudoaneurysm after carotid endarterectomy (CEA) was found occluded at 6-month follow-up, despite the patient being on Coumadin.14 Duane et al15 describe the 2-year patency of a covered stent placed in the right ICA for traumatic pseudoaneurysm on daily ASA alone, whereas a covered stent in another patient of theirs was occluded at 6 weeks on ASA therapy. Kubaska et al16 describe a 2-year patency of a covered stent placed in the left ICA for traumatic pseudoaneurysm after being treated with ASA and clopidogrel for just 30 days. One case report describes a Wallgraft (Boston Scientific, Natick, Mass) covered stent placed in the carotid bulb for delayed pseudoaneurysm following CEA to be occluded at 12 months despite 6 weeks of clopidogrel followed by continued ASA.13
We used varying anticoagulation/antiplatelet regimens due to the supposed risk of hemorrhage from the pseudoaneurysm or the other severe injuries. Clopidogrel was given either before or as a loading dose during the procedure in 5 of our 10 patients. Eight patients received clopidogrel and ASA postprocedure. Procedural heparin was used in 9 of our patients. Because there is individual variation in platelet aggregation and clot formation, the ideal antiplatelet regimen will probably remain unknown.
We found no specific articles reporting the ideal follow-up imaging for covered stents in carotid or vertebral arteries. While digital subtraction angiography is known as the gold standard for evaluation of arterial stenosis, Orbach et al17 have shown that by using stent-optimized reconstruction kernels, CTA can approximate the accuracy of digital subtraction angiography for the evaluation of bare metal stents. Although in our experience CT and US were both useful, we believe that US is the examination of choice if the stent is not obscured by the skull base or thoracic inlet. US is inexpensive, easy to use, and does not require radiation. We found that routine CTA was helpful to determine patency in stents as small as 4 mm in diameter in the cavernous segment of the carotid artery.
Conclusion
Our experience suggests that covered stents are an effective treatment option for carotid and vertebral artery pseudoaneurysms.
Footnotes
Indicates article with supplemental on-line table.
References
- Received May 4, 2007.
- Accepted after revision November 30, 2007.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}