
Abstract
BACKGROUND AND PURPOSE: Clot extent, location, and collateral integrity are important determinants of outcome in acute stroke. We hypothesized that a novel clot burden score (CBS) and collateral score (CS) are important determinants of clinical and radiologic outcomes and serve as useful additional stroke outcome predictors.
MATERIALS AND METHODS: One hundred twenty-one patients with anterior circulation infarct presenting within 3 hours of stroke onset were reviewed. The Spearman correlation was performed to assess the correlation between CBS and CS and clinical and radiologic outcome measures. Patients were dichotomized by using a 90-day modified Rankin scale (mRS) score. Uni- and multivariate logistic regression models were used to assess variables predicting favorable clinical and radiologic outcomes. Receiver operating characteristic and intraclass correlation coefficient (ICC) analyses were performed. Diagnostic performance of a CBS threshold of >6 was assessed.
RESULTS: There were 85 patients (mean age, 70 ± 14.5 years). Patients with higher CBS and CS demonstrated smaller pretreatment perfusion defects and final infarct volume and better clinical outcome (all, P < .01). CBS (P = .009) and recanalization (P = .015) independently predicted favorable outcome. A CBS >6 predicted good clinical outcome with an area under the curve of 0.75 (95% confidence interval [CI], 0.65–0.84; P = .0001), sensitivity of 73.0 (95% CI, 55.9–86.2), and specificity of 64.6 (95% CI, 49.5–77.8). The recanalization rate with intravenous recombinant tissue plasminogen activator was higher in patients with CBS >6 (P = .04; odds ratio, 3.2; 95% CI, 1.1–9.4). The ICC was 0.97 (95% CI, 0.95–0.98) and 0.87 (95% CI, 0.80–0.91) for CBS and CS, respectively.
CONCLUSIONS: CBS and CS are useful additional markers predicting clinical and radiologic outcomes.
Persistent anterior cerebral circulation occlusion is one of the most devastating clinical events, often causing severe neurologic deficit or death. Current stroke strategy focuses on recanalization as one of the most important factors to reduce tissue at risk and reverse neurologic deficits. The extent of revascularization depends not only on recanalization of the primary arterial occlusive lesion but also on reperfusion of the distal vascular bed.1 Many factors impact the success of recanalization, including clot composition, thrombolytic technique, extent of clot burden, site of clot impaction, and collateral supply.2-6 More proximal and increased clot length is harder to treat, leading to a worse outcome compared with a shorter distal clot.2,3,5,7,8 Patients with a hyperattenuated middle cerebral artery (MCA) sign, essentially a marker of proximally located thrombus, have been shown to have a larger final infarct volume and worse functional outcome.2 Tandem internal carotid artery (ICA)/MCA occlusions have lower early recanalization and early neurologic improvement rates compared with isolated MCA occlusion.9
Although the effects of clot burden have been indirectly examined via the hyperattenuated arterial sign on noncontrast CT (NCCT)3,10,11 and directly via conventional angiographic studies, these have only recently been assessed and quantified with CT Angiography (CTA).2 Many clinical and radiologic variables impact the decision for thrombolysis and route of administration. Treatment decisions need to be made rapidly due to the narrow therapeutic window. CTA is widely available and provides a rapid assessment of many of the variables needed to make these decisions. CTA improves infarct depiction and delineation12,13 and provides a noninvasive assessment of cervical and intracranial circulation. CT perfusion (CTP) may also provide important additional information in the acute stroke setting that may be used to predict outcome.14-17
The degree of collateral supply through peripheral leptomeningeal sources is important and correlates with the presence of smaller final infarct volume.4,18 Evaluation of collateral supply remains challenging due to their diminutive size and complex routes.19 A conventional angiographic grading system demonstrated a significant relationship between collateralization and favorable outcome.20,21 Collateral presence was the only radiologic predictor of favorable outcome in this study, despite a simplistic binary categorization.21 A modified collateral score by using high-resolution multidetector CTA, which grades degree of leptomeningeal collateral supply in the MCA territory from grade zero (no collateral supply) to 3 (complete collateral supply), has recently been proposed.22 We refer to this grading system as a collateral score (CS) in this study.
In many centers, CTA precedes conventional angiography for the assessment of patients with stroke. The rationale in these centers is to gather information pertaining to vascular anatomy and site of occlusion before thrombolytic treatment. The purpose of this study was to compare the relationship of clot extent and collaterals with clinical outcome and amount of tissue at risk. We hypothesized that a novel clot burden score (CBS) and the CS are important determinants of clinical and radiologic outcomes and serve as useful additional variables in stroke outcome prediction.
Materials and Methods
Study Design and Patient Cohort
A single-center retrospective study was performed in all patients presenting within 3 hours of stroke symptoms to a regional stroke center between October 2005 and December 2007. Patients were assessed by the stroke team and underwent clinical assessment and an acute CT-based stroke protocol, including CTA and CTP. Follow-up imaging included repeat CTA/CTP within 24 hours and 5- to 7- day CT or MR imaging. Clinical data were collected by a stroke neurologist (J.H. and D.G., 3 and 5 years’ experience, respectively) and maintained in a prospective stroke database (M.M., K.W.). Presenting National Institutes of Health Stroke Scale (pre-NIHSS) and 3-month follow-up modified Rankin Scale (mRS) scores were the minimum clinical data required for the study. For the purpose of this study, only patients with unilateral MCA territory stroke who had completed 90-day clinical follow-up were included. Of 458 patients in a prospective stroke and transient ischemic attack data base, 121 had unilateral anterior circulation infarct with variable occlusion involving the MCA with or without ICA occlusion—none had anterior cerebral artery (ACA) infarcts. Of those, 36 patients did not have complete 90-day clinical follow-up at the time of data analysis and were excluded from the study. The final cohort comprised 85 patients. This study was approved by the institutional review board, and individual patient consent was obtained.
Scanning Protocol and Generation of Parametric Maps
The CT stroke protocol, performed on a 64-section CT scanner (LightSpeed VCT, GE Healthcare, Milwaukee, Wis), included pre- and postcontrast CT head scans with the following parameters: 120 kilovolt (peak) (kVp), 340 mA, 8 × 5 mm collimation, 1 s/rotation, and table speed of 15 mm/rotation. CTA was performed from the aortic arch to the vertex with the following parameters: 0.7 mL/kg iodinated contrast agent up to a maximum of 90 mL (iohexol, Omnipaque, 300 mg iodine/mL; GE Healthcare, Piscataway, NJ), 5- to 10-second delay, 120 kVp, 270 mA, 1 s/rotation, 1.25-mm-thick sections, and table speed of 3.7 mm/rotation. CTA data were automatically processed by the technicians, including multiplanar 7-mm maximum intensity projection (MIP) reconstructions and 4-mm axial reformats or CTA source images.
The CTP technique included a 45-second scanning reconstructed at 0.5-second intervals to produce a series of 90 sequential images for each of the 8 sections, covering a total of 40 mm from the basal ganglia to the lateral ventricles. CTP scanning parameters were the following: 80 kVp, 190 mA, 0.5-mL/kg (maximum, 50 mL) iodinated contrast agent injected at 4 mL/s with a 3- to 5-second delay.
A repeat CTA or MRA was performed within 24 hours of the initial study. Follow-up included an NCCT head scan with similar parameters as previously mentioned and/or follow-up MR imaging protocol at days 5–7. MR imaging sequences included axial fluid-attenuated inversion recovery (FLAIR) (TR/TE/TI, 8000/120/200 ms; FOV, 22 cm; matrix, 320 × 224; section thickness [ST], 5; 1-mm gap), gradient T2-weighted (TR/TE, 1100/35 ms; flip angle [FA], 20°; FOV, 24 cm; matrix, 320 × 224; ST, 5; 1-mm gap), diffusion-weighted imagining (TR/TE, 8125 ms/min; FOV, 26 cm; image matrix, 128 × 128 pixels; ST, 5 mm with no gap), T2-weighted fast spin-echo (TR/TE, 5100/100 ms; ST, 5 mm; 1-mm gap; FOV, 24 cm; matrix, 320 × 224), and sagittal T1-weighted FLAIR (TR/TE/TI, 2163/26/750 ms; FOV, 22 cm; matrix, 320 × 224; ST, 5; 1-mm gap). 3D spoiled gradient-recalled-echo contrast-enhanced MRA parameters were the following: TE/FA, minimum/35°; ST, 2 mm; FOV, 30 cm; matrix, 384 × 320. Gadolinium 9 mL (Gadovist; Bayer Schering Pharma, Berlin, Germany) 1.5 mL/s with 25 mL of saline flush at same rate.
Imaging Analysis
Scores.
The Alberta Stroke Program Early CT Score (ASPECTS) methodology is well described by Barber et al23 and is shown to have high interobserver agreement. Precontrast CT head scans were independently reviewed by 2 staff neuroradiologists (R.I.A., S.P.S. with 5 years’ stroke imaging experience) who were blinded to the patient's clinical symptoms. Median ASPECTSs of these readers were used.
The CBS is a scoring system to define the extent of thrombus found in the proximal anterior circulation by location24 and is scored on a scale of 0–10 (Fig 1). A score of 2 is subtracted if thrombus is found in each of the supraclinoid ICAs, the proximal half of the MCA trunk, and the distal half of MCA trunk. A score of 1 is subtracted if thrombus is found in the infraclinoid ICA, ACA, and for each affected M2 branch. The thrombus can be partially or completely occlusive. A score of 10 is normal, implying clot absence. A score of 0 implies complete multisegment vessel occlusion.

Illustration of CBS. A, A 10-point score is normal, implying absence of thrombus. Two points (as indicated) are subtracted for thrombus found on CTA in the supraclinoid ICA and each of the proximal and distal halves of the MCA trunk. One point is subtracted for thrombus found in the infraclinoid ICA and A1 segment and for each affected M2 branch. B, Occlusion of infra- and supraclinoid ICAs with a CBS of 7. C, Distal M1 and 2 M2 branch occlusions produce a CBS of 6. D, Occlusion of the terminal ICA, proximal M1, and A1, with a resultant CBS of 5.
The collateral grading system was scored on a scale of 0–3 (Fig 2).19,21 A score of zero indicated absent collateral supply to the occluded MCA territory. A score of 1 indicated collateral supply filling ≤50% but >0% of the occluded MCA territory. A score of 2 was given for collateral supply filling >50% but <100% of the occluded MCA territory. A score of 3 was given for 100% collateral supply of the occluded MCA territory. Both the CBS and CS were scored independently and read by a staff neuroradiologist (S.P.S. with 5 years’ experience) and neuroimaging fellow (I.Y.L.T. with 1 year of experience) blinded to clinical data. Raw data and reconstructed CTA images were available for review. Median CS and CBS scores of these readers were used. ASPECTS, CBS, and CS were all obtained only on baseline imaging.

MTT and CTA source images (CTA-SI) of 4 different cases, each demonstrating prolonged MTT from a left MCA territory ischemia. CS grading is demonstrated for each collateral grade. A, Absence of vessels on CTA-SI is consistent with a CS of 0. B, A score of 1 indicates collateral supply filling ≤50% but >0% of the occluded MCA territory. C, A score of 2 is given for collateral supply filling >50% but <100% of the occluded MCA territory. D, A score of 3 is given for 100% collateral supply of the occluded MCA territory.
Recanalization was graded according to the Thrombolysis in Myocardial Infarction (TIMI) classification on follow-up CTA/ MRA, which was performed within 24 hours of initial study. TIMI zero and 1 were considered nonrecanalized.
Image Processing.
CT Perfusion 4 software (GE Healthcare) was used to calculate parametric maps of CBF, CBV, and mean transit time (MTT) by using data from the baseline CT perfusion study. Maps were calculated by deconvolution of the arterial input curve by using the model of Johnson and Wilson.25 Partial volume averaging of the arterial input curve was corrected by using the venous time-attenuation curves.26 Arterial input and venous output functions were obtained from the ipsilateral ACA and from the superior sagittal sinus, respectively. Functional maps created with CTP were analyzed by using custom software (IDL, Verison 6.1; RSI, Chapel Hill, NC) (R.I.A., 5 years’ experience). All components of the analysis were performed blinded to clinical information to reduce bias. Thresholds of cerebral blood volume (CBV) <1.0 mL/100 g and a cerebral blood flow (CBF) threshold of <25 mL/100 g/minute were used for volumetric measurement of penumbra and infarct, respectively.17,27 The final infarct volume was measured on the follow-up CT or MR imaging study by using Medical Image Processing, Analysis and Visualization, Version 4.0.2-2007-12-12 (Center for Information Technology, National Institutes of Health Bethesda, Md).
Statistical Analysis
Calculations were performed by using SAS (Version 9.1; SAS Institute, Cary, NC) statistical software package (L.Z.). Results were expressed as the mean ± SD or median (interquartile range [IQR]) for quantitative variables and as proportions for categoric findings. The Spearman nonparametric rank correlation was performed to assess the correlation between variables and clinical and radiologic outcomes according to recanalization status. Patients were dichotomized by using the 90-day mRS score into good (mRS score, ≤2) versus poor outcome (mRS score, >2).
Group comparisons were made by using the Wilcoxon rank sum test and the Fisher exact test. Log transformation was used for variables not passing the normality check. A P value of <.05 was considered statistically significant. A univariate logistic regression model was repeated; adjustment for potential confounders included age, sex, and recombinant tissue plasminogen activator (rtPA) administration. Overdispersion and underdispersion were corrected with the Pearson goodness-of-fit statistic. Odds ratio (OR) with 95% confidence interval (CI) was calculated for each variable.
Multivariate analysis was then performed. The Hosmer and Lemeshow test and C statistic were used to assess the goodness of fit of the multivariate logistic regression model. The subjects were divided into approximately 10 groups of roughly the same size on the basis of the percentiles of the estimated probabilities. The discrepancies between the observed and expected number of observations in these groups were summarized by the Pearson χ2 statistic, which was then compared with a χ2 distribution with t df, where t is the number of groups minus n. A small P value suggested that the fitted model was not adequate. The C statistic is a measure of the discriminative power of the logistic equation. It varies from 0.5 (the predictions of the model are no better than chance) to 1.0 (the model always assigns higher probabilities to correct cases than to incorrect cases for any pair involving dependent = 0 and dependent = 1). Thus C is the percentage of all possible pairs of cases in which the model assigns a higher probability to a correct case than to an incorrect case.
Radiologic outcomes measured by final infarct volume and success of recanalization were also analyzed by using the above statistical models. Due to the dynamic nature of clot and collaterals and the interaction with time from onset to scanning, scanning to rtPA, and MTT × recanalization, we considered interaction of these factors with CBS. Finally, receiver operating characteristic (ROC) curve analysis was performed on the CBS, the area under curve (AUC) was measured, and a threshold was found. Inter-rater reliability was assessed by intraclass correlation coefficient (ICC) analysis of CBS and CS. A value of 0.20 implied poor agreement; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, good agreement; and 0.81–1.0, very good agreement.
Results
Baseline Data
The mean patient age was 70 ± 14.5 years with 36/85 (42%) being male patients. Baseline median pretreatment NIHSS score was 16 (IQR, 10–20). Median symptom onset-to-CT time was 108 minutes (IQR, 70–148). Intravenous rtPA was given to 60 patients (70.5%). Median time to rtPA was 143 minutes (IQR, 120–165) with a mean dose of 60.5 ± 16.5 mg. The median baseline NCCT ASPECTS was 7 (IQR, 5–9); CBS, 6.5 (IQR, 5–9); and CS, 2 (IQR, 1.5–3). Recanalization occurred in 37 patients (43.5%). Thirty (50%) patients receiving rtPA were recanalized compared with 7 (7/25 or 28%) who were not. Final infarct size was 54 mL (IQR, 17–166 mL). Median 90-day mRS score was 3 (IQR, 2–5). Good clinical outcome was seen in 37 patients (43.5%).
CBS and CS Correlation
Correlation was better for CS than CBS for all measured perfusion parameters (Table 1). Patients with smaller thrombus extent (ie, higher CBS) and better collaterals demonstrated smaller pretreatment CBF, MTT, and CBV (P < .01 for all parameters) and final infarct volume (P < .01) and better functional clinical outcome (P < .01). CS was higher in patients with smaller thrombus extent (r = 0.38, P < .01).
Spearman rank correlation of CBS and CS
Clinical Outcome
Patients with good clinical outcomes were younger (P = .009), with higher baseline ASPECTSs (P < .0001), lower baseline NIHSS scores (P < .0001), earlier presentation (P = .027); and smaller final infarct volume (P < .0001) (Table 2). These patients also had a higher CBS (P = .0005), CS (P = .002), and recanalization rates (P = .022) and smaller perfusion defects. No rtPA or sex differences were found between the 2 groups.
Patient clinical outcome dichotomized into good (mRS score, ≤2) and poor clinical outcome (mRS score, >2) at 90 days
Univariate logistic regression analysis is presented in Table 3. Baseline NIHSS score, CBS, and ASPECTS were the most significant predictors of clinical outcome. We considered 5 variables a priori as potential important clinical confounders, including sex, age, baseline NIHSS score, ASPECTS, and rtPA administration. Univariate analysis was repeated, controlling for these variables. Baseline NIHSS score, ASPECTS, and age were significant confounders, but rtPA and sex had limited effect. After adjustment, CBS (P < .01), final infarct volume (P < .01), and time to scanning (P < .01) were significantly associated with clinical outcome. Recanalization had borderline significance (P = .047). Multivariate logistic regression analysis, adjusting for confounders, demonstrated significance for CBS (P = .009), recanalization (P = .015), and 2 confounding factors: baseline NIHSS (P = .0025) and age (P = .0181) (Table 4). There was an adequate model goodness of fit demonstrated by the Hosmer and Lemeshow test (P = .72) and C statistic (C = 0.90). Interaction with CBS and time from onset to scanning, scanning to rtPA, and MTT × recanalization were considered. No interaction could be found between each of these parameters and CBS (P = .25, P = .27, P = .08, P = .69). CBS, recanalization, baseline NIHSS score, and age remained significantly associated with outcome.
Univariate logistic regression analysis for favorable clinical outcome (mRS score, ≤2 at 90 days)
Multivariate logistic regression analysis of favorable clinical outcome (mRS score, ≤2 at 90 days), controlling for confounders
ROC analysis (Fig 3) demonstrated an AUC of 0.75 (95% CI, 0.65–0.84; P = .0001). CBS >6 predicted good clinical outcome with a sensitivity of 73% (95% CI, 55.9%–86.2%), a specificity of 64.6% (95% CI, 49.5%–77.8%), and a positive likelihood ratio of 2.1. The patient group was dichotomized by a CBS threshold of >6 (Table 5). There was no significant difference between the 2 groups for age, sex, and baseline clinical variables, including time to scanning (P = .3), time to rtPA (P = .8), rtPA dose (P = .2), hypertension (P = .47), and hyperglycemia (P = .75). Patients with CBS >6 had a higher baseline ASPECTS, smaller CBV and CBF volume, higher collateral score, smaller final infarct size, and better clinical outcome. Risk of parenchymal hemorrhage was lower but did not reach statistical significance (P = .08).

ROC for CBS prediction of good clinical outcome (mRS score, ≤2). A threshold of >6.5 was found with an AUC of 0.73 (95% CI, 0.62–0.82; P = .0001).
Group dichotomization by ROC-defined CBS threshold of more than 6
Radiologic Outcome
Univariate logistic regression analysis for final infarct volume demonstrated a negative association between final infarct size and ASPECTS, CBS, and CS (P < .0001 for all variables). Baseline CBF, CBV, MTT, and baseline NIHSS score were positively associated with final infarct outcome (P < .0001 for all). Baseline ASPECTS (P = .02), CBS (P = .03), CBV (P = .002), and CS (P = .04) were associated with final infarct size on multivariate linear regression analysis. Patients with CBS >6 achieved higher recanalization rates (71%) with rtPA than CBS ≤6 (44%) (P = .04; OR, 3.2; 95% CI, 1.1–9.4) (Table 5)
Interobserver Agreement
There was very good interobserver correlation for CBS (ICC, 0.97; 95% CI, 0.95–0.98) and CS (ICC, 0.87; 95% CI, 0.80–0.91).
Discussion
CTA-derived assessment of clot extent (CBS) is an independent predictor of clinical and radiologic outcomes in acute MCA territory stroke. Patients with smaller clot extent are more likely to have smaller baseline infarcts and lower baseline NIHSS scores, achieve a good clinical outcome, and have smaller final infarct size. Recanalization rates are also higher following intravenous rtPA in patients with smaller clot extent. A CBS threshold of >6 has a modest sensitivity and specificity and could be considered an adjunct to other imaging and clinical features, including baseline NIHSS and ASPECTS. CS predicts final infarct size but does not independently predict clinical outcome. CBS and CS demonstrate high interobserver reliability.
Many stroke physicians rely predominantly on clinical data such as baseline NIHSS score and time of symptom onset when deciding whether to perform thrombolysis in patients presenting with strokelike symptoms within accepted treatment time windows. Imaging data are often limited to an NCCT to determine infarct extent and presence of hemorrhage. In stroke centers and recent trials, increasingly advanced CT- and MR imaging−based strategies are being considered to stratify patient risk better.28,29 A recent publication, for example, defined infarct core and mismatch sizes associated with poor outcome or showing little benefit following thrombolysis.29 Proximal clot location is increasingly appreciated as an important determinant in outcome.3,30-32 Patients with a larger clot burden have been shown to have larger infarction volumes at baseline and poorer clinical outcomes.33,34 The CBS is designed to be weighted to vessel location, assigning higher points to the terminal ICA and proximal MCA locations. However, by distinguishing proximal and distal MCA and ICA locations and number of M2 branches affected, the score also accounts for clot extent (Fig 4).
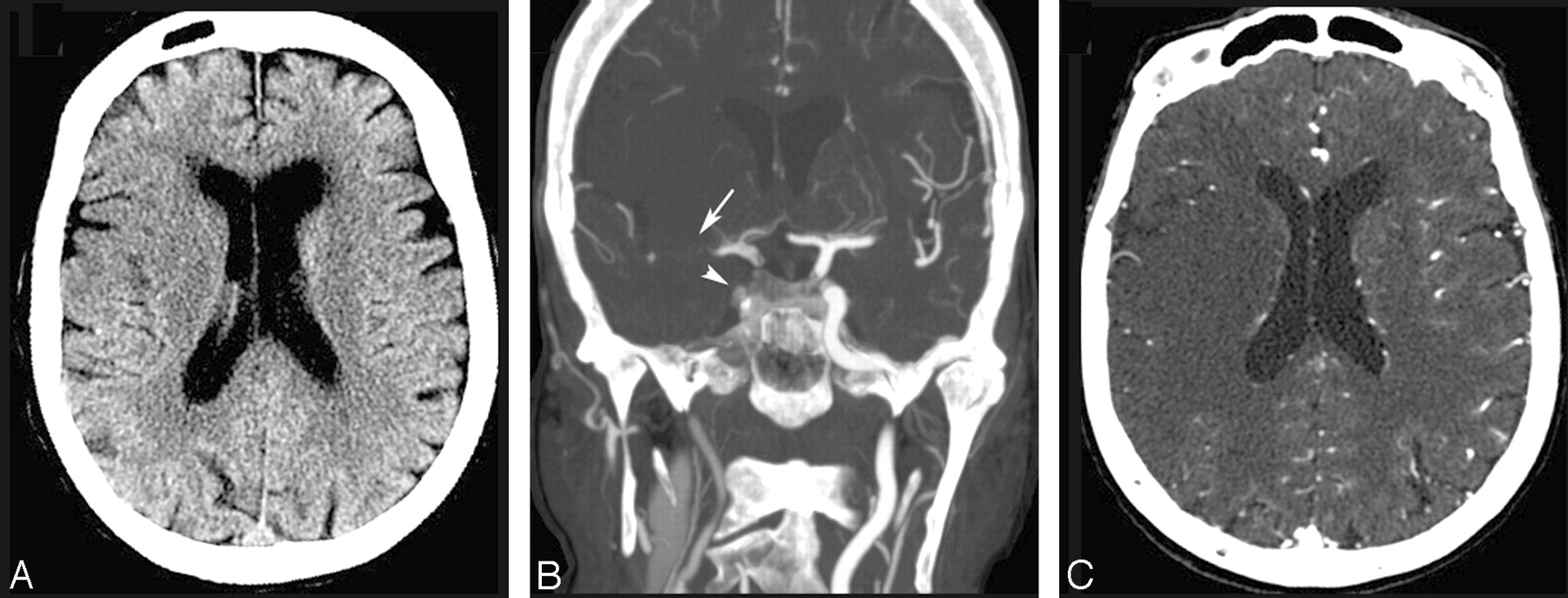
An 88-year-old woman presented with left-sided weakness treated with intravenous rtPA without recanalization. A, Noncontrast head CT scan demonstrates loss of gray-white matter differentiation within the right frontal lobe and caudate body with an ASPECTS of 3 and a baseline NIHSS score of 17. B, Coronal MIP image demonstrates poor contrast opacification of right supra- and infraclinoid ICAs (arrowhead) and M1 segment extending into the proximal M2 branches (arrow), scoring a CBS of 1. C, Axial CTA source image demonstrates a CS of 1. The patient was not treated with thrombolysis, was not recanalized, and achieved an mRS score of 4 at 90 days.
An increasing number of established and emerging vessel recanalization techniques are available, including intravenous and intra-arterial thrombolysis, mechanical thrombectomy devices, and low-frequency pulsed-waved transcranial Doppler sonography.7,8,35,36 Recanalization rates are known to vary according to thrombus location, which is often a reflection of thrombus extent. Recently, occlusion length has been shown to be an important determinant of the efficiency and complication rates in mechanical thrombectomy.5 Higher rates of recanalization are often achieved with more invasive techniques, though at the cost of increased complications, including parenchymal hemorrhage37and vessel injury/rupture.38 Rates of intravenous rtPA recanalization for isolated MCA occlusion are reported at 39%, compared with 9% for tandem ICA and MCA occlusion.9 These results are consistent with our observations that a lower CBS is associated with lower intravenous recanalization rates and suggest the need for a stratified treatment response according to the site of vessel occlusion and clot extent. A rapidly applied and reproducible scoring system that enables patient stratification in combination with established parameters such as ASPECTS, NIHSS score, and perfusion deficit is desirable. We propose that identification of patients with a larger thrombus extent could allow patient selection for more aggressive recanalization strategies in those centers where intra-arterial thrombolysis does not routinely follow intravenous rtPA use.
Several studies have established the importance of collateral supply in the prediction of stroke outcome by means of final infarct volume and functional outcome.4,39,40 Without adequate collateral flow, irreversible neuronal damage occurs within minutes.41 Collateral supply helps to prevent or limit the extent of infarction until recanalization facilitates ischemic penumbra reperfusion.21 Collateral supply plays a pivotal role in the pathophysiology of cerebral ischemia but is difficult to quantify due to its diminutive and complex routes. Although somewhat crude, the CTA-derived CS provides a simple and reproducible assessment of collateral supply22 and confirms the association between smaller infarct volumes and good collateral supply.
Outcome results in this study are limited by their applicability only to patients treated with intravenous rtPA or receiving no thrombolytic treatment. Different thresholds may exist for patients in those centers that follow the Interventional Management of Stroke protocol, where patients are transferred immediately to the angiographic suite for intra-arterial intervention after a bridging dose of intravenous rtPA. This limitation reflects a lack of a dedicated neuroangiographic suite and difficulty in emergent anesthesia access in the authors’ center. However, despite theoretically more rapid time to recanalization, the impact of an intra-arterial approach remains dependent on baseline infarction volume, which, in turn, is determined by the interplay between clot extent/location and collateral supply. The study is limited by heterogeneity in treatment, follow-up technique, and time to treatment, which are common limitations in a clinically managed cohort of patients. CT perfusion representation of initial infarct is limited to 8-cm coverage in this study; however, good correlation has been found between baseline CT and MR perfusion parameters and final infarct volume.42,43 Furthermore, given the constraints on imaging and the lack of continuous arterial monitoring, the exact time of recanalization within 24 hours of presentation cannot be determined with certainty.
In conclusion, many important radiologic and clinical predictors have been studied to help determine favorable clinical outcome in acute stroke. The factors are used clinically to stratify treatment options and enable the clinician to ensure that patients and their relatives are adequately informed before the consent process.44-46 Clearly, no single parameter can predict outcome accurately, and it is clear that a predictive model must incorporate a number of easily derived and reliable factors. The importance of these factors varies temporally with increased time from ictus. We have demonstrated the correlation between a novel CTA-derived score of clot extent and CT-derived perfusion parameters. Furthermore, we show in an independent patient cohort that a baseline scan assessment of CS and CBS adds additional prognostic information. Whether these results could facilitate the choice of route and type of thrombolytic treatment remains to be determined.
Acknowledgments
We gratefully acknowledge the hard work, efficiency, and devotion of our imaging technicians, which made this work possible. We thank V. Li for assistance with data management.
References
- Received July 7, 2008.
- Accepted after revision October 17, 2008.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Hyperperfusion and Blood-Brain Barrier Disruption beyond the Diffusion-Restricted Infarct 1 Day after Successful Mechanical Thrombectomy
- Magnitude of systolic blood pressure reduction following endovascular treatment and clinical outcomes in acute large artery occlusion stroke
- Clinical uncertainty in large vessel occlusion ischemic stroke: does automated perfusion imaging make a difference? An intra-rater and inter-rater agreement study
- Association between basal ganglia infarction and hemorrhagic transformation after mechanical thrombectomy in acute ischemic stroke: insights from the DIRECT-MT trial
- Estimating Flow Direction of Circle of Willis Using Dynamic Arterial Spin-Labeling MR Angiography
- Association of Carotid Artery Disease with Collateralization and Infarct Growth in Patients with Acute Middle Cerebral Artery Occlusion
- Correspondence on 'Predictors for large vessel recanalization before stroke thrombectomy: the HALT score by Colasurdo et al
- Clinical Uncertainty In Large Vessel Occlusion Ischemic Stroke (CULVO): An Intrarater And Interrater Agreement Study
- Brain-derived Tau for Monitoring Brain Injury in Acute Ischemic Stroke
- Alberta Stroke Program Early CT Score and collateral status predict target mismatch in large vessel occlusion with delayed time windows
- Predictors and outcome of early neurological deterioration after endovascular thrombectomy: a secondary analysis of the DIRECT-MT trial
- Pretreatment and interventional parameters predict excellent recanalization of large vessel occlusion in patients with acute ischemic stroke
- Collateral status and recanalization after endovascular treatment for acute ischemic stroke
- Factors associated with unfavorable outcome after anterior circulation stroke despite successful reperfusion and early neurological improvement
- Benefit of successful reperfusion achieved by endovascular thrombectomy for patients with ischemic stroke and moderate pre-stroke disability (mRS 3): results from the MR CLEAN Registry
- Hyperacute Perfusion Imaging Before Pediatric Thrombectomy: Analysis of the Save ChildS Study
- Management of extracranial carotid artery stenosis during endovascular treatment for acute ischaemic stroke: results from the MR CLEAN Registry
- mTICI 1 vs mTICI 0 before endovascular stroke treatment in middle cerebral artery M1-occlusion - predictor for revascularization success and outcome?
- Endovascular treatment beyond 24 hours from the onset of acute ischemic stroke: the Italian Registry of Endovascular Thrombectomy in Acute Stroke (IRETAS)
- Delayed CTP-Derived Deep Venous Outflow: A Novel Predictor of Striatocapsular Infarction after M1 Thrombectomy
- Comparison between collateral status and DEFUSE 3 or DAWN criteria in patient selection for endovascular thrombectomy within 6-24 hours after stroke: a protocol for meta-analysis
- Time Since Stroke Onset, Quantitative Collateral Score, and Functional Outcome After Endovascular Treatment for Acute Ischemic Stroke
- Circle of Willis variation and outcome after intra-arterial treatment
- Rescue Stenting in Mechanical Thrombectomy Refractory Occlusions: A Single Center Multiethnic Cohort
- Predictors of futile recanalization in patients undergoing endovascular treatment in the DIRECT-MT trial
- Quantitative Collateral Assessment on CTP in the Prediction of Stroke Etiology
- Collateral status and recanalization after endovascular treatment for acute ischemic stroke
- Early recanalization in large-vessel occlusion stroke patients transferred for endovascular treatment
- Benefit of successful reperfusion achieved by endovascular thrombectomy for patients with ischemic stroke and moderate pre-stroke disability (mRS 3): results from the MR CLEAN Registry
- Characterization of Subarachnoid Hyperdensities After Thrombectomy for Acute Stroke Using Dual-Energy CT
- Cerebrovascular Collateral Integrity in Pediatric Large Vessel Occlusion: Analysis of the Save ChildS Study
- Reduced Leukoaraiosis, Noncardiac Embolic Stroke Etiology, and Shorter Thrombus Length Indicate Good Leptomeningeal Collateral Flow in Embolic Large-Vessel Occlusion
- Endovascular treatment in anterior circulation stroke beyond 6.5 hours after onset or time last seen well: results from the MR CLEAN Registry
- Radiology-Pathology Correlations of Intracranial Clots: Current Theories, Clinical Applications, and Future Directions
- Hypoperfusion Intensity Ratio Correlates with CTA Collateral Status in Large-Vessel Occlusion Acute Ischemic Stroke
- Absent Cortical Venous Filling Is Associated with Aggravated Brain Edema in Acute Ischemic Stroke
- Small thrombus size, thrombus composition, and poor collaterals predict pre-interventional thrombus migration
- Systematic review protocol to assess artificial intelligence diagnostic accuracy performance in detecting acute ischaemic stroke and large-vessel occlusions on CT and MR medical imaging
- Prediction of Clinical Outcome in Patients with Large-Vessel Acute Ischemic Stroke: Performance of Machine Learning versus SPAN-100
- Distal Vessel Imaging via Intra-arterial Flat Panel Detector CTA during Mechanical Thrombectomy
- Association of White Matter Lesions and Outcome After Endovascular Stroke Treatment
- Clot Burden Score and Collateral Status and Their Impact on Functional Outcome in Acute Ischemic Stroke
- Endovascular treatment in older adults with acute ischemic stroke in the MR CLEAN Registry
- Artificial intelligence to diagnose ischemic stroke and identify large vessel occlusions: a systematic review
- Anesthetic management during endovascular treatment of acute ischemic stroke in the MR CLEAN Registry
- Greater infarct growth limiting effect of mechanical thrombectomy in stroke patients with poor collaterals
- Impact of single phase CT angiography collateral status on functional outcome over time: results from the MR CLEAN Registry
- Clot Burden Score and Early Ischemia Predict Intracranial Hemorrhage following Endovascular Therapy
- Inter- and intraobserver reliability for angiographic leptomeningeal collateral flow assessment by the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology (ASITN/SIR) scale
- Guidelines for evaluation and management of cerebral collateral circulation in ischaemic stroke 2017
- Value of Contrast-Enhanced MRA versus Time-of-Flight MRA in Acute Ischemic Stroke MRI
- Republished: Natures Wastebasket: The Role of the External Carotid Artery in Acute Stroke
- Similar Outcomes for Contact Aspiration and Stent Retriever Use According to the Admission Clot Burden Score in ASTER
- Value of Quantitative Collateral Scoring on CT Angiography in Patients with Acute Ischemic Stroke
- Impact of time to endovascular reperfusion on outcome differs according to the involvement of the proximal MCA territory
- Endovascular treatment for acute ischaemic stroke in routine clinical practice: prospective, observational cohort study (MR CLEAN Registry)
- Erythrocyte Fraction Within Retrieved Thrombi Contributes to Thrombolytic Response in Acute Ischemic Stroke
- Vulnerability to Infarction During Cerebral Ischemia in Migraine Sufferers
- Associations Between Collateral Status and Thrombus Characteristics and Their Impact in Anterior Circulation Stroke
- Opercular Index Score: a CT angiography-based predictor of capillary robustness and neurological outcomes in the endovascular management of acute ischemic stroke
- Association of clot burden score with radiographic and clinical outcomes following Solitaire stent retriever thrombectomy: analysis of the SWIFT PRIME trial
- Tissue-Selective Salvage of the White Matter by Successful Endovascular Stroke Therapy
- CT angiography-based collateral flow and time to reperfusion are strong predictors of outcome in endovascular treatment of patients with stroke
- Prediction of Clinical Outcome After Acute Ischemic Stroke: The Value of Repeated Noncontrast Computed Tomography, Computed Tomographic Angiography, and Computed Tomographic Perfusion
- The Impact of Conscious Sedation versus General Anesthesia for Stroke Thrombectomy on the Predictive Value of Collateral Status: A Post Hoc Analysis of the SIESTA Trial