
Abstract
BACKGROUND AND PURPOSE:Patients with symptomatic atherosclerotic stenosis of the intracranial vertebrobasilar artery (VBA) have a poor prognosis, and those with coexistent intracranial and extracranial stenoses have worse outcomes despite medical therapy. Our aim was to study the long-term outcome of patients with symptomatic atherosclerotic tandem stenoses at the intracranial VBA and the vertebral artery ostium (VAO) after elective stent placement.
MATERIALS AND METHODS:Ten consecutive patients (mean age, 65.3 years) with this condition underwent elective stent placement at our institution between September 2001 and December 2007. Technical success was defined as stent placement of both VAO and intracranial VBA stenoses with complete stent coverage of the lesions, residual stenosis of ≤30%, and good antegrade blood flow. The study end point was a composite of any stroke or death within 30 days and ischemic stroke in the VBA territory after 30 days.
RESULTS:Technical success was obtained in 9 of 10 patients without any stroke or death within 30 days. During a median follow-up duration of 32 months, 1 patient had a fatal ischemic stroke in the VBA territory at 4 months, and the other 9 patients were free from stroke recurrence. Thus, the annual stroke rate in VBA territory (including any stroke or death within 30 days) was 3.8%.
CONCLUSIONS:This pilot study shows that elective stent placement for patients with symptomatic atherosclerotic tandem stenoses at the intracranial VBA and VAO has an acceptable long-term outcome and may be considered as an alternative to medical therapy.
Patients with symptomatic atherosclerotic stenosis of the intracranial vertebrobasilar artery (VBA) have a poor prognosis,1–3 and those with coexistent intracranial and extracranial stenoses have worse outcomes, despite medical therapy.4 In the last decade, stent placement has increasingly been used to recanalize large- and medium-sized supply arteries of the brain. Some case series have shown the safety and feasibility of stent placement for patients with stenosis of either the extracranial vertebral artery (VA) or the intracranial VBA alone,5–7 but, to our knowledge, relevant reports regarding the outcome of stent placement for symptomatic tandem lesions in the intracranial VBA and VA ostium (VAO) are lacking. Our aim was to study the long-term outcome of patients with such posterior circulation tandem stenoses after elective stent placement.
Materials and Methods
Patients
Between September 2001 and December 2007, 132 consecutive patients with symptomatic atherosclerotic stenosis of the intracranial VBA underwent elective angioplasty with a balloon-expandable stent at our institution. Of them, 10 patients (9 men, 1 woman) with a mean age of 65.3 years (range, 49–79 years) were identified as having tandem stenoses of the intracranial VBA and VAO. Six of the 10 patients had intracranial VA and ipsilateral VAO tandem stenoses, with occluded contralateral VAs. The other 4 had basilar artery (BA) and access VAO tandem stenoses, whose contralateral VA was either occluded (n = 2) or hypoplastic with stenosis of 50% and 90% (n = 2). Six patients also had coexistent arterial stenosis of ≥50% in the anterior circulation. The patients’ baseline characteristics were prospectively collected and shown in Table 1. Warfarin-Aspirin Symptomatic Intracranial Disease (WASID) criteria were used to quantify the percentage of stenosis at the intracranial VBA,8 and North American Symptomatic Carotid Endarterectomy Trial criteria, at the VAO.9
Patients’ baseline characteristics
Stent placement protocol was approved by the ethics committee of our institution, and each patient provided written informed consent. Patients were given 30-mg aspirin plus 75-mg clopidogrel daily (n = 7) or 300-mg aspirin daily plus 250-mg ticlopidine twice daily before 2004 (n = 3), at least 7 days before the operation. The antiplatelet therapies were continued for ≥6 months after the operation. Atherosclerotic risk factors were managed according to America Heart Association guidelines.10 Intravenous nimodipine was routinely infused 2 hours before stent placement and lasted 24 hours after stent placement, at a rate of 0.6–2 mg per hour adjusted according to blood pressure.
Interventional Procedure
The stent-placement procedure was performed under local anesthesia in all patients (n = 9), except 1 patient who received general anesthesia due to a small access vessel. During the operation, the patients received 2000- to 3000-U heparin as an intravenous bolus, followed by 500–800 U per hour intravenous infusion, similar to the protocol described in the Prolyse in Acute Cerebral Thromboembolism II trail.11 A 6F Envoy (Cordis, Miami Lakes, Fla) guiding catheter was used to deliver the stent system via the femoral (n = 9) or brachial artery (n = 1). Quantitative angiography was performed by using the diameter of the catheter as a reference to size up the stents required. For the VAO lesion, the stent-to-normal-vessel diameter ratio was 1.1:1 or 1:1. The length of the stent had to cover 3–5 mm of normal vessel segment distal to the stenosis and to protrude 1–2 mm into the subclavian artery (SA) proximally. For the intracranial VBA lesion, the stent diameter was undersized with a stent-to-normal-vessel ratio of 0.9:1.
Direct VAO stent placement without balloon predilation was performed in all patients to prevent a large debris embolization. VAO stenosis was first treated with a balloon-expandable stent in 7 patients. Following this, attempts were made to advance the guiding catheter through the VAO stent into the V2 segment of the VA. A 0.014-inch microguidewire was used to cross the intracranial VBA lesion. The balloon-expendable stent system was delivered to the intracranial VBA lesion over the microguidewire and released by slow balloon inflation. In 3 other patients, the guiding catheter was advanced into the V2 segment of the VA to stent the intracranial VBA lesion before VAO stent placement. These 3 patients had a large-enough residual lumen of access VAO to accommodate the guiding catheter without obstructing antegrade VA blood flow. Technical success was defined as stent placement of both VAO and intracranial VBA stenoses with complete stent coverage of the lesions, residual stenosis of ≤30%, and good antegrade blood flow.
Study End Point
The end point was composite of stroke or death from any cause within 30 days and ischemic stroke in the VBA territory 30 days after the procedure. This was assessed by a stroke neurologist. Stroke definition was the same as in a previous study.5 Patients were followed up by a stroke clinic and telephone interview. A patient's independence was defined as modified Rankin Scale (mRS) score of ≤2 at final follow-up.
Catheter angiography was repeated on a voluntary basis. Restenosis was defined as in-stent diameter narrowing of ≥50%. Analyses were performed on an intention-to-treat principle.
Results
Procedural characteristics, including stents used, are detailed in Table 2. The overall technical success rate was 90% (9 of 10 patients). VAO stent placement was successful in all patients, and intracranial VBA stent placement was successful in 9. The guiding catheter could not be advanced into the VA in 2 patients whose VAO lesions were stented first. Intracranial VBA stent placement was successful in 1 of these 2 patients (case 7), with the guiding catheter placed at the SA, but failed in another patient (case 4) because the microguidewire could not cross the intracranial lesion. Additionally, 2 patients underwent simultaneous stent placement of the contralateral VAO (case 6) and the right intracranial internal carotid artery (case 10). Both of them were uneventful.
Procedural characteristics and follow-up outcomes
There was no periprocedural death or stroke within 30 days in all patients, including a failed procedure (case 4). During a median follow-up duration of 32 months (range, 4–59 months; total, 26.25 patient-years), only the patient (case 4) whose intracranial VBA stent placement failed had a fatal ischemic stroke in the VBA territory at 4 months. The other 9 patients were free from stroke in either the VBA or anterior circulation territory. Thus, the VBA territory stroke rate (including any stroke or death within 30 days) was 3.8 per 100 patient-years. All surviving patients were independent at final assessment. Follow-up catheter angiograms were available in 4 patients at 6–8 months, which showed no restenosis.
Discussion
The long-term outcome of our patients with symptomatic atherosclerotic tandem stenoses of the intracranial VBA and VAO after elective balloon-expandable stent placement appears better than the natural history of isolated intracranial VBA stenosis. The annual stroke rate of VBA territory was 3.8% for our patients. Two retrospective studies showed a higher annual stroke rate of 6.2% and 8.7% in the VBA territory for patients with symptomatic intracranial VBA stenosis of ≥50% while on antithrombotic therapy.1,2 A recent prospective study, the WASID trial,3 also revealed a higher annual stroke risk (8.3%) in the stenotic artery territory for patients with symptomatic intracranial stenosis of ≥50%, despite aspirin treatment. Furthermore, multiple stenoses in the posterior circulation are frequent, accounting for 36.4% of patients in a posterior circulation stroke registry study,12 and the prognosis of patients with concurrent intracranial and extracranial stenoses was worse as shown in a Chinese stroke population study.4
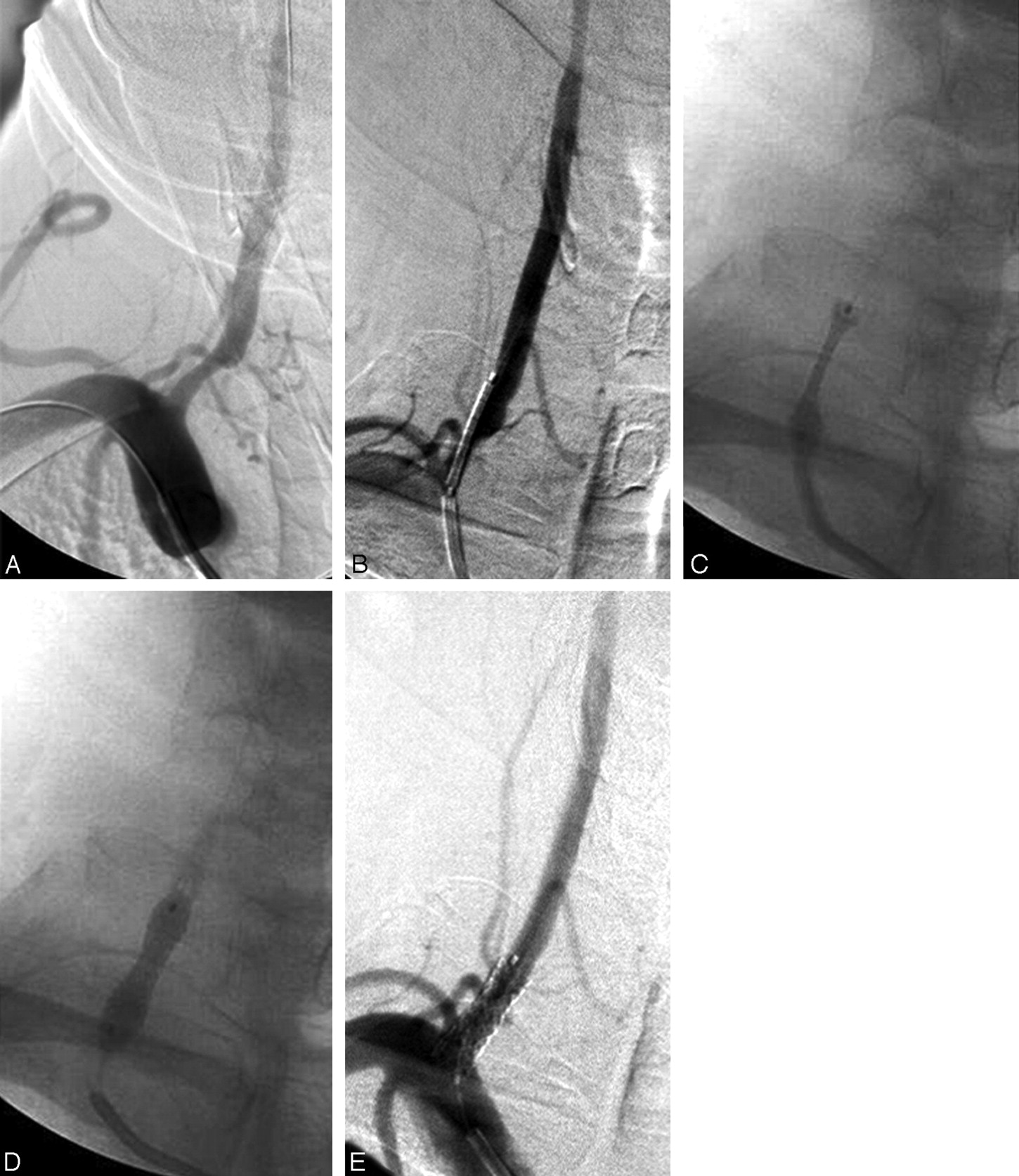
A stent-placement procedure of intracranial VBA and VAO tandem stenoses is technically more complicated than that of an isolated stenosis. There is no standardized interventional approach that would fit all patients. The VAO lesion can be stented first to ensure good antegrade blood flow and to avoid dislodging plaque from the VAO lesion (because it has been covered by the stent); then the guiding catheter is advanced into the VA to treat the intracranial lesion subsequently. Indeed, placement of a guiding catheter into the VA after VAO stent placement is one of the most technically challenging aspects of the procedure. Accurate placement of the VAO stent that protrudes 1 or 2 mm into the SA is crucial. A poorly placed VAO stent protruding more than this length could thwart further intracranial intervention because it would become very hard for one to steer the guiding catheter through it. Hence, meticulous care should be taken to prevent the VAO stent from sliding backward toward the subclavian artery during its opening, the so called “watermelon-seeding effect.”13 One way to prevent this is to support and stabilize the unopened balloon-expandable stent system from below by placing the proximal 1–2 mm of the uninflated balloon within the distal guiding catheter, just enough to anchor the balloon without constraining the stent segment. This is followed by slowly inflating the balloon with low pressure (eg, 5–6 atm) until the stent is visibly expanded at both ends, resembling the shape of a dumbbell on fluoroscopy (Fig 1). The guiding catheter is then slightly withdrawn after deflating the balloon, followed by re-inflating the balloon at a higher pressure (eg, 9–11 atm) to open up the stent fully and completely.

Case 9. A, A 6F guiding catheter placed at the right SA near the right VA ostium of 50% stenosis. B, Proximal end of the uninflated balloon anchored in the guiding catheter. The stent segment remains outside the catheter. C, The stent opening at first inflation resembles the shape of a dumbbell. D, The guiding catheter is pulled back to allow a second full inflation. E, Complete resolution of the stenosis.
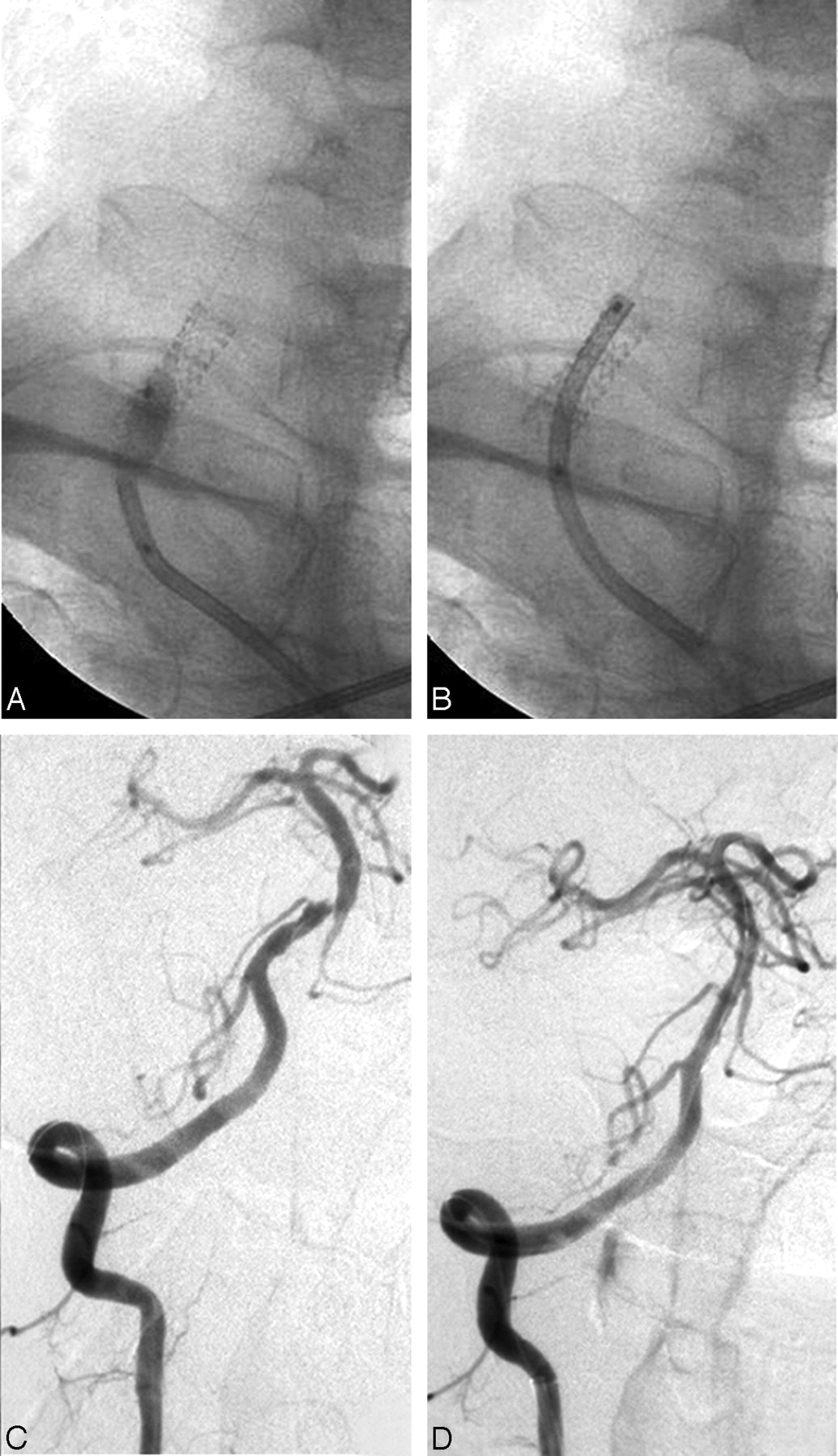
Despite a well-placed VAO stent, advancement of a guiding catheter into the VA could still be a challenge in patients whose V1 segment is obtusely angulated away from the SA. In this situation, a partially re-inflated balloon within the VAO stent may act as a flexibly shaped “cushion” to help steer the guiding catheter into the VA (Fig 2). The stopcock connected to the balloon inflation port needs opening to allow the balloon to deflate as the catheter envelops it and is advanced through VAO. Despite these measures, we were unable to place the guiding catheter into the VA in 2 of 7 patients after VAO stent placement. This contributed to subsequent failure of the intracranial VBA stent placement in 1 patient.

Case 9. A, The guiding catheter is steered into the right extracranial VA with the aid of a partially re-inflated balloon within the stent at the VAO. B, The balloon was deflated as the catheter envelopes it within the VAO stent. C, The tip of the guiding catheter is placed at the distal V2 segment for stent placement of a short-segment stenosis (80%) in the BA. D, Resolution of the stenosis.
Another option is to insert the guiding catheter into the VA and to stent the intracranial lesion up front, provided that the residual lumen of the access VAO is large enough to accommodate a 6F catheter as in 3 of our patients (cases 2, 5, and 6). This approach may carry an increased risk of embolic stroke for the reasons mentioned above, but it, fortunately, did not occur in our patients. A compromised alternative, which was not used in our patients, would be to perform VAO balloon angioplasty first, together with an embolic protective device (EPD). The guiding catheter could then be advanced into the VA over the balloon catheter and EPD guidewire. The intracranial stenosis would be stented next, followed by VAO stent placement after retreating the guiding catheter into the SA.
There were a few limitations in this pilot study. First, it was not a randomized controlled study. It could not confirm the efficacy of stent placement compared with medical therapy directly. Second, because the sample size was small and the number (40%) of digital subtraction angiography follow-ups was limited in this cohort, the reported poststenting stroke and restenosis rate may be underestimated by chance.
Conclusions
This pilot study shows that stent placement of symptomatic atherosclerotic tandem stenoses of the intracranial VBA and VAO appears feasible and safe when performed at experienced centers; it has an acceptable long-term outcome and may be considered as an alternative to medical therapy. Further study of a larger patient population with long-term clinical and angiographic follow-up is needed.
Footnotes
This work was supported by the Ministry of Health of the People's Republic of China (2004BA714B-7).
References
- Received August 25, 2008.
- Accepted after revision October 25, 2008.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}