
We read with interest the article by de Souza et al1 about the use of susceptibility-weighted imaging (SWI) for the evaluation of patients with cerebral cavernous malformations (CCMs). In this regard, we would like to report the following case: In November 2008, a 38-year-old woman presented with a history of left tinnitus and hypoacusis. The usual MR imaging sequences showed a left acoustic neurinoma; she also was found to have a single CCM in the left frontal region as an incidental finding. She underwent surgery, and a small CSF fistula presented through the surgical wound as complication. A new MR imaging was performed, adding SWI, showing several lesions that suggested the presence of multiple CCMs (in addition to the frontal cavernous malformation previously diagnosed) that were not seen on the usual sequences (Fig 1).
The clinical correlation with the patient's medical history and a thorough analysis of the images led to the suspicion that the lesions seen on SWI corresponded to extra-axial air collections. A second intervention to close the CSF fistula and remove the frontal cavernous malformation was performed without complications, and the patient was discharged shortly after.
SWI is a relatively new MR imaging technique suitable for detection of magnetic susceptibility effects.2 SWI is more sensitive than T2*-weighted gradient-refocused images in CCMs.1,3 SWI may prove to be outstandingly useful in identifying the true extent of cavernous malformations or in confirming the presence of suspected small CCMs.
However, as stated by Tong et al,4 the loss of signal intensity created by a disturbance of a homogeneous magnetic field seen on SWI can be caused by various paramagnetic, ferromagnetic, or diamagnetic substances such as iron, some forms of calcification, or even air. Additionally, this fact may suggest that SWI could be a suitable sequence for monitoring the progress of recovery from pneumocephalus in neurosurgical patients.

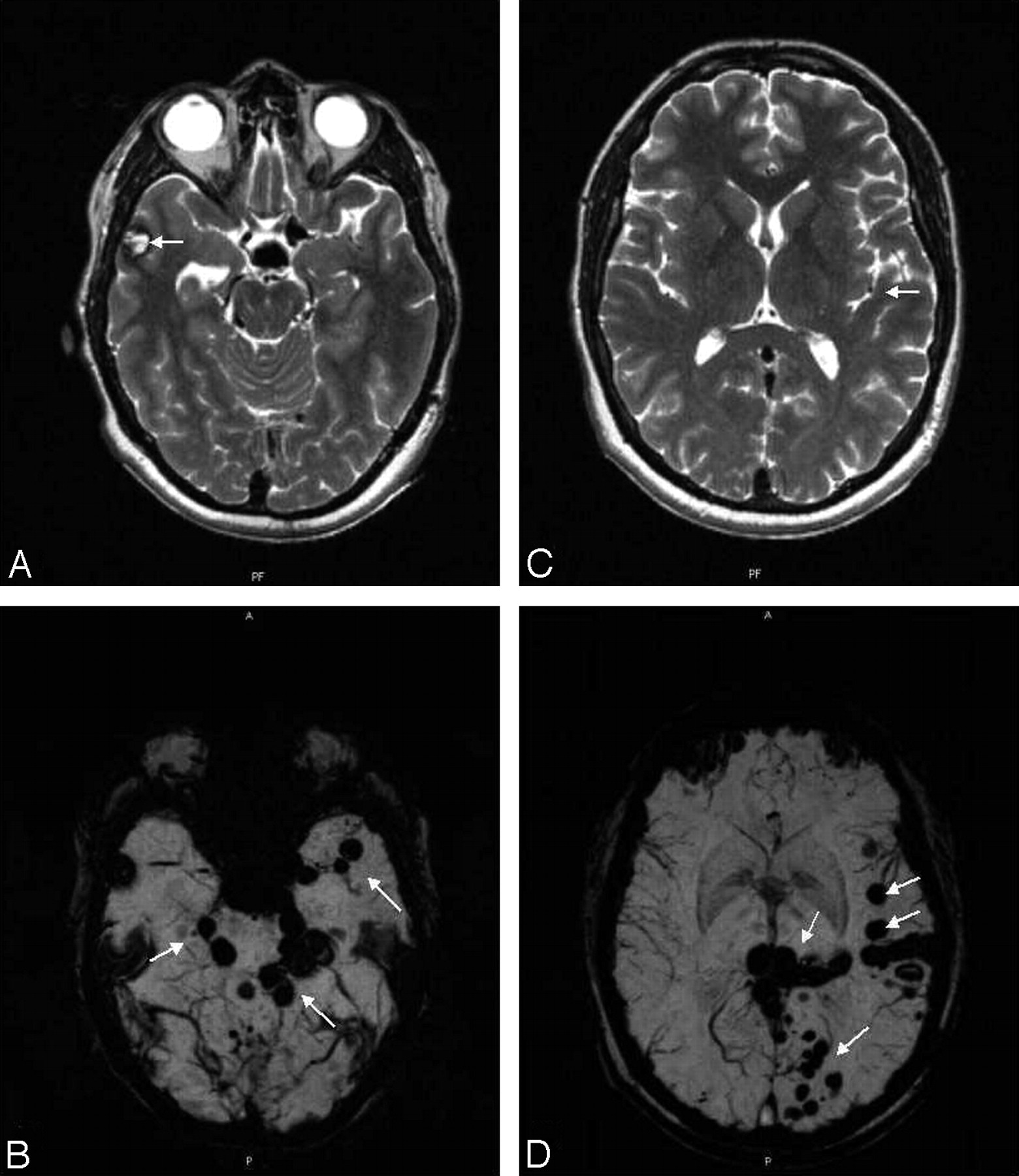
A, Axial T2-weighted image shows a right frontotemporal lesion with mixed signal intensity (arrow) suggesting a cavernous malformation. B, SWI confirms the right frontotemporal lesion and also demonstrates several lesions (arrows), all of them extra-axial. C, Axial T2-weighted image at an upper level shows no significant abnormalities except for a small focus of low signal intensity on the left opercular area (arrow). D, SWI demonstrates additional extra-axial foci (arrows), which are not seen on the T2-weighted image.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.