
Abstract
SUMMARY: Septations within cerebral arteries or aneurysms are exceedingly rare in the absence of associated fenestrations. We report an unusual unruptured pedunculated basilar apex aneurysm, with a “pseudoseptation” between the main aneurysmal sac and an anterior compartment, which was, in fact, represented by a perforation in the membrane of Liliequist, permitting anterior aneurysmal herniation into the carotid-chiasmatic cistern. The patient was successfully treated with detachable coils. This case is unusual on 2 accounts: 1) the aneurysm's appearance, and 2) the presence of a large fenestration in the membrane of Liliequist, of which anatomic features are herein reviewed.
Although intraluminal septations of cerebral arteries have been described by several anatomists,1 it is generally agreed that arterial dividing partitions are related to fenestrations, of which they may represent a “forme fruste.”1,2 From a theoretic standpoint, such septations could also involve arterial lesions such as aneurysms, especially because fenestrations predispose to aneurysmal formation.1,2 We report a basilar terminus aneurysm with an unusual horizontal orientation, and a “pseudoseptation” separating the main sac from a poorly opacified anterior part. This “pseudoseptum” was, in fact, caused by a herniation of the aneurysm through a perforated membrane of Liliequist. One commonly held belief about the membrane of Liliequist is that it is thick and is not fenestrated,3–8 contrary to the finding in this case.
Case Report
A 43-year-old right-handed female patient presented to the emergency department with severe headaches. Her medical history was only significant for mild chronic bifrontal headaches, self-treated with acetaminophen. Her general and neurologic examinations revealed no abnormalities. CT scan results revealed a suspicious hyperattenuated mass in the interpeduncular cistern (Fig 1), without subarachnoid hemorrhage or ventriculomegaly. Results of CSF analysis did not reveal xanthochromia. Cerebral angiography revealed a 10 × 7-mm aneurysm arising from the basilar apex, with a short pedicle, oriented cephalad and horizontally, and a blurred, flat anterior surface (Fig 2). The patient was counseled on the natural history of cerebral aneurysms and opted for endovascular therapy. At the time of treatment, the aneurysm was found to be compartmented, with a “pseudoseptum” separating a poorly opacified anterior sac (Fig 2). Sequential obliteration of the anterior compartment of the aneurysm (Fig 3A) and the posterior sac was performed (Fig 3B-C). A postoperative CT scan was obtained, not MR imaging. The patient's hospital course was uneventful. She later reported that her headaches had resolved. Follow-up angiography at 9 months showed persistent obliteration of the aneurysm.
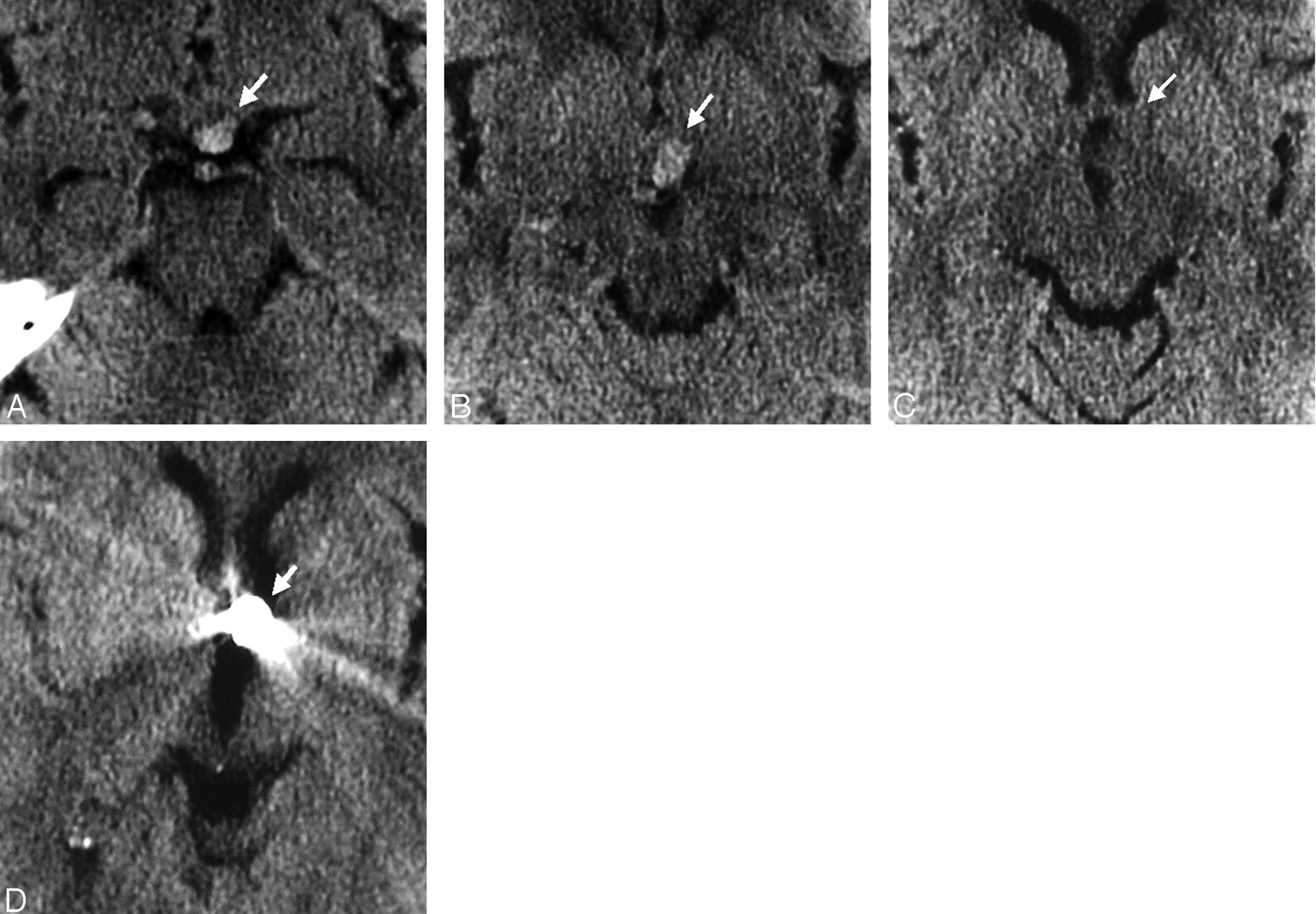
Axial noncontrast CT scan before treatment (A-C) and after treatment (D) shows the aneurysm extending from the prepontine and interpeduncular cisterns (A,B) to the left carotid-chiasmatic cistern lateral to the third ventricle (C), filled with platinum coils (D).

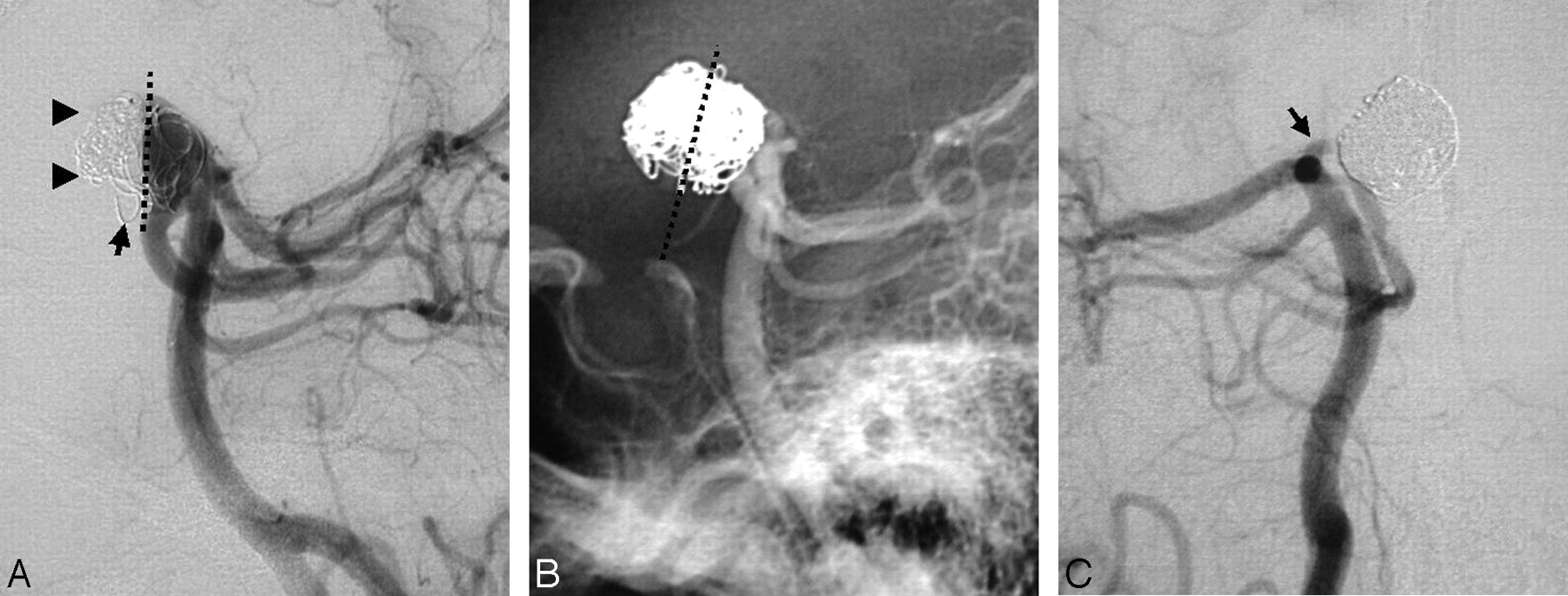
Posterior circulation angiogram shows an anteriorly pointing pedunculated basilar apex aneurysm. Lateral unsubtracted view (A) shows the flat anterior surface of the opacified aneurysmal sac (arrowheads), lying high relative to the clivus. Subtracted lateral (B) and anteroposterior oblique (C) views show the pedicle of the aneurysm (arrow) and a pseudoseptum with an anterior opening within the aneurysm (C; arrowheads).
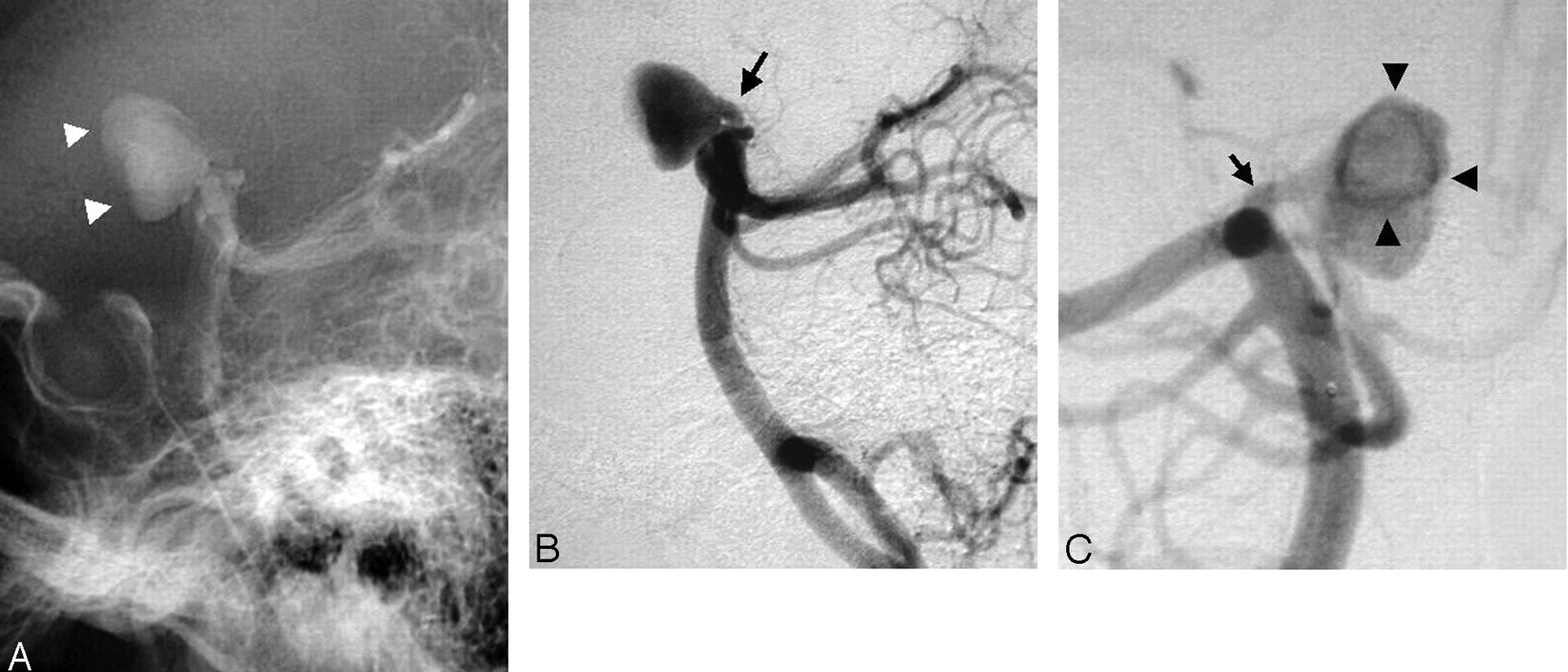
Angiogram, lateral oblique view during treatment (A) and lateral and oblique views after treatment of the aneurysm (B-C), show coil packing of the unopacified anterior aneurysmal sac (A; arrowheads), anterior to a line drawn along the theoretic course of the membrane of Liliequist (A,B; dotted line). After treatment, stagnant flow is noted in the pedicle of the aneurysm (C; arrow).
Discussion
Flattening of the anterior surface of the aneurysm in our patient was caused by an anatomic structure extending in the retroclival subarachnoid space, the membrane of Liliequist, which prevented anterior expansion of the aneurysm, with the exception of a herniated part (Figs 2 and 3). Although this membrane may be evaluated noninvasively with MR imaging techniques such as 3D Fourier transform constructive interference in the steady state,3 relatively little remains known about it.
The first anatomic description of the membrane of Liliequist is owed to the 19th century Swedish anatomists Axel Key and Gustaf Retzius,4 who were the first to show that the subarachnoid space was compartmentalized yet widely communicating. Bengt Liliequist, a Swedish radiologist who pioneered the technique of pneumoencephalography, noticed that the previously described membrane was able to prevent supratentorial passage of air from the interpeduncular cistern and left his name associated with that anatomic structure.4,10
The membrane of Liliequist is generally viewed as a continuous, unperforated, avascular fold of the tentorial arachnoid mater with a double layer, which arises from the arachnoid membrane of the dorsum sellae,5 and has 2 distinct sheets. The superior sheet (the diencephalic membrane)3,5–7 extends from the dorsum sellae superiorly to attach to the mamillary bodies in a premamillary4,7–8 or retromamillary11,12 position (Fig 3). The lower sheet (the mesencephalic membrane)3,5–7 extends posteriorly and inferiorly from the diencephalic membrane to attach to the pons and has openings for and attachments to the basilar artery and the superior cerebellar arteries.5,6 Structural differences exist between the relatively thin, trabecular mesencephalic membrane, which harbors perforations variable in number and size, and the diencephalic membrane, credited with a thick, continuous arachnoid structure.5,6 There is controversy as to the membrane's lateral attachment sites, whether these sites are in the medial surface of the temporal lobes8 or the pia surrounding the oculomotor nerves.11 Renewal of interest in the membrane of Liliequist has arisen from the practice of endoscopic procedures to treat hydrocephalus. A 25% failure rate of endoscopic third ventriculostomy procedures has been believed by some to be the result of lack of fenestration in the membrane of Liliequist, presumably preventing the expected outcome of free CSF flow from the third ventricle to the subarachnoid space.13,14
In our patient, although thick enough to flatten the anterior surface of the aneurysm, the diencephalic membrane harbored a wide fenestration, allowing anterior herniation into the carotid-chiasmatic cistern. Although arterial pulsations could have played a role for a long period, this finding contradicts the notion that the superior part of the membrane of Liliequist is not perforated.4–8
Conclusions
This report documents an unusual configuration of a pedunculated basilar apex aneurysm, with a pseudoseptated appearance between 2 aneurysmal compartments because of a large perforation in the membrane of Liliequist, which is generally considered not perforated.
References
- Received February 16, 2009.
- Accepted after revision March 10, 2009.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.