
Abstract
BACKGROUND AND PURPOSE: Fetal ventriculomegaly (VM) is important because of its high prevalence and high risk of association with other brain abnormalities. The purpose of this article was to investigate the hypotheses that including in utero MR imaging (iuMR) in the diagnostic pathway for fetuses with isolated VM on antenatal imaging will show other brain abnormalities in a high proportion of cases and that these will have a significant effect on clinical management.
MATERIALS AND METHODS: One hundred forty-seven pregnant women were recruited prospectively from 8 fetomaternal centers in Britain. All of the fetuses had VM diagnosed on sonography but no other abnormality. iuMR was performed, and the results of the examinations were compared with those of sonography. Two fetomaternal experts made independent assessments of the effects of any new diagnoses on clinical management.
RESULTS: Categoric assessments of ventricular size were the same in approximately 90% of fetuses. Other abnormalities were shown in 17% of fetuses. The most frequent additional brain abnormality shown on iuMR was agenesis of the corpus callosum. Severe VM was associated with an approximately 10-fold increase in the risk of another brain abnormality being present when compared with fetuses with mild VM. The most profound effects on clinical management, however, were found in cases of mild VM.
CONCLUSIONS: This work supports our hypotheses by showing a high detection rate of other brain pathology when iuMR was used to supplement antenatal sonography (17%). In a high proportion of cases, the detection of the extra pathology would have led to significant changes in clinical management.
Structural abnormalities of the fetus are investigated in many countries by using sonography, first by way of screening programs and then by detailed anomaly scanning if necessary. It is desirable to have as much anatomic information available as possible for the parents for 2 main reasons: First, finding no abnormality is of great comfort to parents, particularly if the fetus is at increased risk of malformation. Second, if abnormalities are found, the parents need as much accurate information as possible to assist in making decisions about the future of the pregnancy.
Abnormalities of the brain and spine are among the most common causes for concern in fetal imaging, and ventriculomegaly (VM) is one of the most frequent abnormal brain findings. The widely used definition of fetal VM is a transtrigone measurement of ≥10 mm at any stage of pregnancy.1–3 With that definition, VM is found in ≤2.5 per 1000 pregnancies.4 In some cases, VM is the only abnormal finding, leading to the term “isolated VM,” which is found in approximately 20% of all cases of fetal VM diagnosed on sonography (eg, 22% from 267 cases5 and 16% from 51 cases6). Fetuses with isolated VM are at an increased risk of aneuploidy,7 particularly trisomy 21, and amniocentesis is often offered for this reason.
It is important to recognize VM antenatally because it may be an indicator and/or manifestation of other serious central nervous system (CNS) abnormalities with values of 88% sensitivity in 1 study.8 Fetal VM is associated with poor outcome in terms of both mortality and morbidity if projected outcome data from termination of pregnancy cases are included.9 Once VM has been demonstrated on a screening sonography examination, women are referred to specialist fetal/maternal centers for further sonographic assessment, which includes detailed neurosonography by an expert in fetal imaging. The implications of detecting fetal VM are complicated because there are many underlying etiologies. Most authorities believe that if other structural CNS abnormalities are found in conjunction with VM, there is a high risk of a poor neurologic and/or developmental outcome. When VM is the only abnormal finding and the fetus is known to be euploid, counseling parents is partly based on the severity of the VM because increasing size of the ventricles is associated with a higher risk of poor outcome. The most recent data on outcome have used the results of in utero MR imaging (iuMR) to define isolated VM.10
The purpose of this study was to investigate the hypotheses that including iuMR in the diagnostic pathway for fetuses with isolated VM on antenatal imaging will show other brain abnormalities in a high proportion of cases and that these will have a significant effect on clinical management. We have attempted to quantify these potential benefits to management.
Materials and Methods
The study was approved by the South Sheffield Research Ethics Committee and sponsored by the Wellcome Trust, United Kingdom. None of the cases have been previously reported in our earlier publications on diagnostic accuracy assessment on iuMR.
Participants
One hundred forty-seven pregnant women were recruited from 8 tertiary fetal assessment units in England and Scotland. Entrance criteria for the study were the following: singleton pregnancy with fetal VM diagnosed on sonography (trigone measurement of ≥10 mm) referred to the study center at 20 weeks’ gestational age or later and no other abnormality of the fetus shown by sonography (brain or somatic) under good sonographic conditions (eg, no obscuration because of maternal body mass index problems, fetal position, or oligohydramnios). None of the fetuses had a known abnormality on karyotyping at the time of referral. The women did not have any known or suspected contraindications to MR imaging and agreed to provide written consent after full explanation by 1 of the authors. The women were not paid for their involvement in the study, but travel expenses were offered for themselves and a companion. Most iuMR examinations were performed within 4 days of the referral; exceptions included periods of machine breakdown and the referral being made before 20 weeks’ gestational age (in which case the examination was delayed to 20–21 weeks’ gestation). The study extended from 2005 to 2009.
Procedures
Our iuMR technique has been described in detail elsewhere11 but is summarized here. All images were acquired on a 1.5T scanner (either Infineon, Philips Medical Systems, Best, the Netherlands; or HDx, GE Healthcare, Milwaukee, Wisconsin). A flexible phased array body coil was attached around the lower abdomen, and a series of 3-plane scout views was obtained. Once the fetal head was located, single-shot fast spin-echo sequences were run by using the following typical parameters: TR, 20,000 ms; TEeff, 75 ms; echo-train length, 132; FOV, 25 cm; matrix size, 248 × 256; NEX, 1; FA, 120°. Twenty 5-mm-thick sections of the fetal brain were obtained (20-second acquisitions) in the 3 natural orthogonal planes. After these were judged to be of diagnostic quality, similar acquisitions were performed by using 3-mm-thick sections with TR, 31,416 ms; TEeff, 92 ms; echo-train length, 136; FOV, 25 cm; matrix size, 183 × 256; NEX, 1; refocusing angle, 120°. An axial gradient-echo T1-weighted sequence was acquired in 30-second acquisition time, either with or without suspended maternal respiration. The parameters for the T1 sequence were the following: TR, 238 ms; TE, 3.4 ms; refocusing angle, 70°; FOV, 23 cm; matrix size, 192 × 256; NEX, 1.
The iuMR images were reported for clinical purposes at the time of the examination but, for the purposes of this study, were later reviewed by a neuroradiologist experienced in iuMR brain studies (P.D.G.). The reviewer had access to the sonography report at the time of review but to no subsequent follow-up information. The size of the trigones of the lateral ventricles was determined on sonography on a standardized axial view by the referring fetomaternal expert. A similar assessment of the transverse diameter of the trigones of both lateral ventricles was performed on the axial MR images by 1 of 2 experienced operators (J.E.M. or M.J.R.). This was done in a blinded fashion—that is, the reviewers did not know the trigone measurements made on sonography when they made the measurements on the iuMR studies. The measurements made on sonography were compared with those obtained from iuMR on the basis of any change in categoric description: mild (10–12 mm), moderate (13–15 mm), and severe (≥16 mm) based on the size of the largest of the ventricles if asymmetric. The final categoric assignment was made on the basis of the MR imaging measurements. Any other brain abnormalities were recorded, and the results of the iuMR examination were passed on to the referring clinician. The pick-up rate of brain pathology other than VM on iuMR was taken to be an indicator of improved diagnostic accuracy when compared with sonography. The gestational age of the fetus at the time of referral for iuMR was used to divide the patients into 2 groups for further analysis: namely, those referred at 20–24 weeks’ gestational age (20–24 weeks’ group) and those referred at 25 weeks or after (25+ weeks; group).
We did not study the clinical significance of the results of iuMR in our patients in real-time; instead we made a retrospective assessment of possible effects on clinical management. This was performed by presenting the results of the sonographic and iuMR studies for each patient to 2 fetomaternal experts independently (G.M., S.A.R.). Each expert reported the change in management that would have been brought about by including iuMR in the diagnostic pathway, in their opinion. One of 4 categoric responses was used to define these data as described in the footnote of on-line Table 1, and their results are presented in on-line Tables 1 and 2.
Results for diagnostic agreement and the proportion of cases in which additional diagnostic information was found are expressed as percentages, with 95% confidence intervals (CI) estimated by using the binomial method.
Results
One hundred forty-seven consecutive singleton fetuses with apparent isolated VM were recruited, of which 99 were referred between 20–24 weeks and the remaining 48 referred at ≥25 weeks’ gestational age. Overall, the diagnosis of isolated VM was supported by iuMR in 122/147 (83%; 95% CI, 76%–89%) cases, while other brain abnormalities were shown on iuMR in 25/147 (17%). In the 122 cases of confirmed isolated VM, the categoric assessments of the largest trigone size made on sonography were compared with those made on iuMR. There was complete categoric agreement in 90% of cases (95% CI, 83%–95%). In the 12 cases with categoric disagreements, 2 fetuses were reclassified from mild VM on sonography to normal-sized ventricles on iuMR, 9 fetuses were reclassified from mild VM on sonography to moderate VM on iuMR, and 1, from moderate on sonography to severe on iuMR.
Twenty to 24 Weeks’ Group
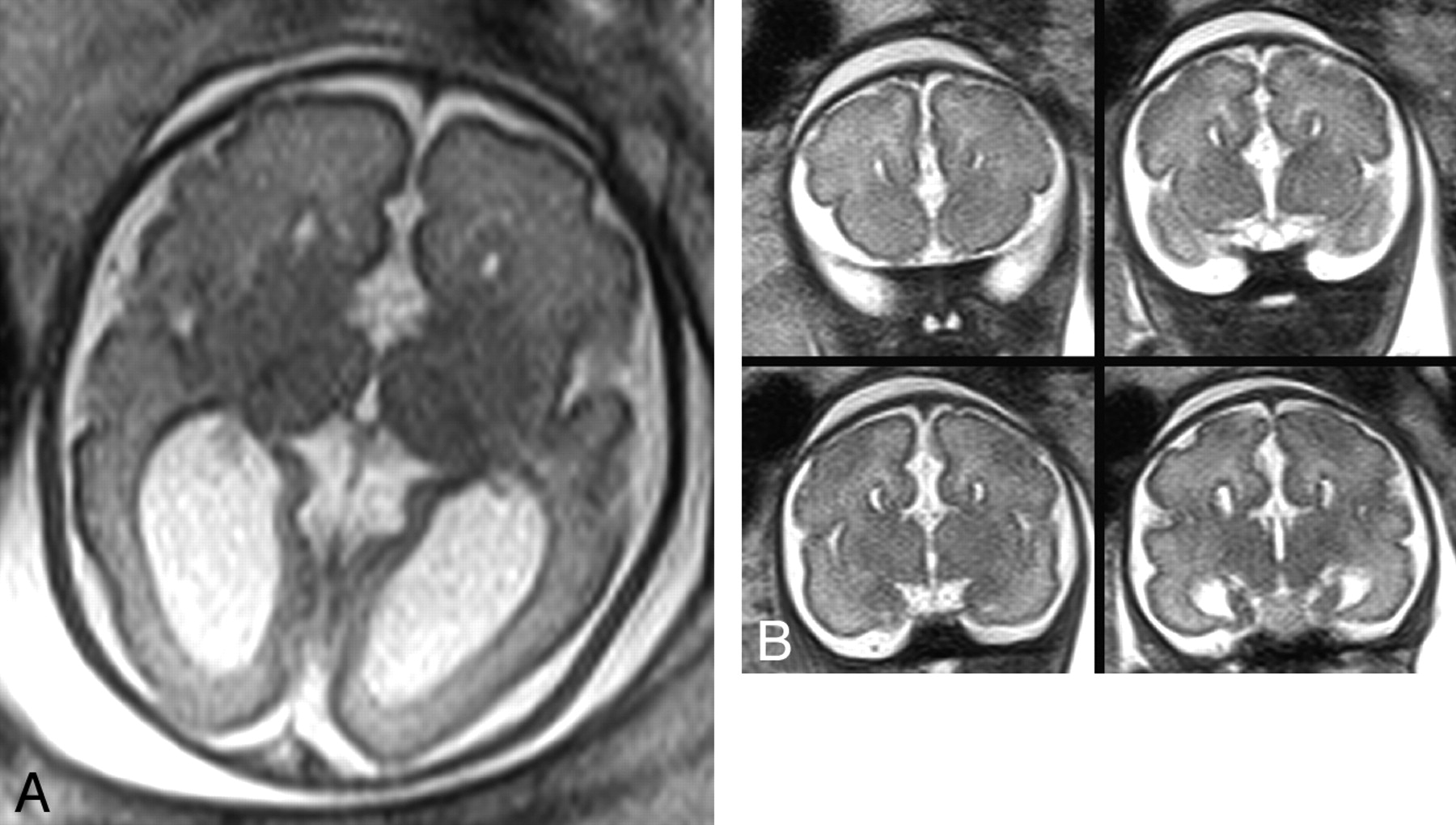
The median gestational age at the time of iuMR in this group was 22 weeks. Additional brain pathology was identified in 9/99 (9%; 95% CI, 4%–17%) fetuses imaged between 20 and 24 weeks’ gestational age. The categories of enlarged trigones (on the most severely affected side) in the 90 confirmed isolated VMs in fetuses of 20–24 weeks’ gestational age, according to iuMR, were the following: normal, 2/90; mild, 66/90; moderate, 15/90; and severe, 7/90. The additional brain abnormalities shown in the 9 fetuses of this subgroup are described in on-line Table 1 and consisted of developmental abnormalities in 8/9 fetuses. Failed commissuration (agenesis of the corpus callosum) was the most frequently found abnormality in fetuses with VM in the 20–24 weeks’ group (5/9). An example is shown in Fig 1 . The sizes of the enlarged trigones on the most severely affected side in the 9 fetuses with abnormal brains are shown in on-line Table 1, with most cases having mild VM.

In utero MR imaging (iuMR) scans of a fetus at 23 weeks’ gestational age thought to have isolated ventriculomegaly (VM) on sonography. A and B, Axial (A) and a montage of 4 consecutive coronal single-shot fast spin-echo images (B) show agenesis of the corpus callosum with colpocephaly.
Twenty-five-weeks’ and Over Group
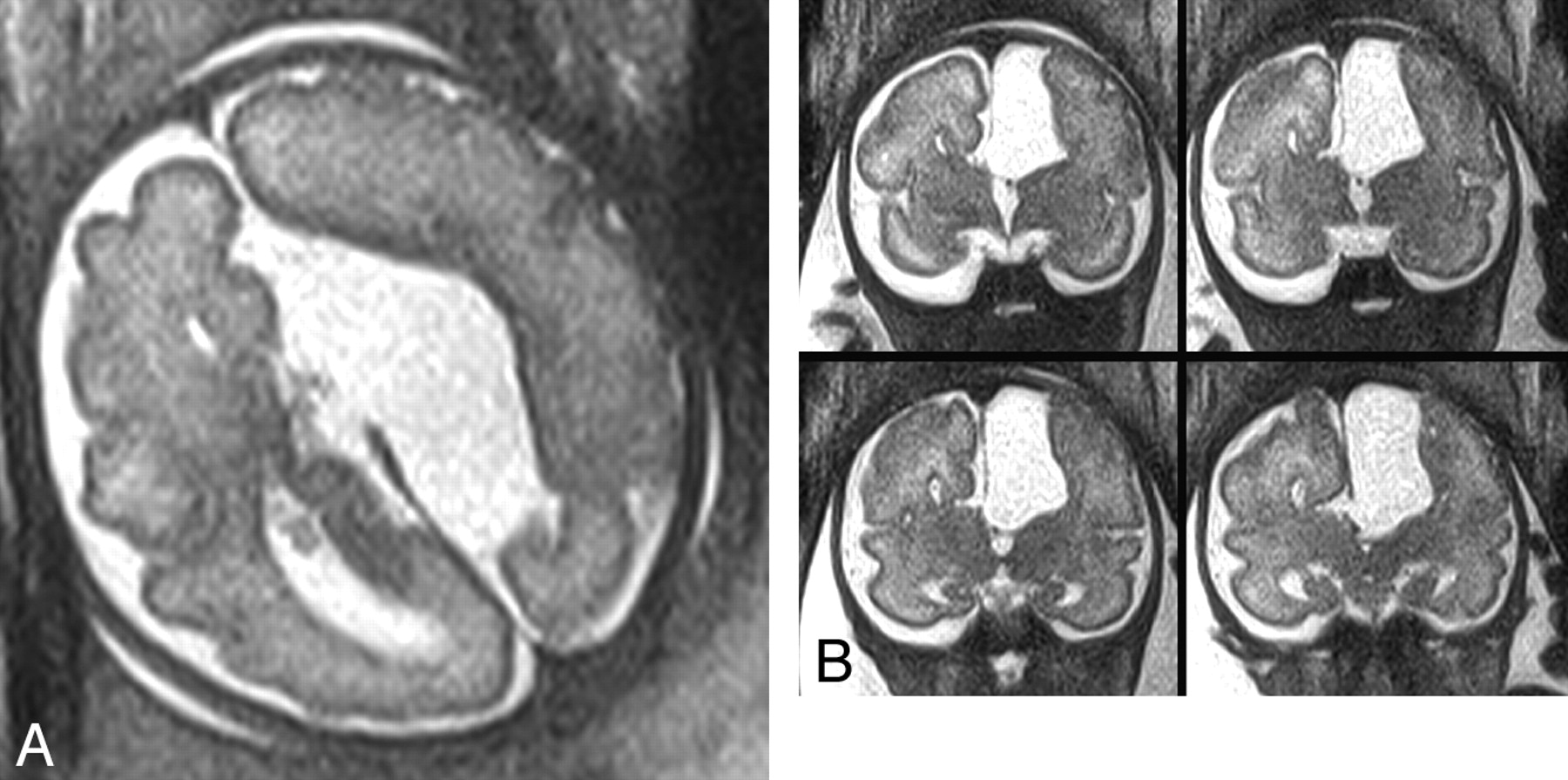
The median gestational age range at the time of iuMR for this group was 25–27 weeks. Forty-eight fetuses were referred with isolated VM on sonography at 25 weeks’ gestational age or later, most between 30 and 34 weeks. Sixteen of 48 (33%; 95% CI, 20%–48%) fetuses had additional brain pathology. The categoric assessment of the largest trigone in the 32 cases of confirmed isolated VM according to iuMR was the following: mild, 17/32; moderate, 10/32; and severe, 5/32. The details of the 16 cases with other brain abnormalities shown on iuMR are presented in on-line Table 2 and consisted of 11 developmental abnormalities and 5 acquired pathologies. As in the 20–24 weeks’ group, failed commissuration was the most frequently associated developmental abnormality of the 25+ weeks’ group (6/16, 3 associated with a neocortical abnormality). Examples are shown in Figs 2 and 3. The categories of enlarged trigones (on the most severely affected side) in the fetuses with other brain abnormalities are shown in on-line Table 2. Most fetuses had severe VM.

A fetus depicted on iuMR at 30 weeks’ gestational age because of VM. A and B, Axial (A) and a montage of 4 consecutive coronal single-shot fast spin-echo images (B) show agenesis of the corpus callosum with colpocephaly.

iuMR images of a fetus at 31 weeks’ gestational age thought to have isolated VM on sonography. Axial (A) and a montage of 4 consecutive coronal single-shot fast spin-echo images (B) show agenesis of the corpus callosum and an associated interhemispheric cyst. The cortex adjacent to the cyst was interpreted as abnormal, but no formal confirmation of that finding is now available.
Table 1 shows that there is a 6% risk for fetuses with mild VM to have a further brain abnormality in both gestational age groups. The overall increase in relative risk in fetuses with severe VM was 10.3 when compared with fetuses with mild VM, and this elevated risk did reach statistical significance.
Risk of detecting brain abnormalities on iuMR relative to the degree of VM of the fetusa
There was excellent independent agreement between the 2 reviewers who performed the analysis on the effect on management in cases of other brain pathology being shown. There was complete agreement in 20/25 (80%; 95% CI, 59%–93%) cases, 1 grade of disagreement in 3, and 2 grades of disagreement in 2 (on-line Tables 1 and 2). In 4/9 cases with abnormal findings in the 20–24 weeks’ group, the effect of iuMR on management was judged as “iuMR gave additional information that significantly altered prognosis to a degree that termination of pregnancy was offered” as judged by both reviewers. Those circumstances occurred in 2/16 cases in the 25+ weeks’ group.
Discussion
Fetal VM can arise from a number of causes, including obstruction to CSF flow (leading to hydrocephalus), focal or generalized loss of brain volume (ex-vacuo dilation), and secondary to malformation of the CNS (dysmorphic). In many cases, however, no cause is found either before or after delivery. The 2 clinical considerations in a fetus with VM are the degree of ventricular enlargement and the presence or absence of other abnormalities, of which CNS abnormalities are common. It is widely accepted that severe categories of VM are associated with higher risks of poor clinical outcome,12 and indeed recent studies have questioned whether mild VM (trigone measurements of 10–12 mm) is truly abnormal if it is an isolated finding.13,14 For example, in a study of 176 cases, Gaglioti et al7 showed that a fetus with isolated VM had a 97.7% chance of being alive at 2 years if the VM was mild, an 80% chance with moderate VM, and a 33.3% chance with severe VM. Of those that were alive, neurodevelopmental outcome was normal in 93% of mild cases, 75% of moderate, and 62.5% of severe VM cases.
An earlier study by Gupta et al15 described 276 cases of apparent isolated VM, all of whom were delivered. They found a 70% survival rate, and 59% of the survivors were developmentally normal. Most centers referring cases into our study quote figures of <5% chance of adverse neurologic outcome in cases of mild VM if there are no other CNS abnormalities. This view has been supported in the recent paper of Falip et al,10 who incorporated iuMR study results into their antenatal definition of isolated VM. They showed that the outcome of isolated VM was excellent in fetuses with 10- to 11.9-mm trigones in 94% of cases and in 85% of cases with trigone measurements of 12–15 mm.
There have been improvements in sonographic image quality which, together with an increased understanding of the importance of failed commissuration (eg, agenesis of the corpus callosum) in prognosis, have contributed to improved detection of isolated VM. The presence of other CNS abnormalities is important because it is the brain abnormality that is responsible for the postnatal morbidity and mortality in most cases rather than VM per se.16 It is of major importance, therefore, to have sought other pathology with the best imaging method available.
The introduction of iuMR into clinical practice has provided a supplementary method of assessing the fetal brain. There could be no a priori reason to believe that iuMR would be more accurate than sonography in assessing the size of fetal ventricles. Early work by Garel and Alberti17 seemed to support that assumption, but a more recent publication, including the same author, showed the opposite conclusion.18 The retrospective analysis of Salomon et al18 included 185 third-trimester fetuses who had isolated mild VM (ie, 10- to 12-mm trigones) as measured on sonography. They found that the most frequent disagreement between sonography and iuMR was in the classification of the degree of VM. Forty-three fetuses (23.3%) had ventricles <10 mm on iuMR (ie, normal size), and 36 fetuses (19.4%) had trigone measurements of >12 mm on iuMR. All of those findings would have had significant effects on the information given to the parents.
The work described in our article supports the authors’ original findings—that is, there is little disagreement between the dimensions of the trigones measured on sonography when compared with iuMR. In the 122 cases of isolated VM confirmed by iuMR in this study, there was complete categoric agreement about the degree of VM in approximately 90%. In all but 1 case of categoric disagreement, there was a difference in absolute measurements of no greater than 2 mm, which is in broad agreement with the work of Salomon et al.18 We found only 2 cases diagnosed on sonography as mild VM with trigone measurements of <10 mm on iuMR.
On the basis of those findings, we conclude that iuMR does not have a role in assessing the size of the ventricular trigones over and above sonography, but with 2 caveats. There are sometimes problems in visualizing the entire ventricular system on sonography because of factors such as fetal position and problems caused by calvarial ossification.19 There is also a specific problem in visualizing the lateral ventricle closest to the sonography probe (near-field effect), which may be of relevance in cases of asymmetric VM. We have not addressed the near-field effect in the current work, but our earlier work suggested that fetal ventricular morphology is an important indicator of brain malformation.20
There is growing evidence that iuMR has a higher detection rate of fetal brain abnormalities when compared with sonography.21–23 Our earlier study of 100 fetuses showed an overall improvement in diagnostic accuracy of 48% for unselected cases of fetal CNS abnormalities.24 Fetuses with VM as part of their referral information accounted for approximately half of those cases, and an improvement in the detection rate of close to 50% was found in that subgroup. With particular reference to fetal VM, Launay et al25 concluded that iuMR was “more informative than sonography in 32.8% of cases” and showed the cause of the VM in 21.3% of cases in a study of 61 fetuses. As described earlier, Salomon et al18 studied 185 third-trimester fetuses with isolated mild VM. With the exception of 43% of cases in which there was a disagreement about the category of VM, 11/185 (5.9%) had other brain abnormalities. Our earlier work, based on a study of the first 30 fetuses with isolated VM referred between 1999 and 2003, showed that iuMR depicted additional abnormalities in 50%.26
Selection bias is a major problem in interpreting such studies, particularly retrospective reviews of clinical referrals, and our present prospective evaluation of fetuses with isolated VM provided an opportunity to control the referral bias as much as possible. In particular, we started with the assumption that the strict criteria for inclusion into the study would be likely to provide the minimum improvement in diagnostic accuracy of any group with fetal CNS abnormalities shown on sonography. If that is true, the overall improvement in detection of 17% must be considered as highly relevant. All of the obstetricians and radiologists from our referring centers were free to enroll all of their cases of isolated VM. However, we did not study how many women were not asked to join the study, nor do we know how many were asked and refused. We must accept, therefore, that we have not eliminated referral bias, and we do not know the depth of the problem. For example, it is possible that the fetomaternal experts were more likely to refer fetuses with severe VM because they had believed that iuMR was more likely to find a further brain abnormality.
Before we discuss our results, it is important to highlight a weakness of the study as it stands. Ideally a study such as this should have a reference standard diagnosis made by follow-up postnatal imaging or autopsy studies, but this has not been performed as yet. Our earlier studies have provided that level of detail, and iuMR was always as good as the reference standard,11 but we do not have those data for the cases in this study at present. In defense of that, many of the diagnoses made in this study could be considered “true by definition” (eg, agenesis of the corpus callosum, intracranial hemorrhage) as is the case in pediatric neuroimaging. We have to accept, however, that the diagnoses of “abnormalities of cortical formation,” for example, cannot be taken as read at present. It is our intention to perform clinical and radiologic studies later in life on the children born in this study. Due comment must also be made about the problems of obtaining postmortem information for studies performed in the United Kingdom because of the very low autopsy rate as discussed previously by Griffiths et al.27
Our results show that there is a clear relationship between the degree of VM and the risk of other brain abnormalities. In the entire group of fetuses studied, severe VM was approximately 10 times more likely to be found in association with a brain abnormality than mild VM. iuMR was more likely to find a brain malformation in the 25+ weeks’ group when compared with the 20–24 weeks’ group, though this is probably explained by the higher frequency of severe VM cases in the later gestational age group. The small number of fetuses recruited into the severe VM group makes interpretation problematic, but as the data stand, the relative risk of a brain abnormality with severe VM in the 25+ weeks’ group was much higher (13.3) than in the 20–24 weeks’ group (4.0).
There was, however, a 6% chance of showing a brain abnormality in cases of mild VM at any gestational age older than 20 weeks. A wide range of brain pathology was shown by iuMR, both developmental and acquired. One malformation that was featured most frequently was failed commissuration (agenesis of the corpus callosum), which accounted for 11/25 (44%) cases either alone or in conjunction with further brain abnormalities. This suggests that failed commissuration can be a difficult diagnosis on sonography. Why that structure presents such difficulties is a subject of debate and warrants further investigation. In many cases, it is difficult or impossible to visualize the corpus callosum directly in the fetus with sonography, and the cavum septum pellucidum is often used as a surrogate indicator that the corpus callosum is present. It has also been raised recently whether there is a potential for misidentification of the septal leaves because of abnormally placed fornices.28–30 The role of advanced sonographic methods such as 3D/4D sonography with its ability to create reconstructed sonographic images in the midline is also under evaluation.
The detection of CNS abnormalities by iuMR has been shown to have a high impact on clinical management in other studies, but not specifically in isolated VM cases. Simon et al22 showed that 46% of 52 cases were managed differently after iuMR, and a similar analysis made by Levine et al31 showed an overall 13.5% rate of management change and a counseling change in 49.7%. Those authors have suggested that in fetuses with VM “MR can be helpful in visualizing associated abnormalities…,” but they did not say which cases should be selected for iuMR.9 Significant effects on clinical management in our study occurred most frequently in the 20–24 weeks’ group of pregnancies; the assessors judged that termination of pregnancy would have been considered in 4/9 cases. Similar changes in patient management were less likely in the 25+ weeks’ group, occurring in only 2/16. The most likely explanation for this is the severity of VM associated with the brain malformation. The negative effect on outcome for the more severe forms of VM has been redemonstrated by Ouahba et al32 recently in a study that included iuMR investigations to confirm or refute isolated VM. Severe VM was much more common in the 25+ weeks’ group, and the assessors judged that women with fetuses with severe VM would have been advised of high risks of poor outcomes and perhaps offered termination of pregnancy irrespective of the information about brain malformation provided by iuMR.
This point is well illustrated in our 20–24 weeks’ group, in which 3/5 of the cases of failed commissuration were associated with mild or moderate VM, and termination of pregnancy would have been considered as a result of the iuMR. In contrast, in the 2 cases in the 20–24 weeks’ group with failed commissuration and severe VM, the effect on management brought about by the detection of the additional brain malformation was minor.
Conclusions
Our work demonstrates that there is a good case for including iuMR as part of the diagnostic process for fetuses thought to have isolated VM on sonography at any time after 20 weeks’ gestational age, with additional brain abnormalities shown in 17%. It could be argued that any resource to provide iuMR on a national basis is best directed at the 20–24 weeks’ group. Although the improvement in detection rate was only 6% in that group, there was a higher impact on clinical management as judged by the independent assessors. It should be noted, however, that some significant changes in clinical management were brought about by the inclusion of iuMR in the older gestational age fetuses.
Footnotes
-
We are grateful for the support of the Wellcome Trust, UK. We would also like to acknowledge Westfield Health for financial support for the salary of Mike Reeves, MD, as a Clinical Research Fellow. Elspeth Whitby, MD, was supported by The Health Foundation via the Academy of Medical Sciences. Westfield Health and The Health Foundation did not have any role in the design or conduction of this study, or in the preparation of this manuscript.
-
The study was approved by the South Sheffield Research Ethics Committee and sponsored by the Wellcome Trust, UK.
-
Indicates article with supplemental on-line tables.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received April 1, 2009.
- Accepted after revision June 3, 2009.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Role of Magnetic Resonance Imaging in Diagnosing Fetal Brain Pathologies
- MR Imaging Diagnosis of Diencephalic-Mesencephalic Junction Dysplasia in Fetuses with Developmental Ventriculomegaly
- Complex Fetal Care: Implications of Fetal Ventriculomegaly: A Neurosurgical Perspective
- MRI of the foetal brain using a rapid 3D steady-state sequence
- The use of in utero MRI to supplement ultrasound in the foetus at high risk of developmental brain or spine abnormality
- Asymmetric Development of the Hippocampal Region Is Common: A Fetal MR Imaging Study
- The Use of In Utero MR Imaging to Delineate Developmental Brain Abnormalities in Multifetal Pregnancies
- Fetuses with Ventriculomegaly Diagnosed in the Second Trimester of Pregnancy by In Utero MR Imaging: What Happens in the Third Trimester?