
Abstract
SUMMARY: Animal models are necessary to develop and test innovations in aneurysm therapy before clinical introduction. This review aims at identifying the most likely candidates for standardizing preclinical testing of aneurysm devices. We systematically searched electronic databases for publications on animal aneurysm models from 1961–2008 to assess the methodologic quality of the studies and collect data on the patency and angiographic and pathologic outcomes of treatments. There has been a steady increase in the annual number of publications with time. Species that were most frequently used were dogs, rabbits, and rodents, followed by swine. Most publications are single-laboratory studies with variables and poorly validated outcome measures, a small number of subjects, and limited standardization of techniques. The most appropriate models to test for recurrences after endovascular occlusion were the surgical bifurcation model in dogs, and the elastase-induced aneurysm model in rabbits. A standardized multicenter study is needed to improve the preclinical evaluation of endovascular devices in aneurysm therapy.
Abbreviations
- Angio
- angiography
- ICA
- intracranial aneurysms
- IHC
- immunohistochemistry
- SEM
- scanning electron microscope
- w
- width
Therapeutic innovations carry with them the promise of new treatments as well as the fear of new adverse events. Some form of preclinical screening test is necessary to minimize the risks for patients and to limit large-scale clinical investigations to the most promising devices. If initial development often involves in vitro experiments and bench testing, the last steps of device assessment before clinical introduction must take into account the complexity of the in vivo environment. Animal models are used for that purpose.
Naturally occurring intracranial aneurysms are rare in laboratory animals. Therefore, various models have been designed in many species, including mice, rats, rabbits, swine, sheep, dogs, and primates. Each model has advantages and limitations, and the choice will depend on the purpose. Experimental aneurysm models can be used for the following: 1) understanding the mechanisms involved in the initiation, progression, and rupture of aneurysms; 2) testing endovascular devices; and 3) training interventionists.
Using a variety of physiologic and pathologic manipulations, such as carotid ligation, renovascular hypertension, and lathyrism in rodents and primates, Hashimoto et al1 developed 1 model that closely resembled the morphologic, histologic, and hemodynamic features of human intracranial aneurysms. One advantage of this model is the induction of cerebral aneurysms without direct manipulation of intracranial arteries.2 These models could offer insight into the potential efficacy of pharmaceutical prevention of aneurysm formation and improved understanding of aneurysmal growth. However, the small size of aneurysms in mice and rats render these models inappropriate for the testing of endovascular interventions.
Murine models are useful for looking into the biology of arterial aneurysms, far beyond what can be achieved in large animals, thanks to the availability of sophisticated molecular and cellular techniques, including a wide array of genetically modified mice strains. An effort to retain these advantages in testing human devices has led some teams to construct aneurysms on the lateral wall of the abdominal aorta of rats or mice by using microsurgical techniques,3 and others to simplify models by eliminating the need for an aneurysm altogether and studying the direct implantation of coils into normal arteries4,5 or stents and flow diverters to determine branch preservation. Even though simpler designs such as arterial occlusion models can provide important insight regarding fundamental vascular phenomena, such as recanalization after coil embolization,5,6 they cannot comprehensively anticipate the potential advantages and complications related to the use of devices in human aneurysms. Hence, the development and refinement of new endovascular therapies have mostly relied on larger aneurysm models such as those in rabbits, swine, and canines,7–11 induced by vessel ligations combined with enzymatic injury or surgically constructed from autologous venous pouches. These larger models will be the focus of this review.
Inspired by the pioneering work of German and Black (1954),12 surgical constructions in rabbits, swine, and dogs varied in complexity, from lateral wall types by end-to-side suturing of a segment of vein to carotid arteries,13–15 to bifurcation aneurysms, anastomosing the right and left carotid arteries at the site of venous pouch implantation.8,16–19 (For a review, see Massoud et al 1994.20) The elastase-induced aneurysm model, most frequently used in rabbits,21,22 has been modified in various ways.23,24 Our aim was to review in the literature the main features of these models and their strengths and weaknesses in an effort to identify those that could serve as the most appropriate final assessor of new aneurysm devices immediately before clinical use. We paid special attention to models assessing coil embolization.
Materials and Methods
Search Strategy and Inclusion Criteria
We performed a computerized search strategy of Medline/PubMed (1961–2008) and EMBASE (1980–2008) for reports on animal models of aneurysms. We used the following keywords: aneurysm, saccular aneurysm, intracranial aneurysm, experimental aneurysm, animal models, swine, rabbit, dog, primate, mice, and rat in different combinations (by using the Boolean operator OR in conjunction with the Boolean operator AND). We performed a hand search in journals not indexed in PubMed and in bibliographies of included articles and review articles for additional studies. This method of cross-reference checking was continued until no further publications were found. We included studies that met all of the following criteria: 1) peer-reviewed articles, 2) original studies (not a letter, review article, conference abstract, or editorial), 3) English or French language, 4) a treatment (stents, coils, embolic agent) performed, 5) minimum number of 5 aneurysms, 6) minimal follow-up of 2 weeks, and 7) angiographic or pathologic outcomes.
The second author (O.N.) independently assessed the reproducibility of the search strategy and the eligibility of studies. In the case of disagreement, both observers (F.B. and O.N.) reviewed the article in question together until a consensus was reached.
Data were extracted to a data sheet, including the following: publication (first author's name, URL), aim of the study, species, the number of animals/aneurysms, aneurysm induction, outcomes, follow-up, compliance with animal welfare regulations, and embolization technique.
General Characteristics and Angiographic and Pathologic Outcomes
The absence of standardized end points precluded a meta-analysis. We collected general characteristics of the models (aneurysm size, neck morphology, patency of untreated aneurysms, angiographic occlusion rates, histologic techniques, and surgical complications) as claimed by the authors of the various source articles, and the results are given as a narrative report with references, without an attempt at quantification and cross-comparison.
Quality Assessment
The methodologic quality of the studies was scored against the following criteria (1 point each)25: 1) compliance with regulations, 2) inclusion of a control groups, 3) aneurysm size, 4) long-term patency, 5) rate of occlusion/recurrences, 6) correlation between angiography and histology, 7) blinding of outcome assessment; 8) randomization; and 9) procedural complications. Results expressed as means ± standard error of the mean were compared with analysis of variance, by using P < .05 as significant.
Results
Description of Studies
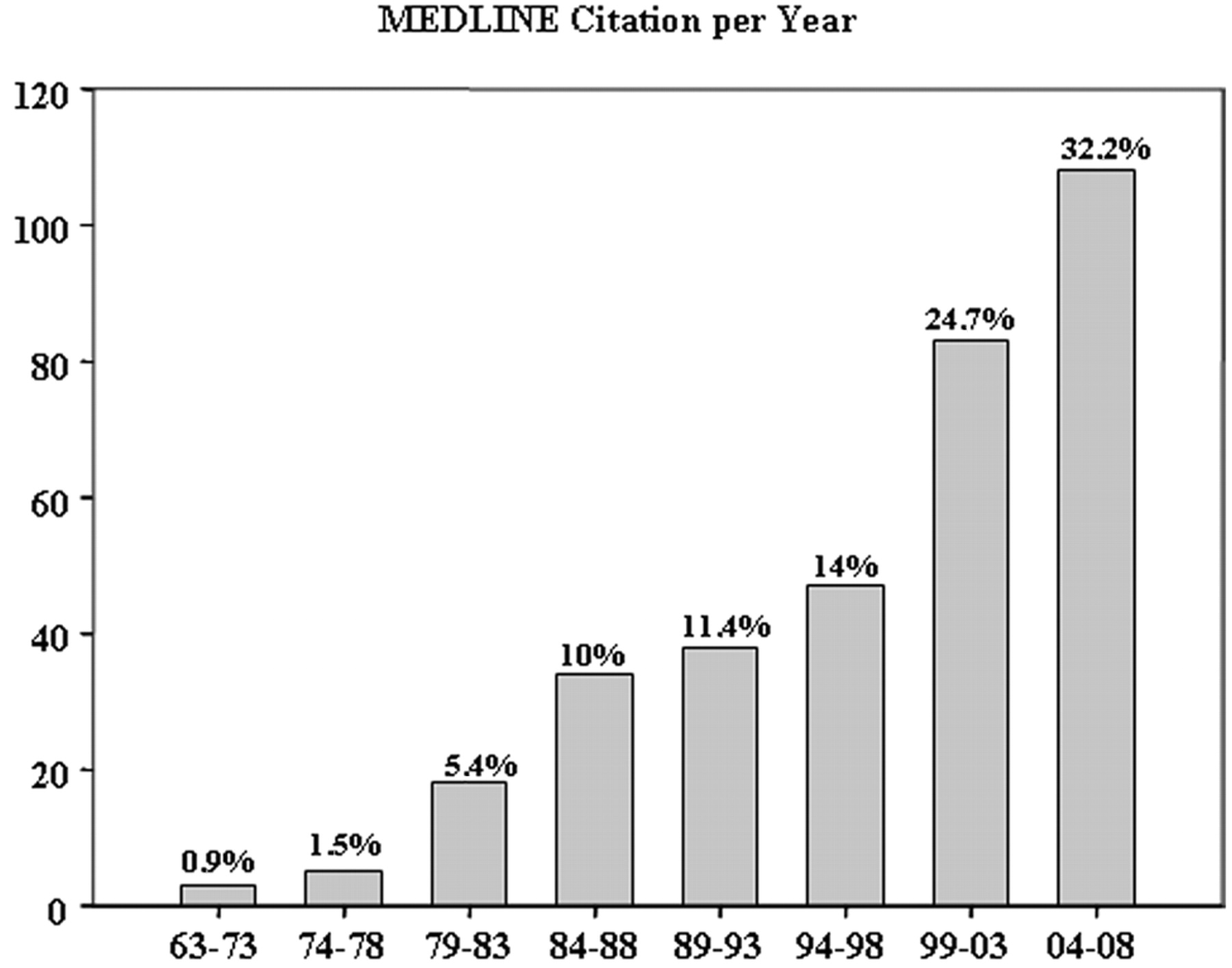
The initial search retrieved 571 publications (Fig 1). After viewing abstracts, we excluded 292 (51%); 57 articles were identified on hand searching of bibliographies and review articles, giving a total of 336 articles that were fully evaluated. We found an increasing number of articles per year published between 1961 and 2008 (Fig 2). Canine models were the most frequent (105 publications), followed by rabbits (90), rodents (83), swine (49), and primates (9).

Search strategy and selection process for identifying articles on aneurysm models.

Number of publications per year reporting intracranial aneurysm models, as recruited in electronic data bases, showing a threefold output in the 2000s compared with the decades from 1963 to 1993.
After examination of the full texts, we excluded 205 articles (61%) on the basis of selection criteria, yielding 131 studies. There were 55 reports on dogs, 31 on swine, 44 on rabbits, and 1 study on primates (Table 1). We identified 3 different models: lateral wall (82 studies; 2143 aneurysms, 57%); bifurcation (31 studies; 848 aneurysms, 22%); and elastase-induced aneurysms (27 studies; 794 aneurysms, 21%). In the 55 reports on dogs, 34 (62%) were on the lateral wall aneurysms, 12 (22%) were on bifurcation aneurysms, and 9 (16%) studies were about both. In the 44 studies on rabbits, 27 (61%) were on elastase-induced aneurysms, 7 (16%) on lateral wall aneurysms, and 10 (23%) on bifurcation aneurysms.
Number of each type of aneurysm per species in the final set of included studies (n = 131)
Quality of Studies
Methodologic domains that were most frequently respected are summarized in Table 2. Few studies used randomization or blind assessment of outcomes or attempted to correlate pathologic end points with angiographic outcomes. There was no difference in quality scores among the lateral wall (5.07 ± 0.19; n = 72), bifurcation (5.41 ± 0.22; n = 31), and elastase-induced aneurysm models (5.56 ± 0.27; n = 27) (P = .38).
Results of quality assessment of included studies
General Characteristics
The main characteristics of the 5 most frequent models are summarized in on-line Table 1.
Surgical constructions were most frequent: 2991 (57%) of 3785 aneurysms were surgically created, while 794 (21%) elastase-induced aneurysms were recorded. Canine models were most frequently used; many desirable features, including reliable anesthesia, large vessels, and excellent long-term survival, were reported.7,11,17,19,26
Claims in favor of swine models included similarities to human physiology and coagulation systems; these models are commonly used in the field of cardiovascular research.27
Surgical constructions have been used in all species, most frequently the lateral wall model (n = 2143, 57%). Bifurcation models included many variants.19,28,29 The ability to vary the anatomy of the bifurcation, aneurysm size, neck size, and fundus-to-neck ratio is a potential advantage of surgical models.20
Creation of bifurcation aneurysms in rabbits is more difficult and perhaps less reliable, with a higher incidence of anesthesia-related deaths, procedure-related mortality, and parent vessel occlusions.8,30,31
The elastase model was limited to rabbits, with advantages of easy in handling and long-term survival with aneurysms followed for >5 years.32 With some training, the results seem to be reproducible. Limitations included the uncontrolled size of aneurysms (potentially corrected by adjusting the ligation site),33 sacrifice of the arterial access for each angiogram, and the small size of the animal, limiting the evaluation of large devices or techniques requiring multiple catheters.34
Angiographic Outcomes
The lack of spontaneous thrombosis is an important criterion for a good model. Natural history studies of untreated aneurysms are few, however. In swine, the patency of untreated aneurysm was evaluated in only 7/31 studies (22%); swine aneurysms, when left untreated, have a tendency for postoperative rupture or spontaneous thrombosis. This drawback necessitated immediate embolization following aneurysm construction.9,35 We noted spontaneous thrombosis between 2 and 7 weeks of lateral wall swine aneurysms (n = 5).13,35 Aneurysm patency was reported in 5/12 canine bifurcation aneurysm studies, in 6/9 on bifurcation and lateral wall aneurysms, and in 21/34 on lateral wall aneurysms. Canine lateral wall aneurysms may infrequently undergo thrombosis (<10%), but most aneurysms (90%) remained patent during a follow-up period of ≥7 months.36–38 Bifurcation aneurysms enlarge during the first several weeks.38 The incidence of spontaneous thrombosis is influenced by the ratio of the volume of the aneurysm to the area of the neck (ostium).12 Modifications of the ostium can also minimize thrombosis.26,39
In rabbits, 1/7 studies assessed the patency of surgically created lateral wall aneurysms, and 8/10, of bifurcation aneurysms. In the elastase model, 20/27 studies confirmed aneurysm patency. A long-term study showed neither spontaneous thrombosis nor significant change in dimensions 24 months after aneurysm creation.40
The standard method for the evaluation of the treatment is angiography. The occlusion and recanalization rates found after embolization will, of course, depend on the device targeted by the publication.
Coil embolization of swine aneurysms is routinely followed by progressive and finally complete occlusion.35 Residual necks and recurrences after coil embolization have been demonstrated in lateral wall aneurysms in dogs; however, recurrences are rare when lateral wall aneurysms are completely occluded initially.28 Bifurcation aneurysm models in dogs and rabbits can show recurrences with variable frequencies, despite treatment with various types of devices.12,13,16,28,41–43 Angiographic recurrences are rarely documented after coil embolization of the rabbit elastase aneurysms, but “microrecurrences” (only seen at pathology) are common.10,44,45
Pathologic Analyses of Treated Aneurysms
The pathology of aneurysms treated by embolization or stent placement is hampered by the presence of metallic or polymeric materials. One option is to embed the specimen in resins with the device in situ and resort to cutting-grinding thick sections, a method that precludes standard processing methods and advanced techniques such as immunohistochemistry or immunofluorescence. An alternative is to carefully dissect the device from the tissues and use standard paraffin embedding. A variety of ways to circumvent these difficulties have been published,46–48 but high-quality analyses of early fragile specimens (within days after embolization), which could have been mechanistically revealing, often remain problematic. Studies reporting pathologic techniques are summarized in Table 3. In the 120 studies that included histologic findings, only 23 (19%) used a qualitative or semiquantitative grading system developed by the authors.
Number of studies reporting the different histologic techniques (tissue-processing procedure, conventional staining, IHC, SEM) and the use of scoring technique
A correlation between pathologic and angiographic outcomes has rarely been documented, except for canine bifurcation aneurysms.29,42,43 Among the 10 studies performed in bifurcation aneurysms in rabbits, 5 revealed a considerable discrepancy between radiologic and pathologic findings, with angiography overestimating the degree of occlusion in all cases.8,18,30,31 Microscopic recurrences have been described with the rabbit elastase model, but a correlation with angiographic recurrences is rarely possible.45,49,50
Nevertheless, characteristics of the healing of experimental aneurysms, mainly gleaned from cross-species comparisons, have been described. These studies have uniformly revealed organization of the thrombus within the aneurysmal sac within 6 months of platinum coil embolization of surgically created aneurysms in canines and swine, as well as neointimal coverage of the ostium of occluded aneurysms.7,51–53 The most frequent descriptions of coil embolization of aneurysms are summarized in Table 4.
Primary histopathologic findings after coil embolization of experimental aneurysms
Aneurysms in swine have a tendency to heal, with or without embolization and with any material.9,13,35,54,55 Early inflammatory changes39,54,55 were followed by a centripetal myofibroblast infiltration, robust collagen deposition, and a thick neointima, which completely sealed the neck.48 When all specimens showed permanent occlusions and favorable healing characteristics at some delayed time points, as seen in swine aneurysms, then some earlier timeframe was chosen, in hopes of detecting accelerated healing with some new material.56
In the long term, treated canine lateral wall aneurysms are completely occluded in most cases.7,41,51–53,57 Canine bifurcation aneurysms have a propensity for recurrences, however; therefore, they can reproduce the problem found in human aneurysms.41,54 Nevertheless, organization of thrombus was found at 4 weeks,57 whether aneurysms were occluded or showed early recurrences. At 3 months,28,29 recurrences were found, despite the presence of a neointimal layer that was continuous with the endothelialized clefts, which are thought to be involved in the recanalization process.
Rabbits seem to have a lesser propensity for healing. There was no endothelialization across the aneurysm orifice and no evidence of organized thrombus, but a thickened wall was associated with chronic31 or no major inflammatory reaction8 in bifurcation aneurysms.
Platinum coil embolization of rabbit elastase–induced aneurysms was followed by relatively poor healing, through thrombus formation, granulated tissue organization, and, finally, loose connective-tissue formation with no contractile cell infiltration. Deposition of collagen was absent, and tissue coverage at the neck was relatively poor.10,44,57
Discussion
The general ability of animal studies to predict future clinical success remains controversial. The debate has resurfaced recently with the repeated disappointments encountered in the development of drug therapies for stroke.58 It remains difficult to choose which promising device should be prioritized and which should be subjected to long and expensive clinical trials, without good quality preclinical studies. We have focused our study on models designed to assess endovascular devices, a modest objective compared with more fundamental research on the growth and rupture of aneurysms, for which most recent models would be deficient or inappropriate.
We believe that animal models remain grossly underused. Many endovascular devices in current clinical use have never been studied in published preclinical studies, and in the absence of randomized trials, many remain of unknown benefit. Animal studies have been more frequent in recent years, but there is no standardized testing required of an aneurysm device to be considered ready for a clinical application. Preclinical testing schemes typically include single-laboratory studies with various poorly validated outcomes and measures and small sample sizes. The main purpose of this review was to identify the best potential models that could serve such a standardizing role.
Some ideal features of a good aneurysm model include the following: minimal surgical and endovascular morbidity; similarity to human aneurysm shear stresses, hemodynamic forces, physical dimensions, perianeurysmal environment, and tissue responses; and stability without spontaneous thrombosis when untreated.59 None of the available models offer all these features.
Different animal models target different purposes. For example, swine models, widely used in cardiology circles, have been thoroughly validated to assess the risk of in-stent stenosis. The propensity of this species for thrombosis and neointima formation, particularly useful to assess arterial stenoses after device implantation,27 makes this model ill-fitted for discriminating the capacity of aneurysm-treatment devices to prevent recanalization or induce permanent occlusions. Reproducing the clinical problem that innovations are designed to address is a fundamental requirement of a model. Hence, lateral wall models in general, and swine models in particular, cannot predict the ability of new coils to improve long-term angiographic results.28,35
Two models have repeatedly proved valuable in the assessment of aneurysmal devices: the canine bifurcation model and the rabbit elastase model. These models have not been thoroughly evaluated for repeatability of results between centers however. Future collaborative work should concentrate on this issue.
Any meaningful research must involve comparison between 2 treatments by using some end point criteria. Angiographic outcomes at 3 or 6 months can be compared in the canine bifurcation aneurysm models, and with such end points, the value of 1 embolic device over another was shown in the past.19,43,60 We must remember that even if better angiographic results in animals could be shown to predict better angiographic results in humans, these end points are surrogates for long-term efficacy in the prevention of ruptures.
The investigation of histologic phenomena that follow embolization has often been purely descriptive, but the meaning of these observations and their clinical relevance remain obscure when findings are not correlated, if not causally related, to a comparison between aneurysms that recur and those that do not.61 In the absence of an explanatory correlation between angiographic evolutions and pathologic findings, researchers have relied on a priori principles inspired from analogies with other vascular research fields. For example, incorporation into the vessel wall and neointima formation on stents, grafts, and stent-grafts62 have played a dominant role in the concept of healing after device implantation. Another potential justification for using pathologic findings as surrogate end points is human autopsy findings. Data on humans are quite limited.63–67 However, enduring occlusions after platinum coiling have been associated with neointimal closure of the neck and organization of the clot within the aneurysmal sac,67 while incomplete occlusions and recanalized aneurysms have been associated with unorganized thrombus and poor cellularity at the implant/parent artery interface.68 Many investigators have published scales that offer a rational, if not a validated basis, for assessing the performance of an implant, by giving points for features considered favorable for healing, including neck coverage with neointima, thickness of neointimal layer, or clot organization at the dome.11,19,43–47,56,69 These semiquantitative scales have largely been confined to single-center experiences; they have not been reproduced or validated. No one, to our knowledge, has been able to show that these criteria predict better in vivo clinical performances, however. Finally, the absence of a proved link between the biologic responses of these models with those found in human aneurysms must be emphasized.
Conclusions
Currently, available animal models present multiple weaknesses, but preclinical testing of new devices remains a necessity. Candidate models most appropriate for this preclinical evaluation include the rabbit elastase and the canine bifurcation aneurysm models.
Footnotes
Indicates article with supplemental on-line table.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.
- 56.
- 57.
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.
- 71.
- 72.
- Received July 5, 2009.
- Accepted after revision July 27, 2009.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Rabbit aneurysm models mimic histologic wall types identified in human intracranial aneurysms
- Surgical technique for venous patch aneurysms with no neck in a rabbit model
- Combined endovascular coiling and intra-aneurysmal allogeneic mesenchymal stromal cell therapy for intracranial aneurysms in a rabbit model: a proof-of-concept study
- Testing Stenting and Flow Diversion Using a Surgical Elastase-Induced Complex Fusiform Aneurysm Model
- Retrieval of Migrated Coils with Stent Retrievers: An Animal Study
- Safety and performance of the Penumbra Liberty stent system in a rabbit aneurysm model
- Angiotensin (1-7) as a Therapy to Prevent Rupture of Intracranial Aneurysms?
- Counterpoint--Response to "In Memoriam: The Matrix Coil"
- Stent-Assisted Coiling of Bifurcation Aneurysms May Improve Endovascular Treatment: A Critical Evaluation in an Experimental Model
- Thrombosis Heralding Aneurysmal Rupture: An Exploration of Potential Mechanisms in a Novel Giant Swine Aneurysm Model
- A Large and Giant Bifurcation Aneurysm Model in Canines: Proof of Feasibility
- Quantitative Angiographic and Histopathologic Evaluation of Experimental Aneurysms
- Improved Microsurgical Creation of Venous Pouch Arterial Bifurcation Aneurysms in Rabbits
- A New Canine Carotid Artery Bifurcation Aneurysm Model for the Evaluation of Neurovascular Devices