
Abstract
BACKGROUND AND PURPOSE: Aneurysm treatment by intrasaccular packing has been associated with a relatively high rate of recurrence. The use of mesh tubes has recently gained traction as an alternative therapy. This article summarizes the midterm results of using an endoluminal sleeve, the PED, in the treatment of aneurysms.
MATERIALS AND METHODS: A total of 19 wide-neck aneurysms were treated in 18 patients: 10 by implantation of PEDs alone and 9 by a combination of PED and coils. Angiographic and clinical results were recorded immediately and at 6 months following treatment.
RESULTS: Immediate angiographic occlusion was achieved in 4 and flow reduction, in another 15 aneurysms. Angiography at 6 months demonstrated complete occlusion in 17 and partial filling in 1 of 18 patients. There was no difference between coil-packed and unpacked aneurysms. Of 28 side branches covered by ≥1 device, the ophthalmic artery was absent immediately in 1 and at 6 months in another 2 cases. One patient experienced abrupt in-stent thrombosis resulting in a transient neurologic deficit, and 1 patient died due to rupture of a coexisting aneurysm. All giant aneurysms treated with PED alone were demonstrated by follow-up cross-sectional imaging to have involuted by 6 months.
CONCLUSIONS: Treatment of large, wide-neck, or otherwise untreatable aneurysms with functional reconstruction of the parent artery may be achieved with relative safety using dedicated flow-modifying devices with or without adjunctive use of intrasaccular coil packing.
Abbreviations
- AICA
- anterior inferior cerebellar artery
- BA
- basilar artery
- Immed
- Immediate
- DSA
- digital subtraction angiography
- ICA
- internal carotid artery
- ID
- internal diameter
- MRA
- MR angiography
- N/A
- not applicable
- PcomA
- posterior communicating artery
- PED
- Pipeline Embolization Device
- PITA
- Pipeline Embolization Device for Intracranial Treatment of Aneurysms
- Recan
- recanalization
- SAH
- subarachnoid hemorrhage
- SCA
- superior cerebellar artery
- Sup
- superior
The application of mesh tube implants for the treatment of intracranial aneurysms was first proposed in the early 1990s.1–3 Early experimental work suggested 3 potential mechanisms of action: improved anatomic reconstruction of the parent artery, functional modification of flow across the orifice of the aneurysm, and biologic repair of the aneurysm neck by neointimal overgrowth.1 Flow conditions within the parent artery and the aneurysm itself have long been thought to play an important role in aneurysm growth and rupture.4–11 Yet, the early application of stent-assisted aneurysm therapy was primarily focused on geometric reconstruction of the parent artery through improved coil packing of the aneurysm. A few clinical case reports, however, suggested that improved outcomes associated with the use of stents may be attributable to stent-induced modification of flow within and around the aneurysm,12,13 providing the impetus for development of higher coverage endoluminal sleeves for the treatment of cerebral aneurysms.14 The purpose of this study was to analyze the early clinical experience with the first dedicated flow-modifying device, the PED (Chestnut Medical, Menlo Park, California).
Materials and Methods
Indications
Between February 2007 and July 2008, a total of 19 aneurysms in 18 patients were treated at the National Institute of Neurosurgery, Budapest. Nine patients were treated in a multicenter international safety trial (the PITA study) enrolling a total of 31 patients. Eight patients were treated in a single-center trial (the PITA II Budapest study), enrolling 8 patients total. These later patients were not included in the PITA trial. Both studies were conducted under an ethics committee−approved protocol. One additional patient was treated following European conformity mark approval of the device.
Two aneurysms were treated as incidental findings; 10 because of headaches; 6 due to mass effect; and 1 due to recanalization following previous endovascular treatment. Regarding aneurysm morphology, sidewall and fusiform aneurysms were treated; we considered these to have a high likelihood of failure and/or recurrence with conventional endovascular techniques either because of a large or giant aneurysm or an unfavorable neck-to-sack ratio.
Periprocedural Angiographic Evaluation of the Aneurysms
Morphologic characteristics of the aneurysms and parent arteries, such as diameter and volume, were measured on 3D reconstructed images derived from rotational angiography before the procedure. All measurements were performed on an Advantage Windows Workstation by using ADW 4.2 software (GE Healthcare, Milwaukee, Wisconsin). Flow modification after PED implantation was classified as either complete stasis (if no contrast material entered the aneurysm following deployment of PED), significant flow reduction (if contrast stagnation was seen within the aneurysm at the late venous phase of the angiographic series), or slow flow (if the contrast circulation within the aneurysm became slower but without contrast stagnation into late venous phase images). Aneurysm occlusion was rated as either complete (if no contrast material entered the aneurysm by completion of the procedure) or incomplete (if any contrast filling of the aneurysm was seen on the last angiogram).
Operative Techniques
The Device.
The PED is a woven wire mesh tube made of 25% platinum and 75% cobalt-nickel alloy. It is designed to provide 30%–35% metal coverage of the inner surface of the target vessel with a pore size of 0.02–0.05 mm2 at a nominal diameter. The PED is attached to a pusher wire, compatible with a 3F (0.027-inch ID) microcatheter. The pusher wire has a platinum coil tip, which extends 15 mm beyond the distal edge of the PED. The device is delivered via a 0.027-inch ID microcatheter, requiring a 6F guide catheter support. Once positioned across the aneurysmal segment, the delivery wire is held while the distal one-third to one-half of the PED is carefully unsheathed. Once the unsheathed segment begins to expand, its distal end is released from the delivery wire by clockwise rotation of the wire. The proximal segment of the PED is then deployed by gentle advancement of the wire. Once the PED is fully deployed, it may be recrossed by advancing the microcatheter over the indwelling delivery wire, which can then be exchanged for a second PED. This provides a safe possibility of deploying multiple PEDs through the same microcatheter if necessary. At any point up to final deployment, the PED may be captured and removed from the body.
Procedural Protocol.
In each case, a 3F neurovascular microcatheter (Renegade High Flow, Boston Scientific, Natick, Massachusetts; or Mass Transit, Cordis [Johnson and Johnson], Miami Lakes, Florida) was placed across the neck of the aneurysm either directly or over an exchange wire that was previously advanced into a distal branch with the help of a smaller microcatheter. The number of PEDs to be deployed was decided on the basis of flow reduction, but multiple coverage of clinically significant side branches (such as the anterior choroidal artery or the SCA and the AICA in the basilar territory) was carefully avoided. Clinically forgiving branches, such as the ophthalmic artery, were liberally covered by as many PEDs as thought necessary to achieve satisfactory flow reduction. Earlier in the series, several aneurysms were treated by PED-supported coil packing of the aneurysm. For those, a dual-marker microcatheter (Excelsior SL 10, Boston Scientific) was placed within the aneurysm before PED implantation to secure the possibility of additional coil placement into the sac in case flow modification was considered unsatisfactory. With growing experience, we abandoned secondary coiling except in cases in which early aneurysm occlusion of an intradural aneurysm was desirable.
Periprocedural Medication.
Each patient was given 75 mg of clopidogrel and 100 mg of aspirin per day for at least 48 hours before and 6 weeks following the procedure. Aspirin, 100 mg/day, is still continued. Patients were anticoagulated by an intravenous bolus of sodium-heparin to achieve a double the normal activated clotting time value. Heparin anticoagulation was discontinued by the end of procedure.
Follow-Up
Patients were clinically followed at 30 days, 6 months, and 1.5–2 years after the procedure. Angiographic follow-up was performed routinely at 6 months. Clinical follow-up examinations were performed by the authors during office visits. Ophthalmologic symptoms were evaluated by an independent ophthalmologist. Angiographic results were evaluated by using both hard copy films and DICOM files by an independent core lab for patients treated in the clinical studies and by the authors for the first patient treated outside the studies (patient 18, On-line Table and Tables 1 and 2). Cross-sectional imaging follow-up by either CT or MR imaging was performed at 6 months for aneurysms presenting with mass effect. Eleven patients (12 aneurysms) had late imaging follow-up by MRA between 1.5 and 2 years postembolization.
Immediate and 6 months angiographic results of 19 aneurysms treated with PED
Complications and clinical outcome of 19 aneurysms treated in 18 patients with PED
Results
Aneurysm Location and Morphologic Data
Eighteen aneurysms were located on the intracranial ICA and 1, on the basilar trunk (BA). Four aneurysms were giant (≥ 25 mm), 10 were large (10–25 mm), and 5 were small (<10 mm) according to the Yasargil classification with a mean largest diameter of 16 mm. The mean aneurysm volume was 1.26 cm3, ranging from 0.047 to 3.969 cm3. All aneurysms had wide necks, ranging from 4 to 18 mm, with a mean neck size of 7.4 mm (On-line Table and Tables 1 and 2).
Procedural Techniques
Ten aneurysms were treated by PED-supported coil packing, and another 9 aneurysms were treated by PED implantation alone. The mean maximum aneurysm diameter was the same in both groups (16 mm), but the volume was larger in the unpacked group (1.63 versus 0.93 cm3). The mean volumetric packing attenuation of coiled aneurysms was 13.4%. These aneurysms were covered by either 1 (5 cases), 2 (4 cases), or 3 (1 case) PEDs. For unpacked aneurysms, a single PED was used in 2 cases; 2 overlapping devices, in 3 aneurysms; 3, in another 2; and 4 and 5 PEDs, in 1 case each. Aneurysms covered by 1 or 2 PEDs had a mean maximum diameter of 13 mm, a neck size of 6 mm, and a volume of 0.88 cm3, while those that received ≥3 PEDs had a mean largest diameter of 23 mm, a mean neck length of 11 mm, and a mean volume of 2.26 cm3 (On-line Table and Tables 1 and 2).
Angiographic Results
Flow Modification and Aneurysm Occlusion.
After placement of the PED construct, angiographic evaluation demonstrated complete stasis in 3 aneurysms, significant flow reduction in 13 (Fig 1A−C), and slow flow in 3. Complete aneurysm occlusion was found in 3 cases of PED-supported coil packing and in 1 case following flow modification alone.

Giant cavernous carotid aneurysm, with the patient presenting with third and sixth nerve palsy due to mass effect (patient 16, On-line Table and Tables 1 and 2), treated with flow modification. A, DSA, right ICA injection, oblique posteroanterior view before treatment demonstrates a giant partially thrombosed aneurysm (arrow). B, DSA, right ICA injection, oblique posteroanterior view, immediately following implantation of 3 coaxial PEDs across the neck of the aneurysm, demonstrates significantly reduced flow (arrow). C, Fluoroscopic image demonstrates the implanted PEDs (arrow) and delayed contrast stasis (broken arrow) within the aneurysm. D, Six-month follow-up angiogram demonstrates complete occlusion of the aneurysm and reconstruction of the parent artery. E, T2-weighted axial MR image of the same patient before treatment demonstrates the giant ICA aneurysm (arrow) with associated significant mass effect. F, Follow-up MR image at 12 months demonstrates collapse of the aneurysm and resolution of the mass effect.
Periprocedural Complications
Thirty-nine of 41 PEDs were successfully deployed in the desired position. Two PEDs were introduced into the microcatheter; however, they could not be deployed due to friction in a highly tortuous ICA. In addition, a gentle balloon dilation (Hyperform Balloon; ev3, Irvine, California) was needed to fully open the distal section of 1 device. Clinical complications occurred in 4 cases. One patient had a mild postprocedural hemiparesis lasting for 2 days. The patient fully recovered, and no ischemic changes were seen on CT. This event was primarily considered the result of contrast overload due to difficulties of catheter navigation and a lengthy procedure, but a CT-negative thromboembolic complication could not be excluded. One patient had an embolic occlusion of a retinal artery branch, resulting in a small visual field deficit following PED-supported coil packing of her complex paraophthalmic aneurysm. One patient who we subsequently learned had not taken her antiplatelet medication experienced acute intraprocedural in-stent thrombosis within the ICA. It was initially recanalized with tirofiban (Aggrastat) but re-occluded 2 days later, despite being treated with double antiplatelets. The patient had a transient hemiparesis. Having good collateral circulation, she fully recovered and the ICA later recanalized (Fig 2).
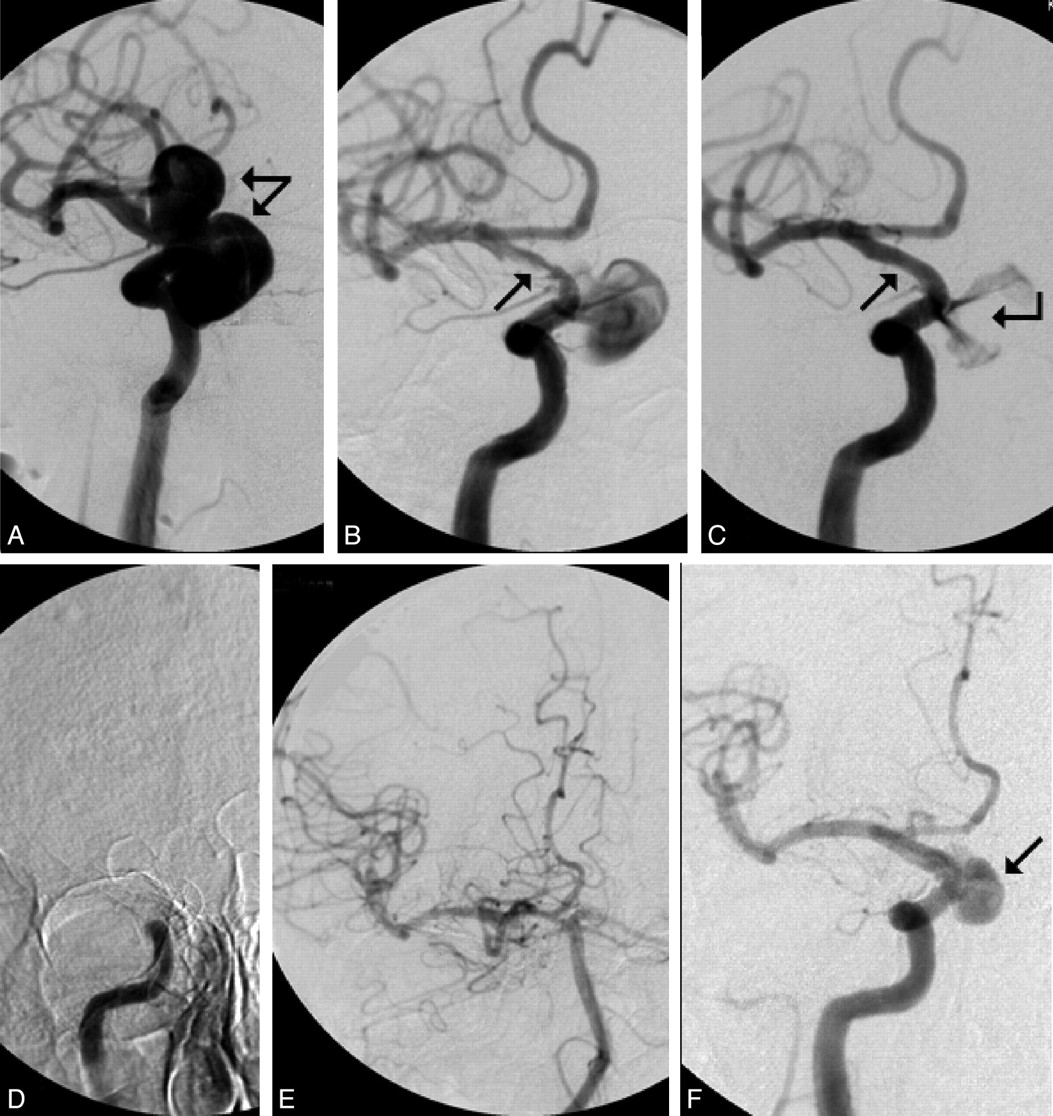
Giant infrasupraclinoid aneurysm of the right ICA. The patient presented with loss of vision due to mass effect (patient 13, On-line Table and Tables 1 and 2) and was treated with flow modification with transient thrombosis of the parent artery. A, DSA, right ICA injection, demonstrates bilobulated giant aneurysm (arrows). B, DSA, same view, following implantation of 2 coaxial PEDs, demonstrates partial in-stent thrombosis (arrow). C, DSA, same view, following tirofiban thrombolysis, demonstrates recanalization of the ICA (arrow) and significantly reduced flow within the aneurysm (broken arrow). D, Complete thrombosis of the ICA 2 days later. E, DSA, right vertebral artery injection, demonstrates good collateral circulation toward the right carotid system. No further action was taken at this time. F, Six-month follow-up angiogram demonstrates residual filling of the inferior portion of the aneurysm only (arrow).
One patient died secondary to a diffuse SAH within 5 hours following treatment. Repeat angiography failed to demonstrate the source of bleeding; however, autopsy suggested rupture of a small coexisting ICA bifurcation aneurysm distal to the target lesion. Given the patient’s tortuous anatomy and difficult catheter navigation, this could have resulted from a guidewire perforation during either the exchange manipulation or PED deployment. Small angiographically occult leakage might have led to a significant collection of blood within the subarachnoid space until it became symptomatic. Altogether, permanent nonrestricting morbidity occurred in 1, and mortality, in another patient.
Normal Branches Arising from the Parent Artery in Which the PED Would Be Deployed
A total of 28 visible side branches were covered, having an estimated diameter of 0.5–1 mm, including the ophthalmic artery in 17, the PcomA in 5, the anterior choroidal artery in 4, and the AICA and the posterior inferior cerebellar artery in 1 patient each. The ophthalmic artery was covered by 2 PEDs in 6, and by 3 and 4 in 1 case each. The PcomA was covered by 2 devices in 1 patient. The remaining branches had single coverage only. One ophthalmic artery was immediately nonvisualized on posttreatment angiography and resulted in a retinal branch occlusion. Two ophthalmic arteries, each covered by 3 or 4 devices, were found occluded at the 6-month follow-up. These delayed occlusions were clinically silent. No additional side branch occlusions were detected, including branches of the basilar trunk (Fig 3).

Giant dissecting aneurysm of the basilar trunk in a 16-year-old boy presenting with mass effect and sudden onset of hemiparesis (On-line Table and Tables 1 and 2, patient 18.). A, T1-weighted sagittal MR image demonstrates a basilar trunk aneurysm with mass effect (arrow). B, DSA, left vertebral artery injection, posteroanterior view, demonstrates the aneurysm (arrow). Small arrows demonstrate the origin of both duplicated SCAs; broken arrow demonstrates the origin of the left AICA. C, Fluoroscopic image following the procedure. Large arrows demonstrate the distal (white) and proximal (black) edges of the 5 coaxial PEDs that were used to reconstruct the lumen of the BA. Small arrows demonstrate the SCAs, and the broken arrow demonstrates the AICA, which are both covered by the flow-modifying devices. D, Six-month follow-up angiogram demonstrates complete occlusion of the aneurysm and reconstruction of the BA. Small arrows represent the duplicated SCAs, and the broken arrow demonstrates the left AICA. All of them are patent. E, T1-weighted MR image 7 months after treatment demonstrates collapse of the aneurysm and resolution of the mass effect. Signal intensity void due to metal artifacts is seen in the treated section of the BA.
Imaging Follow-Up
Eighteen of the 19 aneurysms were studied by conventional angiography at 6 months following treatment (1 patient died). All but 1 aneurysm was completely occluded, without evidence of neck remnant, and exhibited smooth remodeling of the parent artery (Fig 1A−D). In the patient with in-stent occlusion of the ICA, delayed recanalization of the parent artery was associated with partial residual filling of a bilobed giant aneurysm (Fig 2). Additional coil packing did not seem to make a difference in late aneurysm occlusion (9/9 loosely coiled and 8/9 uncoiled aneurysms thrombosed completely, despite the generally larger sizes of aneurysms in the uncoiled cohort; 1.6 cm3 versus 0.9 cm3 by volume) (On-line Table and Tables 1 and 2, Figs 4 and 5).

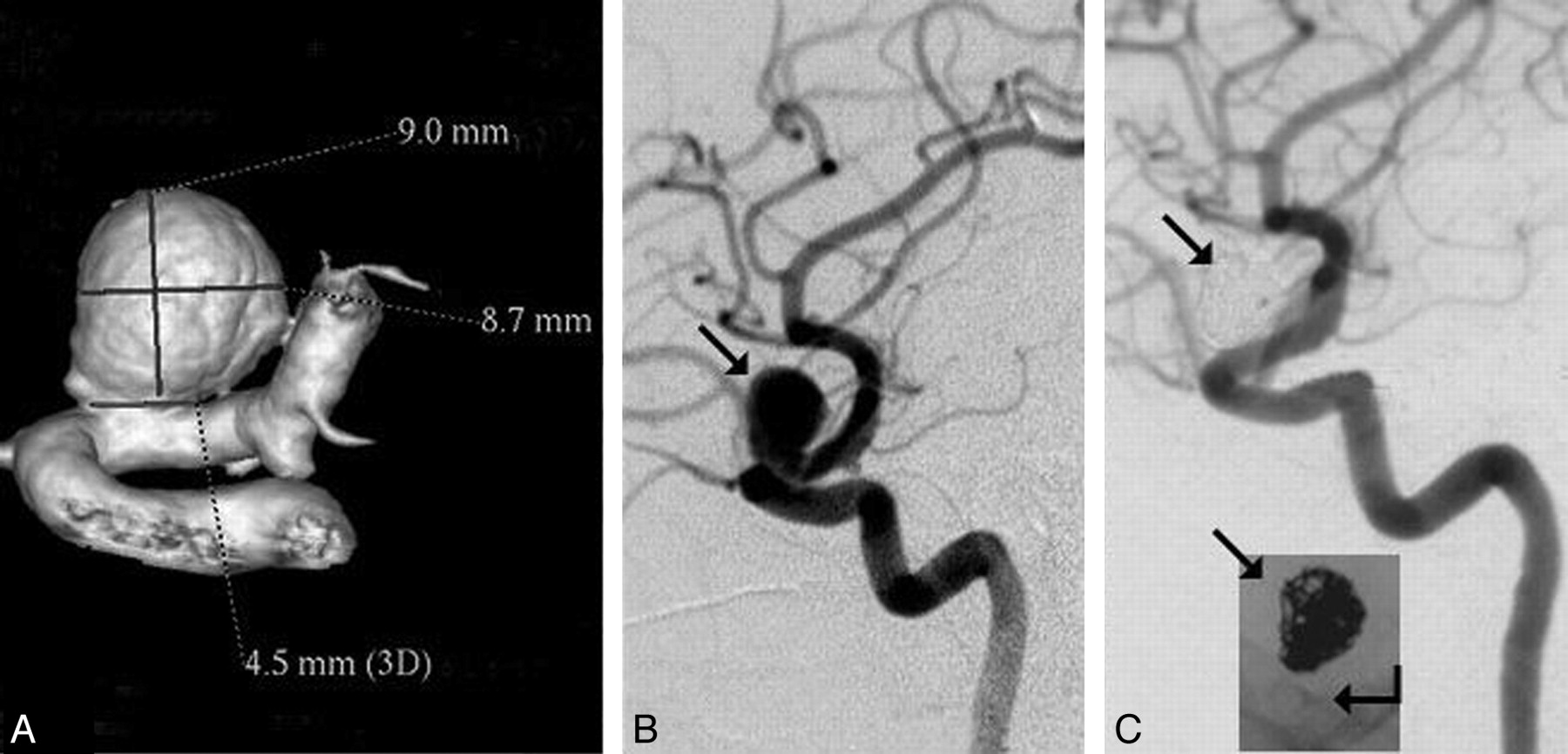
Results of aneurysm treatment by a combination of flow modification and additional coil packing. A and B, Nine-millimeter-diameter paraophthalmic aneurysm (arrow, B) treated with flow modification and coil packing (patient 3, On-line Table and Tables 1 and 2). C, Six-month follow-up angiogram demonstrates complete occlusion of the aneurysm with reconstruction of the parent artery. Arrows demonstrate subtraction artifacts and nonsubtracted view of the coil mass (23.3% volumetric packing attenuation); broken arrow demonstrates a single PED within the ICA.

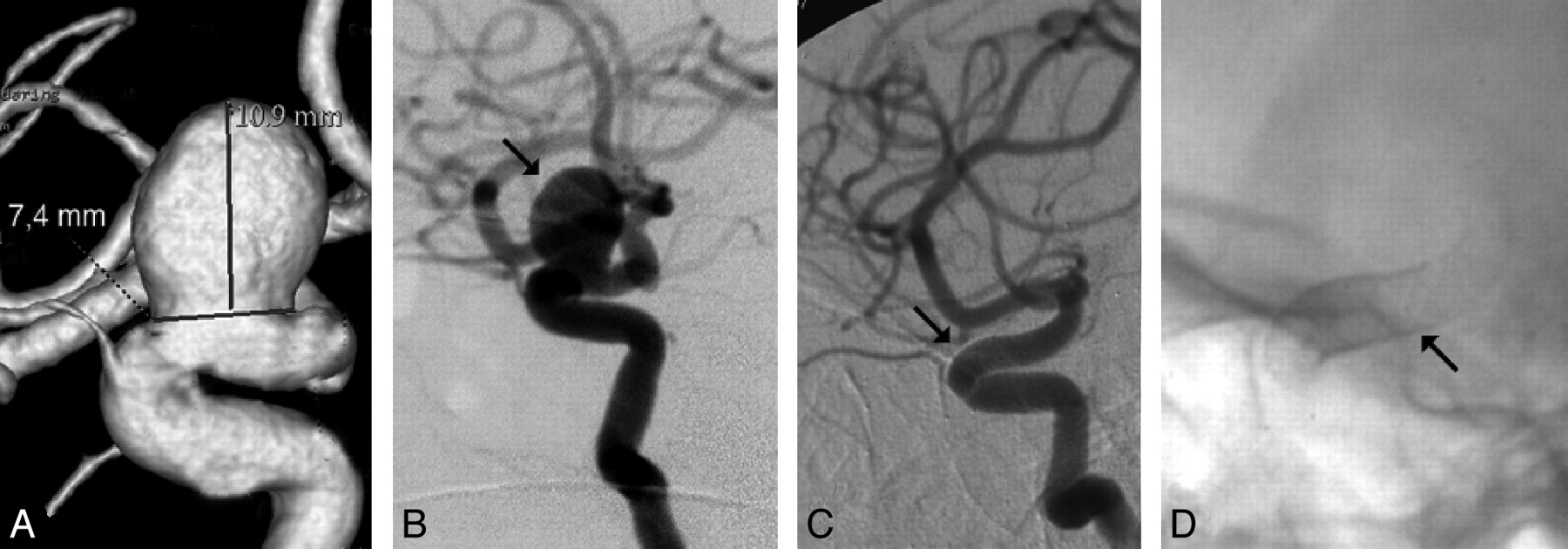
Results of aneurysm treatment with flow modification only. A and B, Aneurysm with size and location similar to the one on Fig 4 (10-mm diameter paraophthalmic ICA aneurysm; arrow, B) treated with flow modification only (patient 11, On-line Table and Tables 1 and 2). C, Six-month follow-up angiogram demonstrates complete occlusion of the aneurysm and reconstruction of the parent artery (arrow). D, Arrow represents 3 coaxial PEDs implanted for parent artery reconstruction. No coils were used.
Large and giant aneurysms treated exclusively with PEDs were demonstrated by cross-sectional imaging (CT or MR imaging) to have involuted, with resolution of mass effect in all patients at 6-month follow-up, except the patient with residual filling of her giant ICA aneurysm (Figs 1 and 3).
Clinical Follow-Up
Seven patients remained clinically unchanged. Six patients with compression syndromes have either completely or significantly improved. Five of 10 patients presenting with headaches reported relief of their symptoms. One patient died (On-line Table and Tables 1 and 2). There was no relationship between the immediate angiographic findings and clinical outcome (On-line Table and Tables 1 and 2).
Late Imaging Follow-Up
Eleven patients had late imaging follow-up by time-of-flight MRA. None of these patients had any new symptoms related to either their aneurysms or potential parent vessel stenosis or occlusion. All parent vessels were patent proximal and distal to the aneurysm, and no aneurysm recurrence was seen by MRA. The treated segment of the parent artery could not be visualized due to the limitations of the technique.
Discussion
The potential of intravascular stent technology in the treatment of aneurysms has been proposed, and its technical feasibility, assessed in animal experiments in the early 1990s.1–3 It was hypothesized that stent implantation may impact the results of endovascular treatment by facilitating attenuated coil-packing, modifying local flow dynamics, and providing a framework for the proliferating intima to cover the aneurysm.1
Further laboratory experiments demonstrated that depending on their mesh attenuation, stents alter and reduce the velocities of vortical flow within the aneurysm, increasing the intra-aneurysmal circulation time and affecting momentum exchange between the sac and the parent vessel.15 It was also shown that in addition to the porosity, the geometry of the stent has an impact on aneurysm thrombosis, depending on the local flow patterns.16,17
For clinical practice, following the application of modified balloon-expandable coronary stents,18 open cell self-expandable intracranial stents became available for the morphologic reconstruction of the parent vessel across the orifice of the aneurysm.12,13,18–24 More recently, closed cell-design stents were added to the therapeutic arsenal, presumably providing better coverage of the aneurysm neck.25–27 Even though most clinical reports published to date have mainly focused on the utility of stents in facilitating coil packing of complex neck aneurysms, several observations suggested that stents not only promote improved packing but may independently contribute to the long-term stability of the aneurysm even with lower packing attenuation.13,18 This assertion is supported by reports of aneurysms found to thrombose spontaneously after stent placement alone12,13 or following double-stent coverage of the orifice without coil packing,18 further highlighting the significance of stent design as proposed by Lieber et al15,16 and Barath et al17 in earlier experimental studies.
The above results allowed a conceptual change in the application of stent technology in aneurysm treatment. Instead of using stents as an adjunctive device, one can apply the intraluminar sleeves primarily for functional anatomic reconstruction of the parent artery by altering flow dynamics and inducing intimal proliferation. Early clinical experiences with 2 such devices, the Silk stent (Balt Extrusion, Montmorency, France)28 and the PED,29–31 have recently been reported. Nine of the 18 cases reported here are part of the first clinical trial designed to study the safety and efficacy of a flow-diverter device, the PED (the PITA trial).
Because our intention was to find an effective treatment technique for aneurysms otherwise difficult to treat, large, giant, fusiform, or wide-neck (as defined by a neck >4 mm or a neck-to-sac ratio <1:2) lesions were treated exclusively. Overall, the aneurysms were larger compared with those in most endovascular series, having a mean diameter of 16 mm and a mean volume of 1.26 cm3. The PED is a single layer of woven wire mesh design with a pore size of 0.020–0.052 mm2. Its flexibility and conformability to the implanted parent arteries were satisfactory. All devices were successfully navigated into position with moderate effort by using standard microcatheters. Two of 41 PEDs could not be deployed due to friction and were easily removed together with the microcatheter. Introduction and gentle inflation of a microballoon was necessary to release and fully open the distal tip of 1 PED that failed to detach from its delivery wire. This, too, was related to friction due to proximal tortuosity. Thirty-nine devices were acceptably deployed across the target lesion and apposed to the parent artery wall.
The exact degree of flow reduction sufficient for aneurysm thrombosis and its importance in achieving ultimate aneurysm occlusion are unclear and are likely to remain subjective in each case until flow and thrombosis simulations become incorporated into routine clinical practice. The aim is to prolong circulation time (contrast residence) within the aneurysm. Intra-aneurysmal circulation (vorticity) has been shown to be directly related to the surface area of the orifice32–34 and can be reduced by decreasing the free surface available for fluid exchange. PED provides approximately 30%–35% surface coverage at a nominal opening as a single layer, but its design allows the overlapping of multiple devices, which can be used to strategically increase the degree of aneurysm coverage, providing 2 options for significantly reducing intra-aneurysmal circulation: the primary use of multiple coaxial PEDs or (particularly where perforator branches restrict the number of PEDs that can safely be used) reducing intra-aneurysmal flow with adjunctive coiling of the aneurysm.10 In this series, we used both approaches.
In very large and giant aneurysms, in which it is difficult to achieve a significant effect on flow with coils, we elected to use multiple PED coverage. Aneurysms covered by ≥3 devices were practically twice as large as those treated with single or double PED coverage (On-line Table and Tables 1 and 2). To avoid occlusion of important side branches, we first used a single long bridging PED to create a stable scaffold, followed by shorter devices placed strategically over the aneurysm neck to enhance coverage of the orifice but minimize that of the parent artery proximal and distal to the aneurysm.
For smaller aneurysms, at the beginning, additional coiling was performed if complete stasis to the subjective satisfaction of the operator was not achieved. Technically, coil packing following PED coverage of the neck was very easy. With growing experience, we learned that complete stasis is not required for ultimate aneurysm occlusion; if the flow is visibly reduced by angiography, the aneurysm is likely to thrombose, and aneurysm packing is discontinued. Applying both techniques provided an opportunity for retrospective comparison of aneurysms that had additional coiling with those that were treated with PED coverage alone. Analysis of the 6-month follow-up results demonstrated that, in general, the coil-packing density was very low. Further, even though unpacked aneurysms had significantly larger volume than those that were adjunctively coiled (On-line Table and Tables 1 and 2), aneurysms of similar size and location occluded equally, regardless of coil packing (On-line Table and Tables 1 and 2, Figs 4 and 5). On the other hand, all but 1 coiled aneurysm was treated with a single PED, while unpacked aneurysms were covered by multiple overlapping devices. We concluded that for many aneurysms, PED coverage itself is an effective treatment, and for the future, we restricted additional coil packing to cases in which there is an increased risk of aneurysm rupture (such as multiple aneurysms) or the need to restrict PED coverage to a single device due to the vicinity of significant side branches.
Patency of side branches is a significant concern for the application of multilayer high-mesh-attenuation stents. In our study, 1 acute occlusion was attributed to severe catheter-induced ICA vasospasm rather than stent coverage. This was supported by the reopening of the ophthalmic artery at 6 months. Both branches that had delayed occlusion were covered by either 2 or 4 overlapping devices. A single-layer PED did not cause any side branch thrombosis. Having this positive experience in the relatively forgiving area of the supraclinoid ICA encouraged us to use the technique of targeted multilayer PED coverage in a large fusiform basilar trunk aneurysm, which was treated by 5 coaxial PEDs. In this case, coverage of the SCA and AICA segments was limited to single anchoring devices, while 3 additional short PEDs were overlapped across the aneurysm neck. No visible branches of the BA occluded, and no clinical signs of perforator-related ischemia were detected within 8 months of follow-up (Fig 3).
Another significant concern regarding high-metal-surface-area stents is their potential thrombogenicity, particularly if multiple devices are used. In-stent thrombosis occurred in 1 case in a patient retrospectively found not to have been suitably covered with antiplatelet agents. The occluded ICA reopened later, while the patient was on proper medication (Fig 2). This suggests that the PED has an acceptable thrombotic profile, but rigorous antiplatelet periprocedural medication is necessary.
Similar to the application of other intracranial stents, the necessity of aggressive antiaggregation raises further concerns about potential bleeding complications. In our study, a patient died due to diffuse SAH. This patient had a very small aneurysm on the ipsilateral ICA bifurcation distal to her giant multilobulated target aneurysm on the proximal ICA. Control angiography failed to demonstrate a source of bleeding; however, an autopsy suggested rupture of the small distal aneurysm, likely related to wire perforation. This suggests that patients having an additional aneurysm distal to the target lesion carry higher risk because perforation of the distal aneurysm may occur during the exchange maneuver or PED placement. While such perforation might otherwise remain clinically silent, it may become catastrophic under double antiaggregation. Treatment of the distal aneurysm before the target lesion should be considered.
The PED device demonstrated high efficacy, inducing complete occlusion in all but 1 aneurysm at 6 months. This was seen in the patient who had transient ICA occlusion and, for this reason, was kept on double antiplatelets for 6 months. She is due for further follow-up (Fig 2). All other aneurysms completely occluded at 6 months, with reconstruction of the lumen of the parent artery (Figs 1, 3, and 4). A minimal (15%) diameter narrowing was detected by follow-up angiography at 6 months in a single case without any flow restriction. The patient is being followed clinically and by MR imaging and MRA.
Effective treatment of mass effect is difficult with intrasaccular aneurysm packing. Treatment with flow diversion resulted not only in angiographic aneurysm occlusion but also in reduction of mass effect. This result is proved by the elimination or improvement of cranial nerve neuropathies and headaches as well as by involution of the aneurysmal mass and resolution of the mass effect at 6 months by CT or MR imaging (Figs 1 and 3).
The long-term results are yet to be studied. We do not have angiographic results for more than 6 months; however, time-of-flight MRA in 11 patients (12 aneurysms at 18–24 months) indicated persistent occlusion of the aneurysms and good flow within the parent arteries proximal and distal to the treated segments. Patients have been clinically followed for ≤12–18 months so far. No further clinical events have been recorded.
This article summarizes short-term results of only a small cohort of patients. On the basis of these results, application of this technology seems to be beneficial for patients with large and giant proximal aneurysms, particularly those having mass effect. Further studies are warranted to collect longer term follow-up data and to investigate the potential of the technique for treatment of more distally located aneurysms.
Conclusions
Treatment of large, wide-neck, or otherwise untreatable aneurysms with functional reconstruction of the parent artery may be achieved with relative safety by using dedicated flow-modifying devices. Currently available technology using the PED provides high efficacy with lasting effects in proximal intracranial sidewall aneurysms. Additional coil packing is not required to achieve aneurysm thrombosis, but it is technically feasible and can be applied if early aneurysm occlusion is desired (ie, acute SAH) or when treating aneurysms in which eloquent branch vessels limit the number of PEDs. Dual-agent antiaggregation seems to be essential in avoiding thromboembolic complications and needs to be seriously considered in cases of multiple aneurysms. Longer follow-up and larger studies are warranted.
Footnotes
-
This work was partially supported by a grant from the Hungarian National Scientific and Research Fund (OTKA 73773).
-
Indicates article with supplemental on-line table.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received September 25, 2009.
- Accepted after revision November 16, 2009.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Embolization of Ruptured and Unruptured Aneurysms with the Contour Neurovascular System--Summary of 106 Cases
- Comparison of flow diverter alone versus flow diverter with coiling for large and giant intracranial aneurysms: systematic review and meta-analysis of observational studies
- Magnetic resonance perfusion imaging findings following flow diversion in patients with complex middle cerebral artery bifurcation aneurysms: a single-center analysis regarding the jailed cortical branches
- Flow diversion for compressive unruptured internal carotid artery aneurysms with neuro-ophthalmological symptoms: a systematic review and meta-analysis
- Flow diversion for compressive unruptured internal carotid artery aneurysms with neuro-ophthalmological symptoms: a systematic review and meta-analysis
- Comparison of the Pipeline embolisation device alone or combined with coiling for treatment of different sizes of intracranial aneurysms
- Postoperative occlusion degree after flow-diverter placement with adjunctive coiling: analysis of complications
- Endovascular treatment of vertebral artery dissecting aneurysms : a 20-year institutional experience
- Feasibility study for use of angiographic parametric imaging and deep neural networks for intracranial aneurysm occlusion prediction
- Advances in endovascular aneurysm management: flow modulation techniques with braided mesh devices
- Outcome of intracranial flow diversion according to the antiplatelet regimen used: a systematic review and meta-analysis
- Outcome Study of the Pipeline Embolization Device with Shield Technology in Unruptured Aneurysms (PEDSU)
- Pipeline embolization device treatment of internal carotid artery terminus aneurysms
- Antiplatelet therapy and the risk of ischemic and hemorrhagic complications associated with Pipeline embolization of cerebral aneurysms: a systematic review and pooled analysis
- Flow-Diversion Treatment of Unruptured Saccular Anterior Communicating Artery Aneurysms: A Systematic Review and Meta-Analysis
- Long-term visual outcome in patients treated by flow diversion for carotid-ophthalmic aneurysms
- LVIS Blue as a low porosity stent and coil adjuvant
- Risk of Branch Occlusion and Ischemic Complications with the Pipeline Embolization Device in the Treatment of Posterior Circulation Aneurysms
- Quantitative flow measurement after placing a flow diverter for a distal internal carotid artery aneurysm
- Early angiographic signs of acute thrombus formation following cerebral aneurysm treatment with the Pipeline embolization device
- An outcomes-based grading scale for the evaluation of cerebral aneurysms treated with flow diversion
- Thrombogenicity of flow diverters in an ex vivo shunt model: effect of phosphorylcholine surface modification
- Selection of helical braided flow diverter stents based on hemodynamic performance and mechanical properties
- Periprocedural outcomes and early safety with the use of the Pipeline Flex Embolization Device with Shield Technology for unruptured intracranial aneurysms: preliminary results from a prospective clinical study
- Large Basilar Apex Aneurysms Treated with Flow-Diverter Stents
- Cerebral aneurysm treatment: modern neurovascular techniques
- Treatment of posterior circulation non-saccular aneurysms with flow diverters: a single-center experience and review of 56 patients
- Compacting a Single Flow Diverter versus Overlapping Flow Diverters for Intracranial Aneurysms: A Computational Study
- Collar Sign in Incompletely Occluded Aneurysms after Pipeline Embolization: Evaluation with Angiography and Optical Coherence Tomography
- Carotid cavernous fistula after Pipeline placement: a single-center experience and review of the literature
- Efficacy and Safety of the Woven EndoBridge (WEB) Device for the Treatment of Intracranial Aneurysms: A Systematic Review and Meta-Analysis
- Does Arterial Flow Rate Affect the Assessment of Flow-Diverter Stent Performance?
- Pipeline embolization device for the treatment of vertebral artery aneurysms: the fate of covered branch vessels
- Flow Diversion for Ophthalmic Artery Aneurysms
- Endovascular treatment of ophthalmic artery aneurysms: ophthalmic artery patency following flow diversion versus coil embolization
- Risk Factors for Ischemic Complications following Pipeline Embolization Device Treatment of Intracranial Aneurysms: Results from the IntrePED Study
- Grading of Regional Apposition after Flow-Diverter Treatment (GRAFT): a comparative evaluation of VasoCT and intravascular OCT
- Immediate procedural outcomes in 44 consecutive Pipeline Flex cases: the first North American single-center series
- Pipeline Embolization Device with or without Adjunctive Coil Embolization: Analysis of Complications from the IntrePED Registry
- Flow diversion treatment of complex bifurcation aneurysms beyond the circle of Willis: a single-center series with special emphasis on covered cortical branches and perforating arteries
- Endovascular treatment of intracranial aneurysms using the Pipeline Flex embolization device: a case series of 30 consecutive patients
- Intravenous C-Arm Conebeam CT Angiography following Long-Term Flow-Diverter Implantation: Technologic Evaluation and Preliminary Results
- SILK flow diverter for complex intracranial aneurysms: a Canadian registry
- Flow Diverter Therapy With the Pipeline Embolization Device Is Associated With an Elevated Rate of Delayed Fluid-Attenuated Inversion Recovery Lesions
- Flow diversion of large internal carotid artery aneurysms with the surpass device: impressions and technical nuance from the initial North American experience
- Effect of antiplatelet therapy and platelet function testing on hemorrhagic and thrombotic complications in patients with cerebral aneurysms treated with the pipeline embolization device: a review and meta-analysis
- Intra-aneurysmal flow rates are reduced by two flow diverters: an experiment using tomographic particle image velocimetry in an aneurysm model
- Pipeline endovascular device for the treatment of intracranial aneurysms at the level of the circle of Willis and beyond: multicenter experience
- Initial Experience with p64: A Novel Mechanically Detachable Flow Diverter for the Treatment of Intracranial Saccular Sidewall Aneurysms
- Utilization of Pipeline embolization device for treatment of ruptured intracranial aneurysms: US multicenter experience
- Preliminary experience with the Pipeline Flex Embolization Device: technical note
- Flow diverters: inter and intra-rater reliability of porosity and pore density measurements
- Periprocedural and mid-term technical and clinical events after flow diversion for intracranial aneurysms
- Evolution of Flow-Diverter Endothelialization and Thrombus Organization in Giant Fusiform Aneurysms after Flow Diversion: A Histopathologic Study
- Critical assessment of complications associated with use of the Pipeline Embolization Device
- Long-Term Follow-Up Results following Elective Treatment of Unruptured Intracranial Aneurysms with the Pipeline Embolization Device
- Posterior circulation flow diversion: a single-center experience and literature review
- Primary endovascular treatment of post-irradiated carotid pseudoaneurysm at the skull base with the Pipeline embolization device
- Radiation dose analysis of large and giant internal carotid artery aneurysm treatment with the pipeline embolization device versus traditional coiling techniques
- Anterior Choroidal Artery Patency and Clinical Follow-Up after Coverage with the Pipeline Embolization Device
- Failure of aneurysm occlusion by flow diverter: a role for surgical bypass and parent artery occlusion
- Extra-Aneurysmal Flow Modification Following Pipeline Embolization Device Implantation: Focus on Regional Branches, Perforators, and the Parent Vessel
- Association between hemodynamic conditions and occlusion times after flow diversion in cerebral aneurysms