
The use of checklists is well-established in aviation, where their application is an integral part of every sequence of flying.1 In cases of emergency flying procedures, the use of checklists is fundamental in dealing with critical tasks, and their application is a central part of pilot training and pilot performance.2
Checklists have only recently been introduced in medicine in an effort to manage a number of procedures in a uniform manner, according to the established standard of care.3 While suited especially for complex or emergency tasks, the application of a checklist in reducing morbidity and mortality for the placement of a central line has gained wide recognition.4–7
Recently, Atul Gawande, a surgeon at Harvard Medical School, has published his experience with checklists in medicine, aviation, and building construction, in his book The Checklist Manifesto: How to Get Things Right.8 The book details his experience in developing a checklist for the World Health Organization in its global effort to reduce the morbidity and mortality of surgical interventions. The checklist incorporated 19 simple items, ranging from the identification of the correct patient and correct surgical site to confirming the application of preoperative antibiotics and making sure all team members in the operating room know each other and their respective roles.8,9 Their initial results, published in the New England Journal of Medicine in 2009, showed dramatic results in reducing both morbidity and mortality at the pilot study sites.9
This effort has led us to believe that checklists have the potential of becoming significant tools in making medicine, and more specifically interventions, safer.3 From a neurointerventional point of view, it was the belief the authors, comprising both neurointerventionalists (G.L., H.C., D.K.) and neurosurgeons (Ph.T., G.L.), that the perforation of aneurysms during coiling is one of the most critical events in the neurointerventional field. The correct response in these instances is guided not only by experience but also by taking the correct measures, with a large number of steps involving clinical, interventional, anesthesiologic, and organizational aspects. As a result, a checklist may help both the experienced and less experienced practitioner to react in the event of aneurysmal rupture according to the best standard of care.10
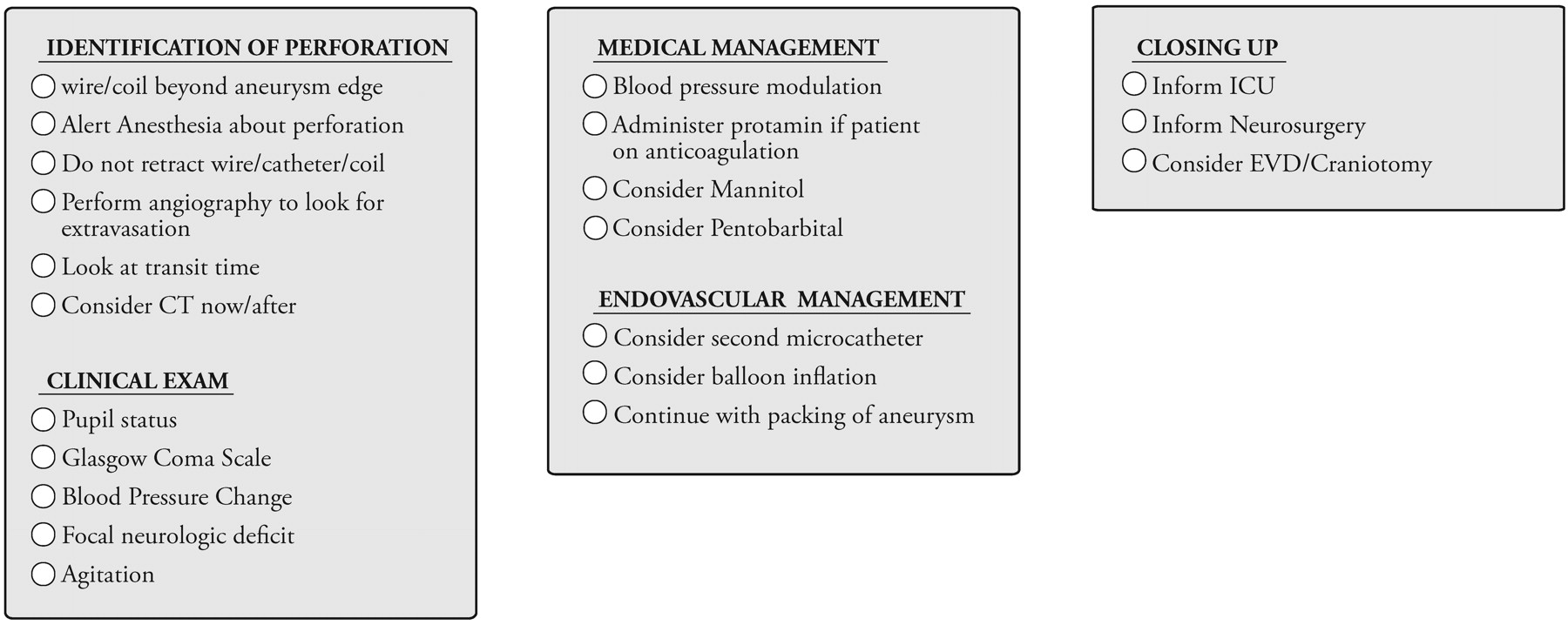
The checklist (Fig 1) proposed here is an initial effort to translate the personal and published experience of both neurosurgeons and neuroradiologists regarding the handling of an aneurysmal perforation during coiling according to the best standard of care. At the heart of this effort is the inspiration of Atul Gawande's book, and we are eager to have the checklist used, studied, and improved.
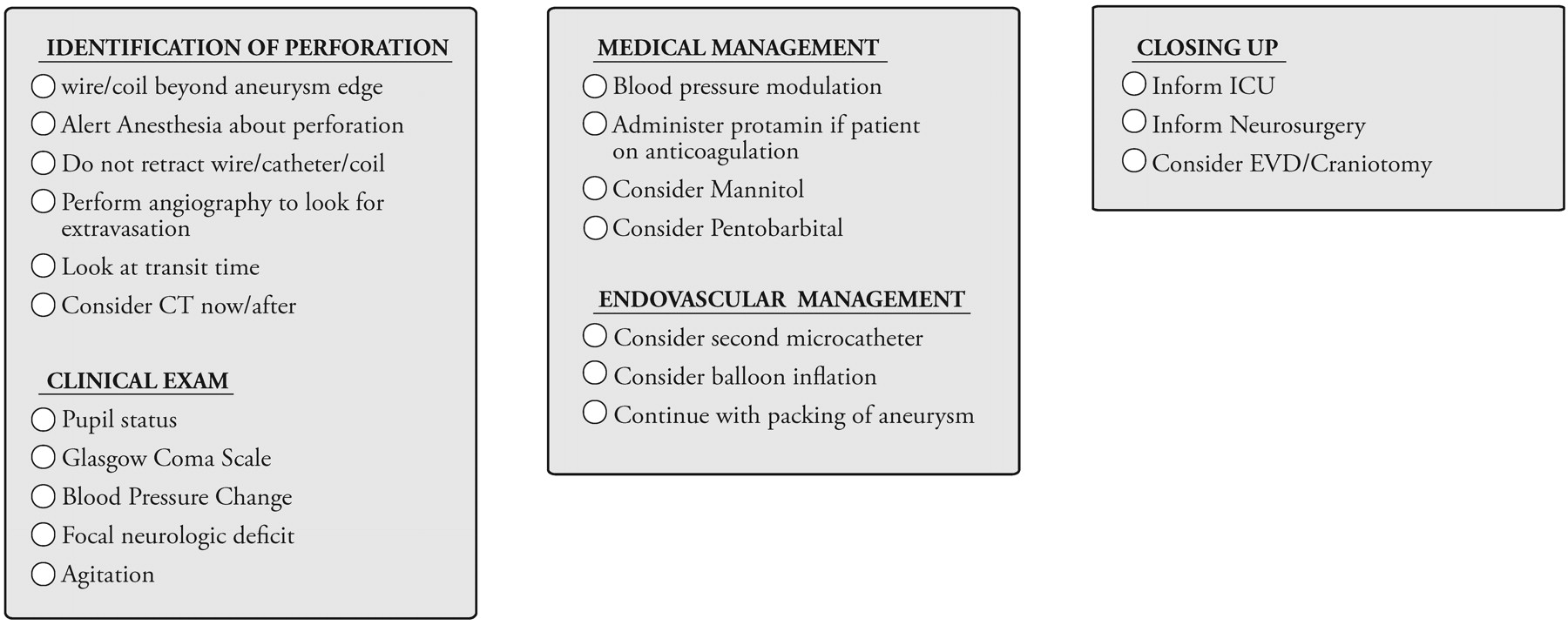
Checklist for aneurysm perforation during coiling. ICU indicates intensive care unit; EVD, external ventricular drain.
References
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.