
Abstract
BACKGROUND AND PURPOSE: The duration of the fracture is considered by many practitioners to be an important predictor of outcome following vertebroplasty. We sought to define the impact of preprocedural pain duration on outcomes, including pain relief, improvement in function, and medication usage among patients treated with single-level vertebroplasty.
MATERIALS AND METHODS: Institutional review board approval was obtained before conducting this retrospective analysis of 321 patients undergoing single-level vertebroplasty at our institution. Fractures were categorized as acute (≤6 weeks, n = 153), subacute (6–24 weeks, n = 124), and chronic (>24 weeks, n = 44). Pain NRS (0–10) scores at rest and with activity and RDS were compared among 3 groups at baseline and post procedure. Also absolute and proportional improvement of pain NRS and RDS were compared among 3 groups by using ANOVA. Linear regression was performed between preoperative pain duration and symptom improvement for each group.
RESULTS: Baseline RDS and pain NRS with activity and at rest were not significantly different among groups (P = .09, .30, and .91, respectively). Mean improvement in pain NRS with activity at 1 month postvertebroplasty in acute (improvement = 4.9 ± 3.5), subacute (improvement = 4.2 ± 3.2), and chronic fractures (improvement = 4.5 ± 3.2) was similar among groups (P = .28). Mean improvement in RDS at 1 month postprocedure was 9.6, 8.3, and 9.9, for acute, subacute, and chronic fractures, respectively (P = .56). There was no strong correlation between length of pain and symptom improvement.
CONCLUSIONS: The age of fracture has minimal impact on outcome following single-level vertebroplasty, with good outcomes noted among patients with acute, subacute, and chronic fractures.
Abbreviations
- ANOVA
- analysis of variance
- NRS
- numeric rating scale
- RDS
- Roland Disability Scale
- VAS
- Visual Analog Scale
- VERTOS
- Percutaneous Vertebroplasty versus Conservative Therapy
Percutaneous vertebroplasty is widely used for the treatment of painful vertebral compression fractures. Numerous clinical and radiographic features are considered relevant in selecting patients for the procedure. Since the advent of vertebroplasty, fracture duration has been a key consideration in whether to intervene. Many previous publications, as well as guidance documents from the US Food and Drug Administration,1 have suggested that vertebroplasty be offered only after a course of failed medical therapy, on the order of 4–6 weeks' duration.2–6 However, as the procedure became routine, early vertebroplasty has become routine. The recently published VERTOS II7 study highlights the potential benefit of early vertebroplasty.
Notwithstanding the perceived importance of fracture duration in predicting outcome, few previous studies have specifically addressed this point. In the current study, we compared response to vertebroplasty among 3 groups of patients, with acute (<6 weeks), subacute (6–24 weeks), and chronic (>24 weeks) fracture duration to determine whether fracture duration impacted outcome following vertebroplasty.
Materials and Methods
Institutional review board approval was granted for this study. We have previously published retrospective reviews of these same patients in a number of studies, but the relation between preoperative pain and symptom improvement has never previously been evaluated in this cohort. A retrospective chart review was performed on all patients undergoing vertebroplasty at our tertiary care institution between February 1999 and October 2009. We then identified patients who had undergone a single-level vertebroplasty to minimize the influence of multiple fractures on outcome. Other inclusion criteria were the availability of complete preoperative evaluation notes and the lack of additional vertebroplasty procedures within the next year after the procedure to avoid potential confounding effects of subsequent vertebroplasty procedures.
Preprocedural physical examination along with evaluation with plain radiographs, MR imaging, and bone scanning were performed to determine the eligibility of patients for vertebroplasty. During preoperative interviews, neuroradiologists and trained vertebroplasty nurses routinely requested patients to rate their pain at rest and with activity by using a pain NRS (0–10) and the modified RDS.8 Postoperative follow-up was performed at 2 hours' postprocedure by interview and examination. Telephone follow-ups were completed at 1 week, and at 1, 6, and 12 months after the procedures.
On the basis of preoperative pain duration, patients were divided into those with acute fractures (≤6 weeks' duration), subacute fractures (6–24 weeks' duration), and chronic fractures (>24 weeks' duration). Within each group, treated thoracic and lumbar levels were compared separately. Preoperative evaluation notes were reviewed to determine the length of pain before vertebroplasty. Outcomes included absolute pain NRS and RDS and improvement in pain NRS and RDS. Symptom improvement was analyzed as both raw numbers and as percentages of baseline scores.
Mobility was evaluated on the basis of the following categorizations: unrestricted, able to walk >1 block, able to walk only <1 block, and bedridden at baseline. We graded mobility changes at each follow-up time point compared with baseline using the following scores: improved = 2, remained unchanged = 1, or decreased = 0.
Analgesic medication use was categorized as non-narcotic, occasional narcotic, regular narcotic, and parental narcotic at baseline and at follow-up. The changes in medication usage were graded as the following: discontinued = 3, decreased = 2, no change = 1, or increased = 0 compared with baseline.
Statistical Analysis
ANOVA was used to compare absolute pain NRS and RDS, improvement (raw difference in mean) in pain NRS and RDS, and percentage of improvement (raw difference divided by baseline scores) in pain NRS and RDS among the 3 groups. χ2 was performed to find differences in medication usage and mobility improvements among groups. Linear regression analysis was used to evaluate the correlation between preoperative pain duration (independent variable) and improvement in pain NRS, RDS, mobility, and analgesic medication use (dependent variable) at each follow-up time point for all patients. Because of the multiple comparisons used (n = 30), a Bonferroni correction was used by dividing the α level (.05) by 30, with P < .002 considered significant. All statistical analyses were performed by JMP 8.0, (SAS Institute, Cary, North Carolina).
Results
In total, 1751 vertebral fractures were treated during 1187 vertebroplasty procedures in 979 patients. Among these, 701/979 (72%) patients had preoperative pain scores both at rest and with activity and at least 1 postoperative follow-up point. Preoperative evaluation notes were available for 617/701 (88%), and preoperative pain durations were included in 592/617 (95%) of these patients with available clinical notes. Within 1 year of the first vertebroplasty, 72/592 (12%) patients underwent a second procedure and were excluded. After these exclusions, 520 patients remained. We then identified 321/520 (62%) patients who had undergone a single-level vertebroplasty with adequate clinical information for analysis.
Age and demographics are listed in Table 1. Sixty-six percent of patients were women, and the median (range) age was 76 years (range, 32–96 years). The mean preoperative pain duration was 12.2 ± 15.1 weeks, and the median was 6.9 weeks (range, 0.3–154.3 weeks). The mean preoperative pain at rest and with activity and the RDS were 4.1 ± 3.1, 8.1 ± 2.0, and 18.1 ± 3.9, respectively. The baseline characteristics of the 3 groups, including acute, subacute, and chronic fractures, are shown in Table 1. There was no significant difference among groups at baseline.
Patient demographics
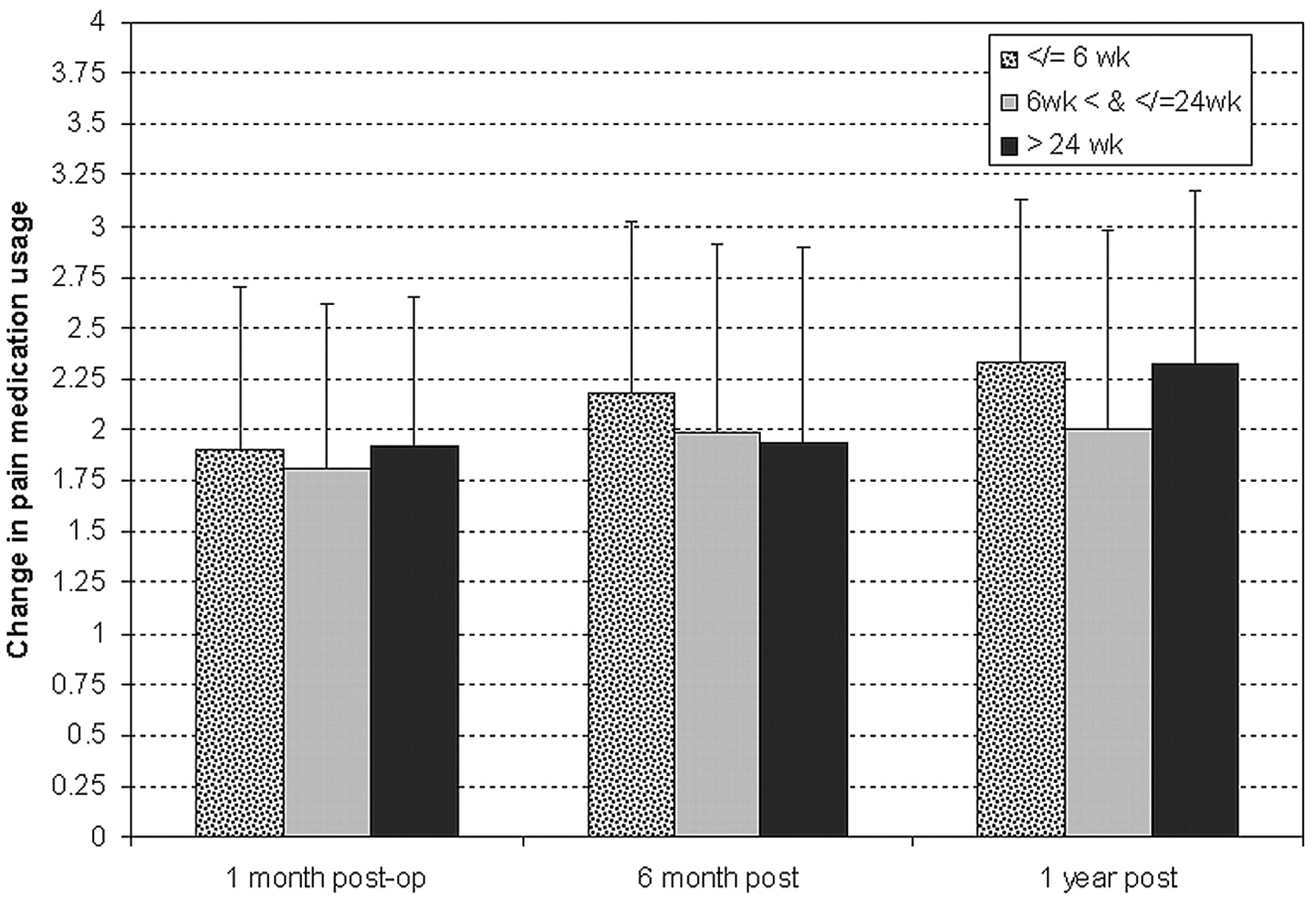
Absolute pain and disability, both raw numbers and as percentage of baseline, were not significantly different among groups at any follow-up time point (Fig 1 and Table 2). Medication use and mobility scores were similar among groups (Figs 2 and 3).

Pain scores at rest (A), with activity (B), and RDS improvement (C).

Change in pain medication use among subgroups: discontinued = 3, decreased = 2, no change = 1, and increased = 0.

Mobility improvement among subgroups: improvement = 2, unchanged = 1, and decreased = 0.
Pain-with-activity VAS (0–10) in the thoracic and lumbar levels in each period of preoperative pain
Among 321 levels, there were 151 thoracic levels with a mean of 12.5 ± 15.0 weeks' and 170 lumbar levels with a mean of 11.9 ± 15.1 weeks' preoperative pain duration (P = .69).
The comparisons of pain with activity between these 2 are shown in Table 2.
There were no positive or negative correlations between preoperative pain duration and pain improvement (absolute and percentage of baseline) at rest or with activity or on the RDS in any follow-up time points (Table 3).
Correlation between preoperative pain duration and symptom improvement at different follow-up time points
Our study had a power of 99%, 92%, and 56% to detect 1 unit of change in pain at rest or with activity and RDS scores, respectively, among groups.
Discussion
In the current study, we failed to detect any correlation between the age of the fracture before vertebroplasty and the outcome following vertebroplasty. The degree of pain relief and functional improvement was similar among patients with acute, subacute, and chronic fractures treated with vertebroplasty. Furthermore, the proportion of patients who noted improved mobility and decreased reliance on opioid medications was similar among groups. These trends persisted for up to 1 year following vertebroplasty. Taken together, our results suggest that the age of the fracture at presentation should not necessarily impact the decision to offer vertebroplasty.
Multiple other single-center studies have reported outcomes following vertebroplasty as a function of fracture age; most of these studies failed to demonstrate differences in outcome based on preprocedural fracture age. Alvarez et al9 failed to detect any statistical association between fracture age and pain improvement in a cohort of 423 levels treated with vertebroplasty. Kaufmann et al10 described 122 levels treated with vertebroplasty, with a mean age of fracture of 19 weeks, with a range of 1–104 weeks; those authors found no correlation between outcome and pain duration up to 1 year following vertebroplasty. Erkan et al11 reported 52 levels treated with kyphoplasty in 2 groups of patients with acute pain (mean, 6.2 weeks) and chronic pain (mean, 27.5 weeks). At almost all follow-up points, the authors detected no significant differences between groups.11 A single study by Jin et al12 found, in a cohort of 383 vertebroplasty procedures on 215 patients, that a shorter period between fracture and procedure provided relatively more satisfaction with vertebroplasty among treated patients. These same authors found an inverse relationship between preprocedural fracture age and pain improvement.12 Our study adds to this previous literature by focusing on a relatively homogeneous population—that is, patients with single-level fractures—and by providing data regarding not only pain relief but also functional outcome, mobility, and medication usage.
The recent publication of 2 placebo-controlled trials noting no benefit of vertebroplasty over a sham procedure has led numerous commentators to suggest that the observed lack of benefit resulted from the chronicity of fractures treated in those studies.13,14 One of these studies enrolled patients with a mean duration of pain of 16 weeks, whereas the other study had a mean duration of pain of 9 weeks. These criticisms regarding the sham studies and fracture duration are perhaps even more relevant because the publication of the VERTOS II study, in which patients treated at a mean fracture duration of approximately 5.5 weeks achieved markedly better improvements in pain and function than those treated with conservative management. Our current series, however, suggests that fracture duration alone likely cannot account for disparate outcomes seen among the recently published randomized trials. The next steps in investigating the impact of fracture duration on outcome might be to conduct a prospective randomized study.
This study had numerous limitations. It was retrospective, and follow-up was imperfect. Fracture age may be difficult to determine with accuracy in some patients. Finally, there was no control group included, so outcomes remain difficult to interpret.
Conclusions
The age of fracture has minimal impact on outcome following single-level vertebroplasty, with good outcomes noted among acute, subacute, and chronic fractures.
Footnotes
-
Disclosures: David Kallmes. Research Support (including provision of equipment or materials): Cook ArthroCare, CareFusion, Stryker, Details: support for clinical trial, Consultant: CareFusion, Details: preparation of educational materials, funds go to the institution.
References
- Received January 24, 2011.
- Accepted after revision February 26, 2011.
- © 2011 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}