
Abstract
BACKGROUND AND PURPOSE: Contrast-enhanced head and neck MRA may be degraded by venous stasis and reflux of contrast into the jugular veins. The purpose of this study was to evaluate the relationship between venous stasis and reflux and the side of injection and other causal factors.
MATERIALS AND METHODS: One hundred twenty-six consecutive patients (94 males and 32 females) who underwent contrast-enhanced MRA were evaluated for the side of contrast injection (left, n = 65; right, n = 61), hypertension, and cardiac disease. The retrosternal space was measured in all patients with left-arm injections.
RESULTS: Eight patients (6.34%) had reflux into the jugular veins. The difference in the mean ages of patients with and without reflux was not significant (P = .069). There was a significant difference in the incidence of systemic hypertension in patients with (77.78%) and without reflux (23.73%; P = .007). There was no significant difference in the incidence of cardiac disease in patients with and without reflux (P = .323). The difference in the side of injection in patients with and without reflux (P = .005) and the difference in the mean retrosternal distance in the patients with left-arm injection with (7.2 mm) and without reflux (12.1 mm) were statistically significant (P < .001).
CONCLUSIONS: Compression of the left brachiocephalic vein between the sternum and a tortuous aorta and proximal vessels may lead to venous reflux that can degrade the quality of contrast-enhanced MRA. Our study suggests that venous reflux can be avoided by routinely injecting right-sided veins.
Abbreviations
- FLASH
- fast low-angle shot
- MIP
- maximum intensity projection
- MRA
- MR angiograpy
Contrast-enhanced MRA is a noninvasive and safe method for the evaluation of head and neck vessels, without the attendant risks of conventional angiography. It is preferred over time-of-flight angiography because contrast medium reduces the T1 relaxation time of blood and virtually eliminates the effect of saturation. The combination of short contrast-bolus injection time and image-acquisition time requires precise timing to achieve high-quality MRA without venous contamination.1 For the purpose of acquiring an optimal contrast-enhanced carotid MRA, image acquisition should occur at the peak concentration of contrast medium during the first pass.2 We have noticed several cases with reflux of contrast into the jugular veins leading to suboptimal opacification of the carotid arteries. We have also noticed that most cases with significant venous reflux involved left-sided injections.
Therefore, we designed a comparative study to test the hypothesis that left-arm injection led to a higher incidence of reflux, degrading the quality of the MRA. The purpose of this study was to evaluate the relationship between venous stasis and reflux and the side of injection and other causal factors.
Materials and Methods
One hundred twenty-six consecutive patients who underwent contrast-enhanced head and neck MRA for various indications during 4 months (from October 2009 to January 2010) were included in this retrospective study. The population consisted of 94 males and 32 females with a mean age of 46.78 years (range, 6–81 years). Contrast was injected via either the left (n = 65) or the right (n = 61) antecubital vein. In all cases, contrast-enhanced MR imaging studies were performed after confirming that serum creatinine levels were normal (<1.2 mg/dL).
From the medical records of these patients, the blood pressure values and history of any concurrent cardiac disease were obtained. Systemic hypertension was defined as blood pressure values >140/90 mm Hg.3
In the patients with left-sided injection, to determine any abnormality in the mediastinum or compression of the left brachiocephalic vein between the arch of the aorta and the sternum, we measured the shortest anteroposterior distance between the posterior cortex of the sternum and the anterior aspect of the arch of aorta or its branches (retrosternal distance).
Repeat contrast-enhanced MRA was performed at an interval of 2–4 days in 3 patients with venous reflux to evaluate the neck arteries and the left brachiocephalic vein. For performing the repeat studies, contrast was injected via the contralateral antecubital vein in 2 patients and via a central venous catheter in 1 patient.
Informed consent was obtained before all the studies for the administration of contrast for MRA.
Imaging Technique
MRA was performed by using a 1.5T MR imaging system (Magnatom Avanto; Siemens, Erlangen, Germany). In all cases, examinations were performed by using the head and neck coil without breath-hold. A 3D-FLASH dynamic contrast-enhanced MRA sequence was used. Image parameters for 3D-FLASH were a TR of 3.52 ms, a TE of 1.1 ms, a 30° flip angle, a 205 × 384 matrix, a 246.7 × 370 mm FOV, and a single slab with 88 sections of 1.00-mm effective thickness and 20% interslice gap. Gadolinium chelate (0.2 mmol/kg of gadobenate dimeglumine section, MultiHance; Bracco, Milan, Italy) was bolus-injected by a power injector (Medtronics MR injector; Medtron, Saarbrücken, Germany) at a rate of 1 mL/s via a 20-ga peripheral intravenous catheter in either antecubital vein with the arm by the patient's side in a neutral position. This was immediately followed by a 15-mL saline flush injected at the same rate. The C.A.R.E. (Combined Application to Reduce Exposure; Siemens, Erlangen, Germany) bolus technique was used to determine the delay from the start of injection. Four dynamic images were acquired. The acquisition time of each phase was 10.8 seconds.
The source images of all patients with injection from the left antecubital vein were reconstructed in the axial plane, to assess the anterior mediastinum. Repeat contrast-enhanced MRA was performed in 3 patients.
Image Analysis
The images were assessed in consensus by 2 experienced neuroradiologists (B.T. and C.K.). The first phase of the contrast-enhanced MRA was assessed for the side of contrast injection, venous stasis, reflux of contrast into the jugular veins, opacification of the epidural collateral veins, and adequacy of visualization of the carotid arteries. On the axial reconstructions of the source images, the shortest anteroposterior distance between the posterior cortex of the sternum and the anterior aspect of the arch of the aorta or its branches was measured in all patients with left-sided injections.
Statistical Analysis
The Statistical Package for the Social Sciences software, Version 17.0 (SPSS, Chicago, Illinois) was used for statistical analysis. Differences for the incidence of hypertension, cardiac disease, and side of injection between patients with and without venous reflux were tested for statistical significance by using the χ2 test. The mean ages of patients with and without venous reflux were compared by using the t test. In all patients with left-sided injections, the mean anteroposterior distance between the posterior cortex of the sternum and the anterior aspect of the arch of aorta in patients with and without venous reflux was compared by using both the 1-way analysis of variance test and the t test. A P value < .05 indicated statistical significance.
Results
Eight patients of 126 developed significant venous reflux, which made their studies unacceptable for interpretation. There were no studies of suboptimal quality in the MRA studies without reflux. The mean age of patients with reflux was 51.57 ± 9.239 years (age range, 35–63 years). Of the 118 patients without reflux, the mean age was 47.18 ± 17.625 years (age range, 6–81 years). This difference was not statistically significant (P = .069).
From the medical records, we could get details of the blood pressure of 69 (54.76%) of our patients, of whom 34 (27.0%) had systemic hypertension and 35 (27.8%) were normotensive. The blood pressure status was not known in the rest of the patients. There was a significant difference in the incidence of systemic hypertension in patients with (77.78%) and without reflux (23.73%, P = .007).
Congestive cardiac failure was excluded in all patients. Details of other cardiac diseases were known in 67 (53.2%) patients, of whom 15 (11.9%) had cardiac disease and 52 (41.3%) had no cardiac disease. In others, detailed cardiac evaluation was not performed. There was no statistically significant difference in the incidence of cardiac disease in patients with and without reflux (P = .323).
In 65 (51.6%) patients, contrast was injected from the left antecubital vein. Eight (12.3%) patients had reflux (Fig 1A) so that the carotid and vertebral arteries were not opacified and the MRA was not diagnostic. Of these 8 patients, MRA was repeated in 3 patients (2 via the right antecubital vein and 1 via a central venous catheter). None of these patients showed reflux of contrast into the venous system in the repeat MRA (Fig 1B). In 61 (48.4%) patients, contrast was injected from the right antecubital vein. None (0%) of these patients had reflux into the internal jugular vein, and all the MRAs were diagnostic. The difference in the side of injection in patients with and without reflux was statistically significant (P = .005).

A, MIP image of MRA with injection from the left arm shows reflux of contrast in both jugular veins and the epidural venous plexus with poor opacification of the arterial system. B, In the same patient, the MIP image of MRA repeated after 4 days with injection from the right arm shows adequate opacification of the arterial system without venous reflux. Also note the ectatic arch of the aorta.
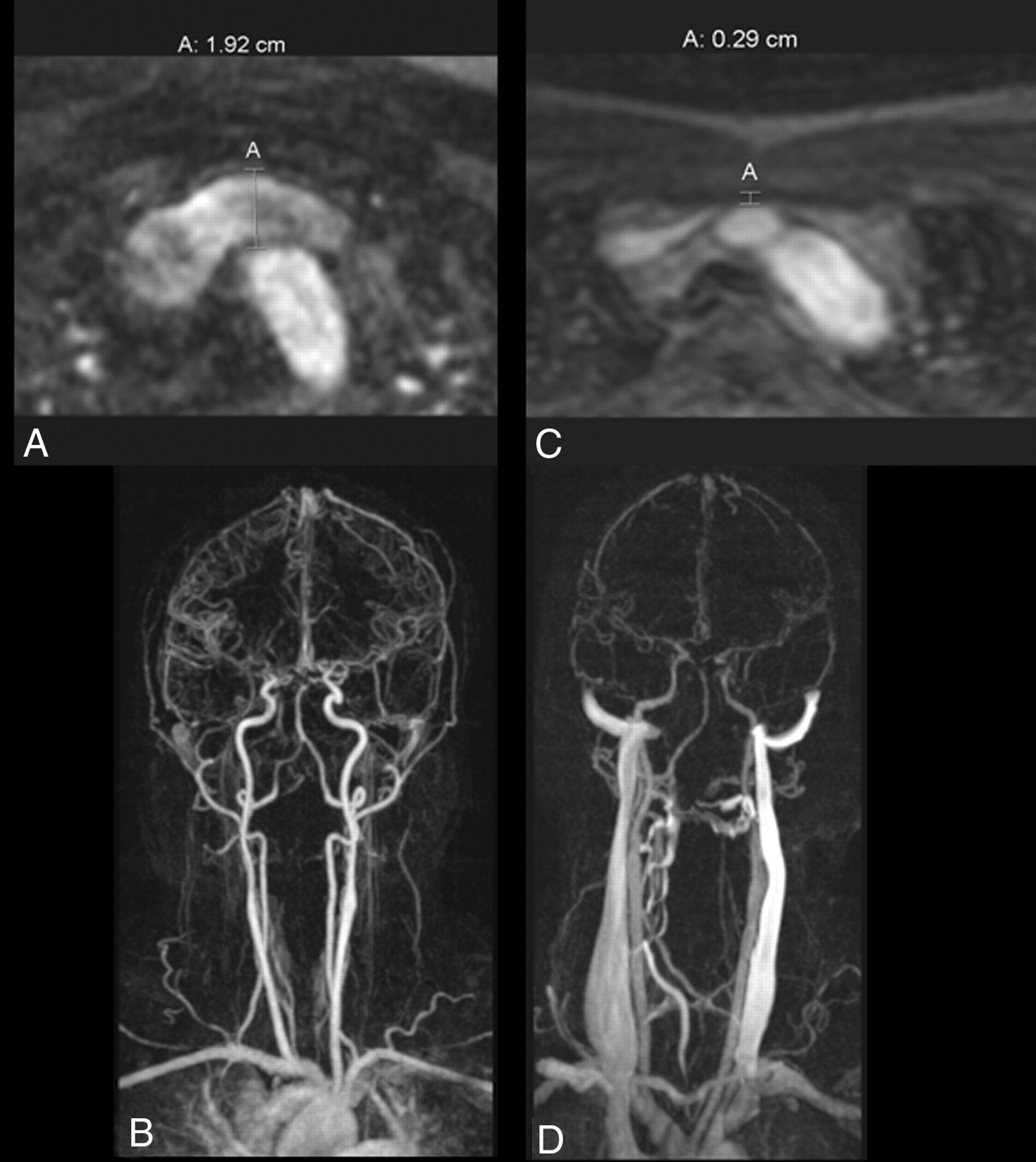
In the 57 patients with left antecubital vein injection and adequate angiograms, the anteroposterior distance between the sternum and the arch of aorta or its branches ranged from 5.8 to 20.2 mm, with an average of 12.1 ± 3.2 mm (95% confidence interval). In 8 patients with reflux, this distance ranged from 3.8 to 13 mm with an average of 7.2 ± 3.1 mm (95% confidence interval) (Figs 2 and 3). This difference in the mean distance in the 2 groups with and without reflux was statistically significant (P < .001).

Coronal reformatted images of MRA of 2 patients with left-sided injections. A, There is adequate retrosternal distance (19.2 mm) measured from the posterior cortex of the sternum to the anterior margin of the arch of the aorta. B, There is no venous reflux in this patient. C, In another patient, the retrosternal distance is decreased (2.9 mm) causing compression of the left brachiocephalic vein. D, This causes reflux of contrast and opacification of the venous system.

Boxplot shows the distribution of retrosternal space in patients without (0) and with reflux (1). The central line in the box represents the median distance and the upper and lower ends of the box represent the interquartile range. The whiskers at either end are the maximum and minimum values.
Five of 8 patients with reflux had poststenotic dilation of the brachiocephalic vein (Fig 4). Four (50%) of the patients with reflux and 32 (56.1%) without reflux of contrast had overlapping values of retrosternal distance (ie, between 5.8 and 13 mm). Furthermore, the visualized volume of refluxed contrast was measured, and quantification was attempted on the basis of the amount of opacification of jugular veins and perivertebral venous plexus. Patients with lesser retrosternal distances had more reflux. However, this classification was arbitrary, and the exact volume quantification was not possible because all the cases had reflux of contrast up to the base of the skull. The Table summarizes the relevant details of patients.

MRA MIP of a patient with reflux shows poststenotic dilation (white arrow).
Summary of patients with and without reflux
Discussion
Contrast-enhanced MRA is a noninvasive technique that provides high-resolution data in a reasonable timeframe. Use of faster acquisition techniques in an attempt to image the first pass of contrast material in the arterial vasculature potentially offers images without venous contamination.4 However, even with newer innovations to synchronize the image-acquisition time with the subject-dependent delay between the venous injection and the arrival of contrast bolus in the arteries, sometimes there is dilution or stasis of the contrast medium with poor opacification of the arterial system.
After injection into either antecubital vein, contrast medium flows through the ipsilateral brachiocephalic vein and then enters the right atrium via the superior vena cava. The neck arteries are opacified when a tight bolus of contrast medium reaches the arch of aorta and then proceeds forward. Any impedance to the venous return from the upper extremities will lead to stasis of contrast material and venous reflux into the internal jugular vein with technically inadequate MRAs.
This phenomenon of venous stasis and reflux has been described in all imaging studies that use intravenous contrast, including nuclear medicine studies,5,6 CT,7 and MR imaging.3 An explanation of the mechanism behind this had previously been provided in nuclear medicine studies.8 This obstruction to venous return occurs due to incorrect arm positioning,9 injection during breath-holding in inspiration (Valsalva maneuver), various mediastinal masses,10 superior vena cava syndrome, and congestive cardiac failure.8,11 None of these conditions were applicable to any of the patients included in our study.
MRAs with reflux had a significant relationship to injection via the left antecubital vein. The stasis of contrast media was noted at the level of the left brachiocephalic vein. This has previously been demonstrated in prospective studies by Lee et al3 and Tseng et al.12
Several factors may contribute to the higher incidence of venous reflux with left-sided injections. Anatomic factors like the course of the brachiocephalic veins and the angle at which they join the superior vena cava play an important role.13 The course of the right brachiocephalic vein is parallel to the arch of the aorta. In contrast, the left brachiocephalic vein travels anterior to both common carotid arteries and superior to the arch of aorta. Hence, it is prone to compression in the retrosternal space if these vessels become tortuous with age or long-standing hypertension.14 Obstruction of the left brachiocephalic vein leads to opacification of left jugular vein. The contralateral jugular vein is opacified by the epidural venous plexus or in severe cases via the dural sinuses.15
Tanaka et al16 have also proposed that asymmetric hyperintensity of the left sigmoid sinus and jugular vein on contrast-enhanced MRA is due to venous reflux as a result of compression of the left brachiocephalic vein between the aortic arch and the sternum.
In our study, there was no significant difference in the mean ages of patients with and without reflux (P = .069). This was also demonstrated by Tseng et al.12 However, while they concluded that dilation and tortuosity of these vessels did not contribute to this effect, we found a significant difference in the incidence of hypertension between these groups (P = .002), which typically leads to tortuous unfolded vessels. This was again confirmed by Lee et al.3
Compression of the left brachiocephalic vein could be thought of as the main cause of venous stasis and reflux as demonstrated by a statistically significant difference in the mean distance between the sternum and the arch of aorta in all patients with left-sided injections (P < .001). However, there was some overlap of this distance between patients with and without significant reflux. Tseng et al12 also found correlation between the volume of refluxed contrast and the retrosternal space in patients with left-sided injection. On repeating the study in 3 of our patients (2 with right antecubital vein injection and 1 via a central venous catheter), the “obstruction” in the retrosternal space was presumably bypassed and adequate opacification of the neck arterial system was obtained.
Another factor that may contribute to venous reflux is the presence of cardiac disease. We excluded all patients with congestive cardiac failure. There was no statistically significant difference in the incidence of cardiac disease between the patients with or without reflux (P = .102).
Quantification of the volume of reflux was attempted, but it was arbitrary because the veins were opacified almost up to the base of the skull in most cases. The limitation of this study is that we were unable to correlate the reduction in the retrosternal space with the volume of reflux and hypertension.
Conclusions
Compression of the left brachiocephalic vein between the sternum and tortuous aorta and proximal vessels aggravated by hypertension may lead to venous reflux that can degrade the quality of contrast-enhanced MRAs. Our study suggests that suboptimal contrast-enhanced MRA examinations can be avoided by the routine use of right-arm veins for contrast injection, especially in patients with hypertension.
Acknowledgments
We thank P. Sankara Sarma, PhD, and N.S. Vishwanath, MBBS, MPH scholar, Achutha Menon Centre for Health Science Studies, Sree Chitra Tirunal Institute for Medical Sciences and Technology, for their help in statistical analysis of this work.
Footnotes
B.T., D.R.H., and C.K. were responsible for the concept and design of the study; D.R.H., B.T., C.K., and T.R.K., for the analysis and interpretation of the results; and D.R.H. and B.T., for writing the article.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received July 6, 2010.
- Accepted after revision July 29, 2010.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.