
Abstract
BACKGROUND AND PURPOSE: Cement PE represents a potentially serious complication following vertebroplasty. To determine the frequency and extent of cement PE during percutaneous vertebroplasty, we performed a retrospective review of chest CT scans obtained in patients who had previously undergone ≥1 vertebroplasty procedure.
MATERIALS AND METHODS: After approval by our local institutional review board, we retrospectively evaluated 244 patients who had undergone vertebroplasty at 465 levels and subsequently underwent chest CT. A thoracic radiologist evaluated the presence, number, size, and location of discrete cement PEs. We catalogued the following data: age, sex, number of treated vertebrae, cement volume per vertebra, operator, presence of cement leakage noted by the operator during the procedure, and clinical presentation at postvertebroplasty CT.
RESULTS: At least 1 cement PE was detected in 23 (9.4%; 95% CI, 6%–13%) of 244 patients; 1 patient was symptomatic from a cement PE. The mean number of discrete cement PEs was 3.2 ± 3.4 (median, 2; range, 1–12). There was no correlation among the total number of treatment sessions, number of levels treated per session, cement volume per level, operator, or time between vertebroplasty and chest CT in the detection of cement PE. Those with PE were significantly younger (P = .0229) and had significantly more total levels treated (P = .0260). Cement PE was recognized by the operator during the vertebroplasty in 2 (8.7%) of 23 patients found to have it on CT.
CONCLUSIONS: Small asymptomatic cement PEs are common during vertebroplasty and usually are not recognized by the operator during the procedure.
Abbreviations
- CI
- confidence interval
- IV
- intravenous
- MIP
- maximum intensity projection
- PE
- pulmonary embolism
- PMMA
- polymethylmethacrylate
Percutaneous vertebroplasty is a widely applied treatment for symptomatic vertebral compression fractures. A potentially serious complication of vertebroplasty is the leakage of PMMA bone cement outside the vertebral body, which then leads to cement PE.1–4 To better define the incidence of PE associated with vertebroplasty, we performed a retrospective review of chest CT scans obtained in patients who had previously undergone ≥1 vertebroplasty procedure.
Materials and Methods
The study was approved by our local institutional review board. This retrospective study surveyed a data base of 1029 consecutive clinical patients, excluding those enrolled in prospective research trials, who had undergone a total of 1247 vertebroplasty procedures between February 4, 1999, and June 3, 2010. A number of previous case series from our institution have been published by using a portion of this same patient data base.5–28 However, we have neither previously performed a detailed analysis of the incidence of cement PE nor ever evaluated postprocedural chest CT findings in these patients. Among these 1029 patients, 250 (24%) subsequently underwent chest CT at our institution, usually for indications unrelated to the vertebroplasty. Six (2.4%) of these 250 patients underwent vertebroplasty outside our institution and were excluded, leaving 244 patients (23.7%) in the current study.
The chest CT technique varied depending on CT indication and date. CT examinations performed without IV contrast and those performed with only IV contrast were included. All examinations performed after April 2005 included 1.5-mm contiguous axial images. Before this date, the chest CT technique was not controlled for minimum section thickness. A single investigator performed a chart review of patient and procedural records to evaluate age, sex, number of treated vertebrae, cement volume per vertebra, operator, presence of cement leakage noted during the procedure by the operator, and presence or absence of pulmonary symptoms due to cement emboli. Operator-detected leakage was categorized as diskal, venous, paraspinal, and epidural.
A thoracic radiologist reviewed chest CT scans after each procedure to evaluate the presence, number, size, and location of cement PE in the pulmonary lobes on an independent diagnostic CT workstation in a darkened reading-room environment. Each CT series was viewed as a dynamic scrollable stack in multiple window/level settings, including standard soft-tissue, bone, lung, and a custom window/level setting designed to visualize high-attenuation barium-opacified PMMA in the presence of other IV contrast (approximately, window, 500; level, 450, adjusted manually for intravascular contrast intensity such that bright IV contrast was medium gray and PMMA was white). For each examination, axial 3D MIPs were used to maximize sensitivity to detect small emboli of PPMA, either MIPs produced routinely as part of the standard thoracic CT scan protocol (an approximately 15-mm-thick axial MIP slab reconstructed at 7-mm intervals) or those manually constructed on the independent workstation from the scan volume with the thinnest available set of images. In the case of patients who underwent multiple vertebroplasty procedures, chest CT performed after the final vertebroplasty session was reviewed.
Thirty-four (14%) patients had baseline chest CTs that were reviewed for comparison. We also assessed parenchymal changes associated with the cement emboli, and we noted any parenchymal changes adjacent or peripheral to the cement PEs. High-attenuation findings in the lungs were classified into 4 categories: certain (positive for cement PE), probable (likely cement but not definite), unlikely (most likely granuloma or other calcifications), and negative (high-attenuation structure in the lung confirmed not to be cement on the basis of historical comparisons). Calcifications smaller than the adjacent vessels associated with calcified lymph nodes in the expected drainage pattern, splenic/hepatic granulomas, or with typical clustered nodular densities were considered to be unlikely. For statistical comparisons, we defined the categories “certain” and “probable” as positive for cement PE, while categories “unlikely” and “negative” were considered negative for cement PE. Symptomatic patients were characterized as those presenting with respiratory symptoms within 30 days of vertebroplasty.
Percutaneous Vertebroplasty Technique
Details for typical vertebroplasty procedures at our institution have been published previously.17,18 Briefly, patients are usually treated under moderate sedation. Local anesthetic, consisting of subcutaneous 1% lidocaine and 0.25% bupivacaine, was placed into the deep soft tissues and periosteum with a 22-ga spinal needle. An 11- or 13-ga needle with an inner stylet was advanced under fluoroscopic guidance by using a transpedicular or parapedicular approach into the anterior one-third of the vertebral body in an attempt to reach the midline. Barium-opacified cement was typically infused under constant lateral fluoroscopy and intermittent anteroposterior fluoroscopy until it reached the posterior one-fourth of the vertebral body. The injection was terminated on observation of venous, epidural, paraspinal, or disk space extravasation. If the contralateral hemivertebral fill was inadequate, a second needle was placed into the contralateral side and additional cement was injected. The volume of cement used was recorded. Patients were instructed to remain supine for 2 hours postprocedure to allow hardening of the cement and resolution of sedation. Various cement mixtures without standardized PMMA-to-solvent ratios were used before July 2005. Since that time, Ava-Tex Radiopaque Bone Cement (Cardinal Health, Dublin, Ohio) has been used.
Statistics and Data Analysis
The frequency of the number and detection of cement PEs was analyzed as a proportion with 95% CIs. Patient age, total number of vertebroplasty sessions and levels treated, number of levels treated per session, cement volume per level, and time between vertebroplasty and CT were compared by using a t test. Operator-detected extraosseous leakage in patients with and without cement PE was compared by using a χ2 test.
Results
A total of 244 patients received treatment at 465 vertebral levels during 313 separate vertebroplasty sessions. Of these, 149 (61.1%) were women with a mean age of 71.4 ± 11.3 years; median, 73.9 years; range, 38.0–91.8 years. Ninety-five were men with a mean age of 68.2 ± 12.4 years; median, 71.0 years; range, 33.6–90.8 years. The age was listed at the time of the first vertebroplasty procedure. Eighty-two and eight-tenths percent (202/244) had 1 vertebroplasty session, 10.2% (25/244) had 2 vertebroplasty sessions, 5.3% (13/244) had 3 vertebroplasty sessions, and 1.6% (4/244) had ≥4 vertebroplasty sessions.
The average time between vertebroplasty and CT was 17.7 ± 21.1 months (median, 8.6 months; range, 0–99.4 months). Eighty-nine (36%) of 244 patients underwent CT for non-cement PE remote from the vertebroplasty, and 2 (0.8%) of 244 patients underwent CT specifically for cement PE. Other common indications were for chronic cough and shortness of breath, to evaluate pneumonitis or bronchiectasis, for metastatic cancer work-up, and to evaluate a pulmonary nodule or mass seen on chest radiographs. Non-IV contrast CT scans were available for review in 103 of 244 patients. The remaining 141 patients had only post-IV contrast images available.
Cement PEs were detected in 23 (9.4%; 95% CI, 6%–13%) of 244 patients. Of these, 87% (20/23) had certain cement PEs and 13% (3/23) had probable cement PEs. Fourteen of 23 patients (61%) underwent non-IV contrast CT, and 39% (9/23) had only post-IV contrast images available for review. One (4.3%; 95% CI, 0%–13%) of these 23 patients developed respiratory symptoms, manifested as mild dyspnea and left-sided pleuritic chest pain, which resolved gradually with conservative treatment. In this patient, who underwent a non-IV contrast CT, no parenchymal changes were visible. One asymptomatic patient (4.3%; 95% CI, 0%–13%) had parenchymal changes associated with the cement embolism visible on post-IV contrast CT.
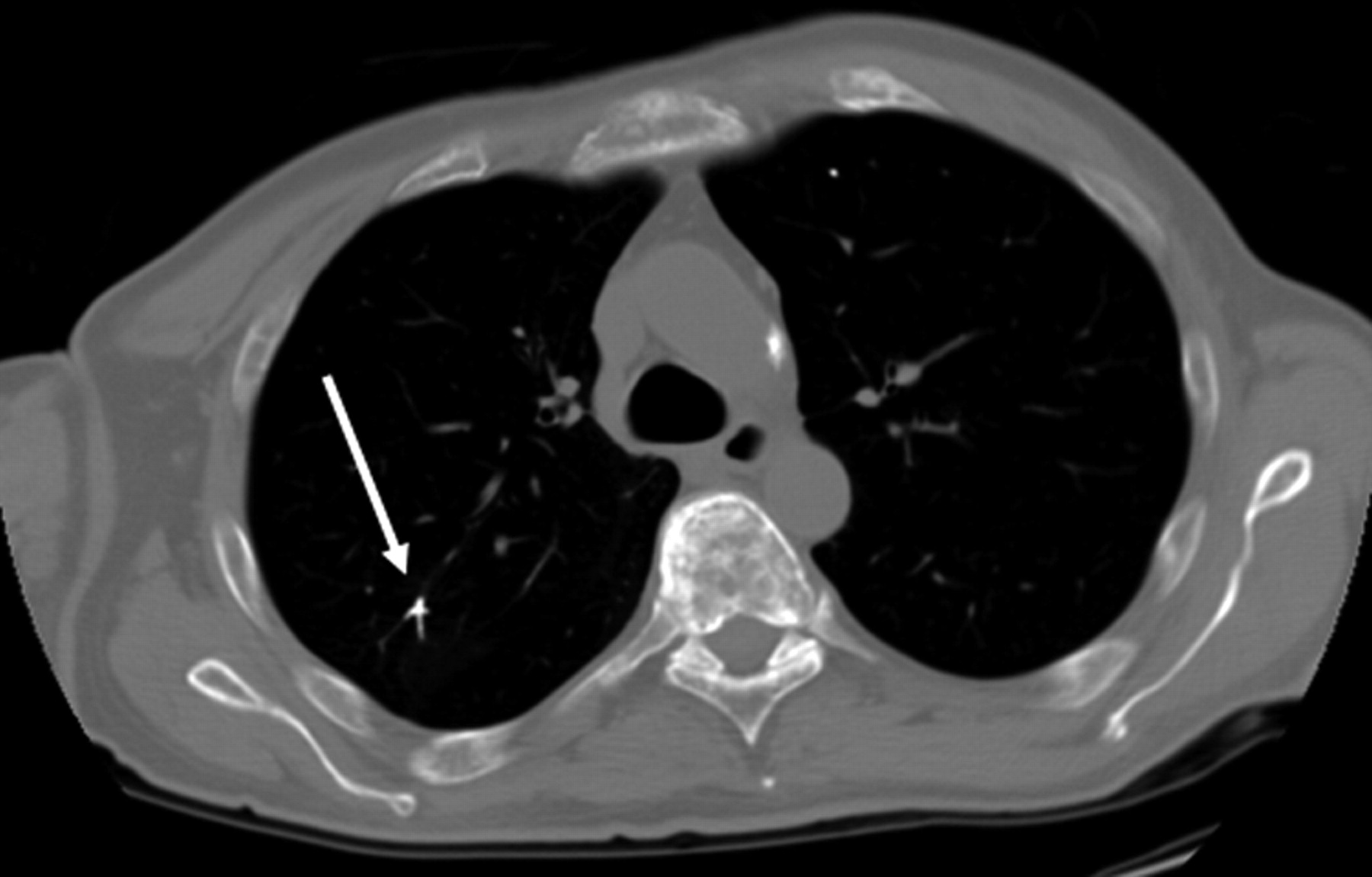
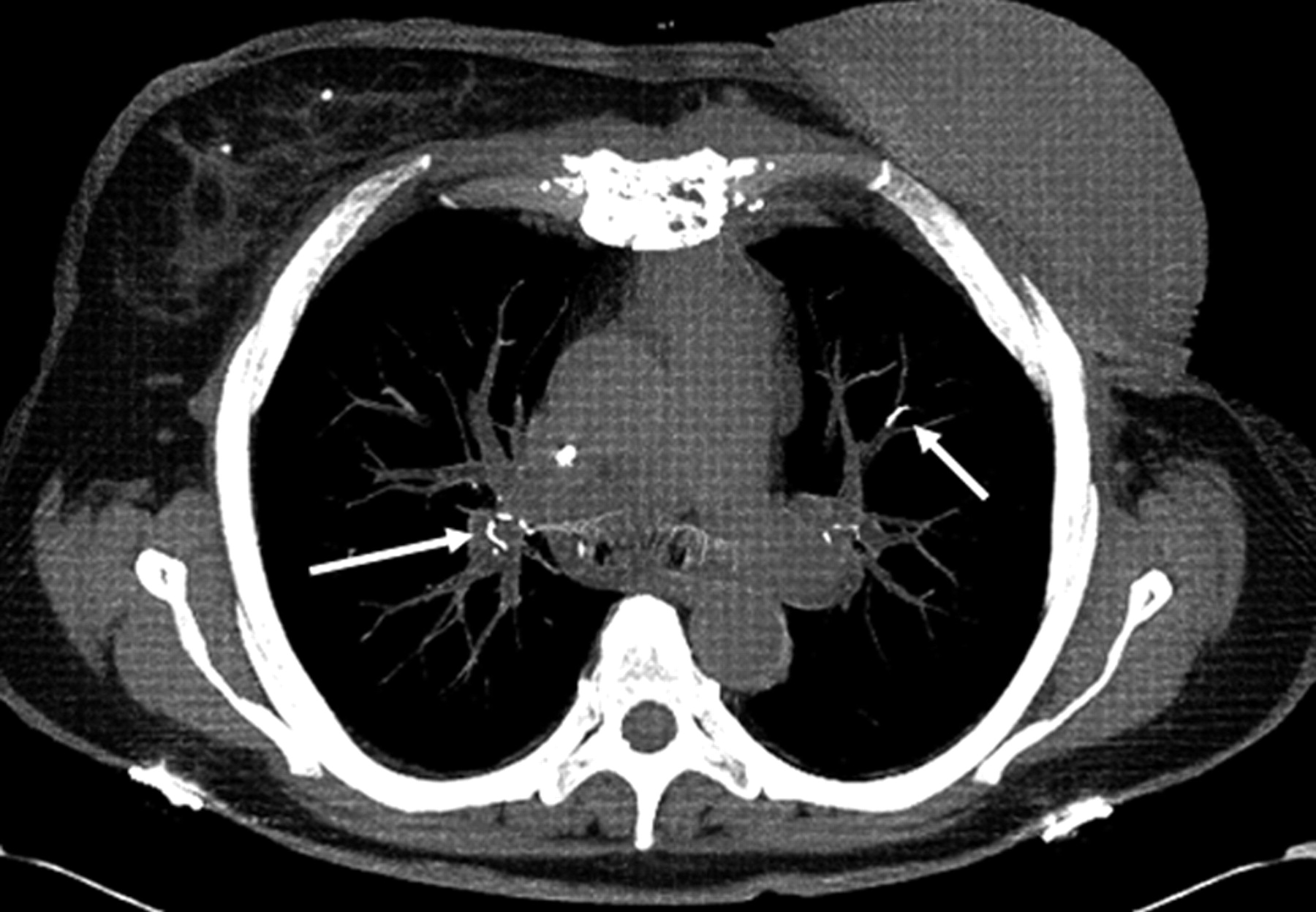
Among these 23 patients with cement PEs, the mean number of discrete emboli per patient was 3.2 ± 3.4 (median, 2; range, 1–12). Nine (39%) of 23 patients had a single embolus, 6 (26%) had 2, three (13%) had 3 emboli, and 5 (22%) patients had 4–12 emboli. Most emboli were tubular or branching (Figs 1 and 2). The mean length of emboli was 5.0 ± 4.4 mm (median, 4.0 mm; range, 1–21 mm). Cement PEs were scattered throughout both upper and lower lobes of both lungs.

A 68-year-old woman treated with vertebroplasty at T12. Axial unenhanced chest CT scan obtained 4 months following vertebroplasty demonstrates linear areas of markedly increased attenuation (arrows) within the pulmonary vasculature, indicating cement PEs.
A 52-year-old man treated with vertebroplasty at L1, L2, L4, and T12. Axial contrast-enhanced chest CT image obtained 6 days following the third vertebroplasty procedure demonstrates linear areas of markedly increased attenuation (arrow) within the pulmonary vasculature, indicating cement PE.
There was no significant difference in the etiology of compression fractures treated in patients with and without cement PEs (P = .19). Of those 221 patients negative for cement PE, 116 (52%) had osteoporosis, 43 (19%) had trauma, 32 (14%) had malignancies, 26 (12%) had multiple myelomas, and 4 (2%) had an unknown etiology. Among these 23 patients with cement PEs, 16 (70%) had osteoporosis, 3 (13%) had a malignancy, 3 (13%) had multiple myelomas, and 1 (4%) had trauma.
As listed in the Table, we detected no significant difference between patients with and without cement PEs regarding total number of vertebroplasty sessions, number of levels treated per session, cement volume per level, operator, or time between vertebroplasty and CT. Those with cement PE were significantly younger than those without (P = .0229). Patients with cement PE had significantly more total levels treated (P = .0260). There was a trend toward a lower amount of cement used per level in the patients with cement PE compared with those without cement PE.
Statistical comparison of patients with and without cement PE
Operators detected extraosseous cement leakage in less than one-half of the 23 patients with cement PE (Table); such leakage was detected almost as frequently among patients without cement PE. Cement migration to the lungs was noticed by the operator during the vertebroplasty in 2 (8.7%) of 23 patients later documented to have cement PE by chest CT. Cement PE was detected in only 17% (4/23) of patients on the initial reading of the CT scan.
Discussion
In the current study, we found, among a large cohort of patients undergoing vertebroplasty, a relatively high incidence of small asymptomatic cement PEs. Notably, operators identified migration of cement to the lungs during the vertebroplasty procedure in only a small minority of patients with cement PE. Indeed, operators failed to detect any type of extravertebral leakage in more than one-half of patients who had cement emboli. These findings suggest that even for practitioners highly experienced in vertebroplasty, cement PEs are not only common but are commonly unrecognized.
Previous studies have found the incidence of cement PE to range from 2.1% to 26%.1–4 As in the current study, patients in those other series typically remained asymptomatic. However, even small emboli may be lethal if they lodge in the right atrium or ventricle and cause cardiac perforation and cardiac tamponade rather than traveling to the pulmonary circulation. Linear pieces of cement as small as 10–20 mm long have been reported to cause cardiac tamponade,29 and pieces as small as 20 mm have been reported to cause perforations of the right ventricle.30–32 Thus, the observation of low rates of symptoms in our current series and other recent publications should not indicate that these frequent complications are necessarily benign.
Those with cement PE were significantly younger than those without, a finding for which we have no definitive explanation. As might be expected, patients with cement PE had significantly more total levels treated than patients without cement PE. There was a trend toward a lesser volume of cement used per level in the patients with cement PE. One explanation for this trend might be that extraosseous leakage would have led to early cessation of cement infusion, but most of the patients who had cement PE did not have leakage noted by the operator during the procedure.
Given the large variation in vertebroplasty cement mixtures available today, there may be a significant difference in rates of cement PE among various types. Studies comparing the types of cement may be useful.
Our study offers complementary and additive information to that of Kim et al4 in that we included nearly 4 times as many patients. However, being retrospective, this study had several limitations. There was some selection bias due to the fact that only a minority of patients subsequently had chest CTs. It may be presumed that those symptomatic patients would be more likely to undergo chest CT. Thus, cement PE may be over-represented in this population. Second, there was no uniform timeframe between vertebroplasty and CT. Nevertheless, the permanence of cement emboli allows variance in follow-up times. Many patients had multiple vertebroplasty procedures, and with 1 chest CT, it was not possible to detect during which session and in which levels the embolization occurred. We also could not control for chest CT technique, including image section thickness and administration of contrast. However, the focus of this article was not the relative accuracy of CT with and without contrast for cement PE detection but rather our best effort to determine, in a large series of patients, the approximate proportion of patients undergoing vertebroplasty who have cement PEs.
Conclusions
In this study, we found, among a large cohort of patients who underwent vertebroplasty, a high incidence of small asymptomatic cement PEs. In most cases, operators failed to identify extravertebral cement leakage during the procedure.
Acknowledgments
We thank Leigh A. Gray for advice regarding patient data collection and manuscript preparation.
References
- Received August 3, 2010.
- Accepted after revision September 14, 2010.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}