
Abstract
BACKGROUND AND PURPOSE: WM injury is associated with different disabilities that children born prematurely may experience during their lives. The aim of this study was to use TBSS to test the hypothesis that WM microstructure at TEA in preterm infants is correlated with cognitive and motor outcome at 2-year corrected age.
MATERIALS AND METHODS: Sixty-three preterm infants, born at a mean gestational age of 28.7 weeks, underwent MR imaging and DTI at TEA. Neurodevelopmental performance was assessed by using the BSITD-III. Voxelwise analysis of the DTI data was performed by using TBSS to assess the relationship among FA, AD, and RD at TEA, and cognitive, fine-motor, and gross-motor scores at 2-year corrected age.
RESULTS: Cognitive scores were correlated with FA values in the CC. Fine-motor scores were correlated with FA and RD throughout the WM. Gross-motor scores were associated with RD in the CC, fornix, and internal and external capsule.
CONCLUSIONS: WM microstructure in preterm infants at TEA was associated with cognitive, fine-motor, and gross-motor performance at 2-year corrected age. This study suggests that TBSS of DTI data at TEA has the potential to be used as a biomarker for subsequent neurodevelopment.
ABBREVIATIONS
- AD
- axial diffusion
- BSITD-III
- Bayley Scales of Infant and Toddler Development, Third edition
- CC
- corpus callosum
- FA
- fractional anisotropy
- FMRIB
- Functional MR Imaging of the Brain
- PLIC
- posterior limb of the internal capsule
- RD
- radial diffusion
- TBSS
- tract-based spatial statistics
- TEA
- term-equivalent age
- TFCE
- threshold-free cluster enhancement
With improvements in neonatal care, the mortality rate of preterm infants is decreasing. However, they remain at risk for neurodevelopmental impairments in later childhood.1,2 MR imaging is increasingly performed to assess brain damage in preterm infants. With the reduction in major focal lesions such as cystic periventricular leukomalacia, diffuse WM injury is now the most common abnormality observed on MR imaging.3
DTI is an MR imaging technique that may be used to assess WM development and injury.4 Image contrast in DTI is based on the Brownian motion of water molecules. In WM, water molecular motion is influenced by various factors (eg, axonal attenuation and degree of myelination).5 Water diffuses preferentially along WM fibers and is restricted across fiber bundles. Thus, the location and direction of cerebral WM tracts can be determined by assessing the preferential direction of water diffusion.6 Objective measures such as FA, AD (diffusion parallel to WM tracts) [λ1]; and RD (diffusion perpendicular to WM tracts [(λ2 + λ3) / 2]), can be derived from DTI and can provide information regarding WM microstructure. DTI studies of the preterm brain have shown that FA increases with age,7–10 which is mainly driven by a decrease in RD,11,12 and that FA is reduced and apparent diffusion coefficient values are increased in WM injury.13,14
TBSS is a recently developed observer-independent tool for analyzing DTI data.15 With TBSS, WM microstructural abnormalities have been identified in the absence of focal injury in the preterm brain at TEA.16 Additionally, Counsell et al17 demonstrated a relationship between FA in specific WM tracts and neurodevelopment, assessed by using the Griffiths Mental Developmental Scales, in children who were born preterm and studied at 2 years of age.
The aim of the present study was to test the hypothesis that WM microstructure, assessed by TBSS, in preterm infants at TEA is associated with neurodevelopmental performance at 2-year corrected age.
Materials and Methods
Patients
Neonates who were born before 31 weeks' gestation and reached TEA between January 2007 and July 2008 were recruited for a prospective preterm cohort study. Neonates with dysmorphic features or an infection of the central nervous system were excluded. Of the 174 consecutively admitted neonates, 22 died in the neonatal period, informed parental consent was not obtained for 14 neonates, and 15 neonates were not examined with our 3T system. MR imaging of the brain was performed around TEA. Written informed parental consent was obtained for all neonates, and this prospective study was approved by the medical ethics committee of our institution.
MR Imaging
MR imaging investigations were performed on a 3T MR imaging system (Achieva, Philips Medical Systems, Best, the Netherlands) by using an 8-channel phased-array SENSE head coil. The infants were sedated with 50–60 mg/kg of chloral hydrate orally, 15 minutes before the MR imaging. Heart rate, transcutaneous oxygen saturation, and respiratory rate were monitored during scanning (Nonin Pulse Oxymeter, Nonin Medical, Plymouth, Minnesota). For hearing protection, MiniMuffs (Natus Europe, Munich, Germany) were used. A neonatologist was present throughout the MR imaging examination.
The MR imaging protocol included sagittal T1-weighted (TR = 886 ms, TE = 15 ms, section thickness = 3.0 mm, number of sections = 31), axial 3D T1-weighted (TR = 9.4 ms, TE = 4.6 ms, section thickness = 2.0 mm, number of sections = 50), and axial T2-weighted imaging (TR = 6293 ms, TE = 120 ms, section thickness = 2.0 mm, number of sections = 50). WM injury was scored as reported previously.18
In 117/123 neonates, DTI was performed by using a single-shot echo-planar imaging sequence with diffusion gradients in 32 noncollinear directions (TR = 7745 ms, TE = 48 ms, voxel size = 1.41 × 1.41 × 2 mm, number of sections = 50, FOV = 180 mm; scan matrix = 128, foldover direction = anteroposterior, b-value = 800 s/mm2). In 6 infants, DTI was not performed due to time constraints. The quality of the DTI data and the derived FA maps were evaluated by 2 researchers. Data with artifacts arising from patient motion or technical errors in reconstruction were discarded; the resulting 66/117 (56.4%) neonates had DTI images eligible for further analysis.
Neurodevelopmental Assessment
At 2-year corrected age (mean 24.1 ± 0.3 months), the children were assessed with the BSITD-III by a single developmental specialist who was blinded to the MR imaging findings.19 Cognition and both fine- and gross-motor function were assessed. The language subtest was not assessed, due to the limited time children are able to concentrate during 1 session. Scaled scores of the 3 subtests and cognitive and total motor composite scores (ie, an overall score for fine- and gross-motor function) were calculated, corrected for prematurity (mean in a normative population: 10 ± 3 and 100 ± 15, respectively). Three of the 66 children were lost to follow-up; consequently, 63 neonates were included in this study.
Data Analysis
DTI data were analyzed with the FMRIB software library, Version 4.1.4 (www.fmrib.ox.ac.uk/fsl/fsl/downloading.html).20 The DTIs were registered to the b=0 image to minimize image artifacts due to eddy current distortions. The skull was removed from the images with the Brain Extraction Tool of FMRIB.21 FA, AD, and RD maps were calculated by using the Diffusion Toolbox in FMRIB. All subjects' FA images were aligned to a target in a common space by using an optimized TBSS protocol for neonates.22 Two linear registration steps were performed before nonlinear registration (6° df and 12° df), to register every subject's FA map to every other one. We selected the target with the minimum mean warp displacement score, and then each infant's FA map was aligned in target space. Following alignment to the target, a mean FA map was created.
A second set of registrations was then performed to register every individual FA map to the mean FA map. The aligned images were then used to create another mean FA map and a mean FA skeleton, which represented the centers of all tracts common to the group. This FA skeleton was thresholded at FA ≥ 0.15 to exclude peripheral tracts with high intersubject variability and/or partial volume effects with gray matter. Each subjects' aligned FA, AD, and RD data were projected onto this mean FA skeleton. Voxelwise cross-subject statistics was performed to assess the relationship between FA, AD, and RD and performance scores of the BSITD-III, corrected for gestational age and postmenstrual age at the time of the scanning. The results were corrected for multiple comparisons by controlling the family-wise error rate following TFCE.23
To visualize the relationship between local tissue abnormalities and neurodevelopmental performance scores, we generated regions of interest from areas that demonstrated a significant correlation with FA. Scores for cognitive, fine-motor, and gross-motor performance were plotted against FA, AD, and RD values in these regions (Figs 1–3). In all analyses, a P value < .05 was considered statistically significant.

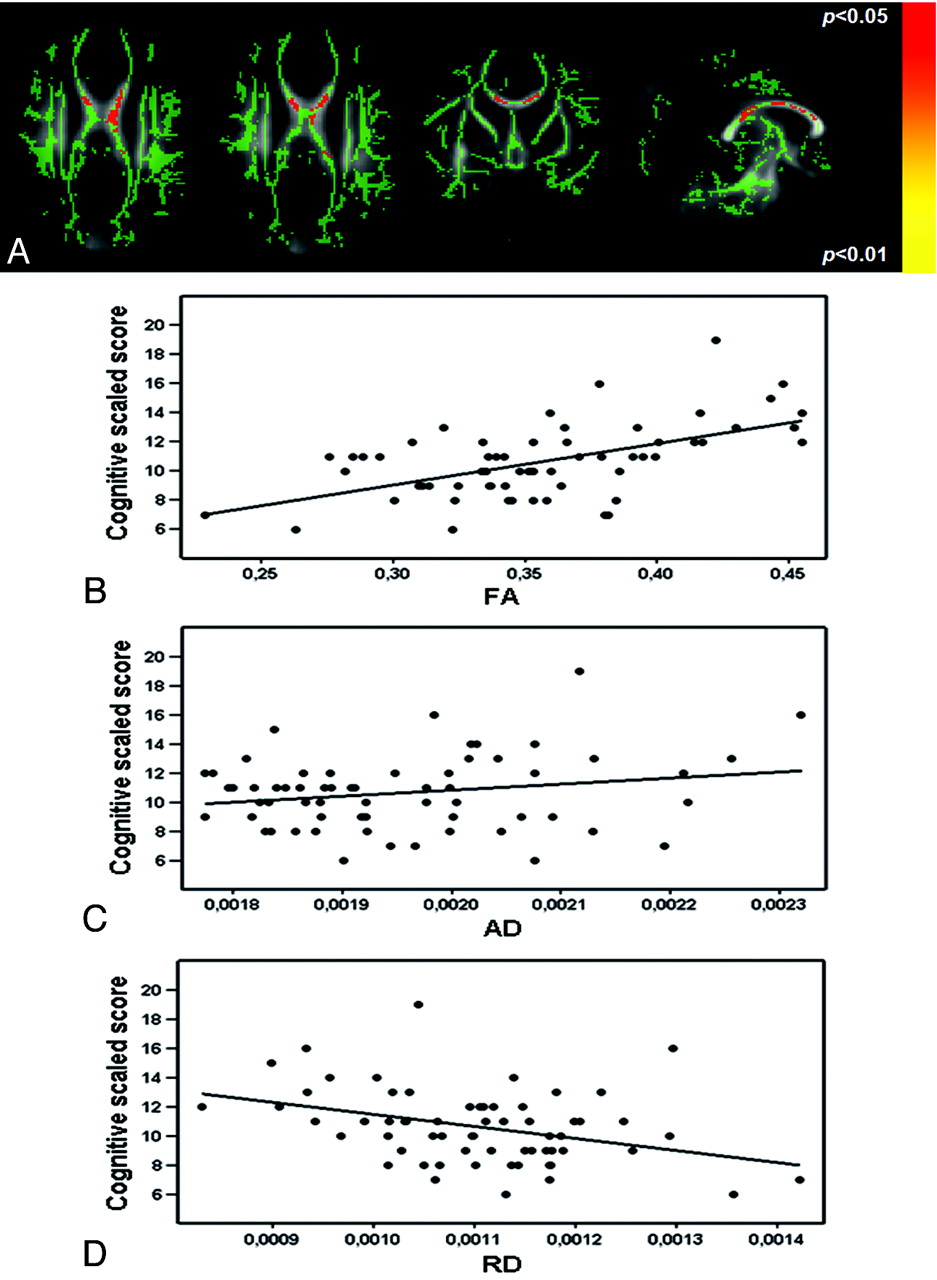
Diffusion parameters in relation to cognitive outcome. Mean FA skeleton (green) overlaid on the mean FA map in the axial, coronal, and sagittal planes. Regions of the mean FA skeleton in green voxels in which there is no correlation between FA and cognitive score. A, Voxels showing a significant correlation between FA and cognitive scores are shown in red-yellow. The graphs demonstrate the relationship between FA (R2 = 0.31, B), AD (R2 = 0.04, C), and RD (R2 = 0.13, D) and cognitive scaled scores from voxels in the CC (170 voxels), which showed a significant correlation between FA and cognitive score.
Results
Neonatal details are presented in Table 1. There were no differences in neonatal parameters between the infants included in this study and infants excluded due to the absence of DTI images (of adequate quality), though included infants tended to be older at birth (gestational age, 28.7 and 28.1 weeks, respectively; P = .054).
Characteristics of the neonates included in this study
MR Imaging Findings
During the neonatal period, 17 neonates were diagnosed as having an IVH on cranial sonography, and 3/17 developed posthemorrhagic ventricular dilation requiring treatment. On the basis of the WM scoring system of Woodward et al,18 54 (85.7%) neonates displayed normal or mildly abnormal WM and only 9 (14.3%) had moderately abnormal WM. No neonates had severe WM injury or cystic periventricular leukomalacia, though 1 neonate showed a small subcortical cyst frontally and 1 child had a cyst due to a hemorrhage in the temporal lobe.
Neurodevelopmental Outcome
Table 2 shows the results for the BSITD-III scores. Fine-motor scores were significantly higher than gross-motor scores (P < .001). No infant developed cerebral palsy or had other major motor deficits. Girls tended to have better cognitive scores than boys (P = .063; median scores 11 and 10, respectively). TBSS did not reveal significant differences in FA between females and males.
Cognitive and motor outcome on the BSITD-III at 2-year corrected age
WM Diffusion Parameters and Neurodevelopment
Cognitive Outcome.
Following TFCE correction for multiple comparisons, TBSS showed a positive relationship between FA values in the body and the splenium of the CC and the cognitive scores of the BSITD-III (Fig 1A). The relationship between FA values in the fornix and cognitive outcome just failed to reach significance (P = .051). No voxels showed a negative correlation between FA and cognitive score. There was no relation between cognition and AD or RD.
Mean FA, AD, and RD data were extracted from voxels in the CC, showing a significant relationship between FA and cognitive scores. The data were plotted in a graph to visualize the relationship between cognitive scores and FA (Fig 1B, R2 = 0.31), AD (Fig 1C, R2 = 0.04), and RD (Fig 1D, R2 = 0.13).
Fine-Motor Outcome.
FA was significantly correlated with fine-motor scores throughout the WM, with many regions significant at a threshold of P < .01. The significant regions included the whole CC, fornix, corona radiata, external capsule, corticospinal tract from the level of the PLIC to the cerebral peduncle, superior longitudinal fasciculus, inferior longitudinal and fronto-occipital fasciculi, cingulum, and uncinate fasciculus (all bilaterally, except for the uncinate fasciculus and the cingulum, which were only significant on the right side) (Fig 2A). No voxels showed a negative correlation between FA and fine-motor score. There was a significant negative relationship between RD in the PLIC on the right and the corticospinal tract from the level of the PLIC to the cerebral peduncle on the left. There was no relationship between fine-motor score and AD.
Mean FA, AD, and RD data were extracted from voxels in the left PLIC showing a significant relationship between FA and fine-motor outcome. The data were plotted in a graph to visualize the relation between FA (Fig 2B, R2 = 0.26), AD (Fig 2C, R2 = 0.04), and RD (Fig 2D, R2 = 0.28) and fine-motor score.

Diffusion parameters in relation to fine-motor scores. Mean FA skeleton (green) overlaid on the mean FA map in the axial, coronal, and sagittal planes. Regions of the mean FA skeleton in green represent voxels in which there is no correlation between FA and fine-motor score. A, Voxels showing a significant correlation between FA and fine-motor scores are in red-yellow. The graphs demonstrate the relationship between FA (R2 = 0.26, B), AD (R2 = 0.04, C), and RD (R2 = 0.28, D) and fine-motor scaled scores from voxels in the left PLIC (45 voxels), which showed a significant correlation between FA and fine-motor score.
Gross-Motor Outcome.
Gross-motor function was significantly correlated with FA values in the fornix, the left PLIC, and the thalamus. No voxels showed a negative correlation between FA and gross-motor score. RD displayed a significant negative relationship with gross-motor scores more extensively throughout the WM, including the fornix, CC (mainly left side), PLIC, and posterior part of the cingulum bilaterally (Fig 3A). There was no relation between gross-motor outcome and AD.
Mean FA, AD, and RD data were extracted from voxels in the left PLIC showing a significant relationship between FA and gross-motor scores. The data were plotted in a graph to visualize the relation between FA (Fig 3B, R2 = 0.26), AD (Fig 3C, R2 = 0.02), and RD (Fig 3D, R2 = 0.22) and gross-motor score.

Diffusion parameters in relation to gross-motor scores. Mean FA skeleton (green) overlaid on the mean FA map in the axial, coronal, and sagittal planes. Regions of the mean FA skeleton in green represent voxels where there was no correlation between FA and gross-motor score. A, Voxels showing a significant correlation between RD and gross-motor scores are in red-yellow. The graphs demonstrate the relationship between FA (R2 = 0.26, B), AD (R2 = 0.02, C), and RD (R2 = 0.22, D) and gross-motor scaled scores from voxels in the left PLIC (52 voxels), which showed a significant correlation between FA and gross-motor score.
Total Motor Scores.
There was a significant correlation between total motor score and FA values throughout the WM, and many WM regions were significant at a threshold of P < .01. The regions included the CC, fornix, corona radiata, external capsule, corticospinal tract from the level of the PLIC to the cerebral peduncle, superior longitudinal fasciculus, inferior longitudinal and fronto-occipital fasciculi, cingulum, and uncinate fasciculus bilaterally. No voxels showed a negative correlation between FA and total motor score. There was a significant negative relationship between total motor score and RD in the CC, fornix, left external capsule, left inferior longitudinal and fronto-occipital fasciculi, corticospinal tracts bilaterally, and the left uncinate fasciculus. There was no relationship between total motor outcome and AD.
Discussion
In this study, TBSS, optimized for the neonatal brain,22 was used for the first time at TEA in preterm infants born before 31 weeks' gestation to assess the relationship between diffusion parameters and neurodevelopmental performance at 2 years of age. TBSS provides an objective and reproducible voxelwise survey of cerebral WM, which reveals features that are consistent across a group of subjects, and avoids subjective selection of locations of interest or hypothesis-based selections of WM regions.15 Using this approach, we have shown that higher FA in the CC at TEA was associated with better cognitive performance. In addition, a widespread association was demonstrated between FA in the major WM tracts and fine-motor performance whereas gross-motor scores were associated with FA values in the PLIC, fornix, and thalamus. The findings for total motor scores were similar to those for fine-motor scores, suggesting that our results for the total motor scores were largely influenced by fine-motor performance and not by gross-motor abilities.
The increase in FA with respect to better BSITD-III scores observed here was mainly driven by a decrease in RD. The relationship between diffusion measures (eg, FA and RD) and underlying WM microstructure is complex. The increase in FA observed with increasing maturation is largely due to a decrease in RD.11,12 FA is largely dependent on axonal thickness, axonal attenuation, and myelination.24,25 The development of oligodendroglia precursors induces anisotropy in WM in a process primarily driven by changes in RD.26 At TEA, only the PLIC and the brain stem are myelinated,27 so the reduction in FA in association with subsequent poor neurodevelopment demonstrated here probably represents deficits or delays in premyelination events such as increasing axonal thickness, alterations in axonal permeability, and premyelination wrapping of the oligodendrocyte around the axon.28
We recognize that cognitive deficits are difficult to diagnose in early childhood and usually first become evident at school age.2 Nevertheless, our findings of altered WM microstructure in the CC and impaired cognitive ability are supported by previous studies that assessed callosal macrostructure and demonstrated that reduced callosal volume on conventional MR imaging was related to impaired cognitive development in children and adolescents born prematurely.29,30 Furthermore, Schmithorst et al31 observed a positive relationship between FA in association fibers and intelligence quotient in a healthy pediatric population, consistent with our findings of higher FA in association tracts and better neurocognitive performance.
Using a region-of-interest−based approach to assess DTI data, Rose et al32 examined FA in the anterior limb of the internal capsule, PLIC, and genu and splenium of the CC. They observed a relationship between FA in the PLIC at TEA and the psychomotor score of the BSITD-II at 18-month corrected age. Using TBSS to survey whole brain WM, we have shown that this relationship exists more extensively throughout the WM. The regions where we observed a positive correlation between fine-motor score and FA values were more extensive than those for gross-motor score. In addition to the PLIC and the corticospinal tracts, a correlation with FA was found in the association tracts, including the cingulum, fornix, uncinate fasciculus, and frontal WM.
The frontal lobes are involved in working memory, planning, monitoring, and organizing retrieval processes.33 The uncinate fasciculus provides a corticocortical link between the frontal and temporal lobes and is thought to be important in episodic memory.34 The cingulum is involved with high-order motor control and organization of motor-control processes.35 Lesions in this region are associated with deficits in working-memory performance,36 and reduced FA in the cingulum in schizophrenia is associated with attention and working-memory deficits.37 The fornix connects the hippocampus to the hypothalamus, and lesions in this structure are associated with memory and learning dysfunctions.38,39 These regions, therefore, are associated with working memory and manipulating information, processes that are assessed in the fine-motor component of the BSITD-III. In this study, we observed that better gross-motor function was related to a region of higher FA in the left PLIC, while decreased RD was correlated with gross-motor outcome in many regions throughout the brain. On examination of those voxels in the left PLIC showing a significant relationship between FA and gross-motor scores, we observed a strong positive correlation between AD and RD. These findings may explain the lack of association between FA and gross-motor scores, because an increase in both AD and RD could leave FA relatively unchanged.
Previous studies have used voxel-based approaches to assess the relationship between WM microstructure and performance in children who were born preterm. Skranes et al40 assessed adolescents born prematurely and age-matched term-born controls. They found lower FA in the internal and external capsules, CC, and the inferior and superior longitudinal fasciculi in the preterm group. Most important, lower FA in these areas was related to worse performance on the visual-motor integration and the Grooved Pegboard tests. At 2 years of age, subscores of the Griffiths Mental Developmental Scales were related to FA in the CC, cingulum, fornix, anterior commissure, and the right uncinate fasciculus.17 Our results suggest that the relationship between WM integrity and neurodevelopment, demonstrated by others in children born prematurely, is already evident at TEA.
We were able to analyze only 56% of the DTI data. DTI data are inherently sensitive to artifacts due to patient motion. Although the infants were sedated and noise reduction was administered, some infants woke up during the DTI sequence. In addition, some data were acquired with a sensitivity encoding factor of 3, which resulted in a lower signal intensity–to-noise ratio and visible artifacts across the brain, so these datasets were rejected. Nevertheless, our study group was relatively large, consisting of 63 infants with data amenable to analysis by using TBSS. This study used DTI data acquired at 3T, which offers a higher signal intensity–to-noise ratio and allows improved spatial resolution than could be achieved at lower field strengths. However, at the resolution achievable in vivo, the imaging voxels will inevitably contain fiber populations with different orientations, resulting in a reduction in the measured FA.
A further limitation of this approach is that TBSS is not always able to assess WM where there is an abrupt change in direction of the fiber pathway, for example at the junction of tracts.15 Finally, these findings were restricted to preterm infants, without the possibility to compare the results with healthy full-term controls. We accept that the lack of healthy term-born controls is a limitation of this study. However, previous studies have already shown differences between preterm infants at term and healthy term-born controls.9,16 Our aim here was to explore the relationship between WM injury and early neurodevelopmental performance in the preterm population.
Conclusions
An increase in FA and a decrease in RD in specific WM regions in preterm infants at TEA were related to cognitive, fine-motor, and gross-motor outcome at 2-year corrected age. These findings support the potential of diffusion parameters, obtained in preterm infants at TEA, as biomarkers for subsequent neurodevelopmental performance.
Acknowledgments
We are grateful to the families who took part in the study and to our colleagues of the neonatal intensive care unit and the MR imaging technicians for their expertise and enthusiastic help.
Footnotes
-
This work was supported by the Young Investigator Exchange Program Fellowship of the International Pediatric Research Foundation and the Netherlands Organization for Health Research and Development (project 94527022).
-
Paper previously presented at: 11th International Congress of the European Society of Magnetic Resonance in Neuropediatrics, March 24–26, 2011; Amsterdam, the Netherlands.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received March 23, 2011.
- Accepted after revision May 2, 2011.
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Brain 3T magnetic resonance imaging in neonates: features and incidental findings from a research cohort enriched for preterm birth
- Brain 3T magnetic resonance imaging in neonates: features and incidental findings from a research cohort enriched for preterm birth
- Early structural connectivity within the sensorimotor network: deviations related to prematurity and association to neurodevelopmental outcome
- Diffusion MRI Microstructural Abnormalities at Term-Equivalent Age Are Associated with Neurodevelopmental Outcomes at 3 Years of Age in Very Preterm Infants
- Lipid Intake and Neurodevelopment in Preterm Infants
- Regional brain volumes, microstructure and neurodevelopment in moderate-late preterm children
- "Integrative genomics study of microglial transcriptome reveals effect of DLG4 (PSD95) on white matter in preterm infants"
- Machine learning shows association between genetic variability in PPARG and cerebral connectivity in preterm infants
- Microstructure of the Default Mode Network in Preterm Infants
- Tract-Based Spatial Statistics in Preterm-Born Neonates Predicts Cognitive and Motor Outcomes at 18 Months
- Optimal Timing of Cerebral MRI in Preterm Infants to Predict Long-Term Neurodevelopmental Outcome: A Systematic Review
- Role of Diffusion Tensor Imaging as an Independent Predictor of Cognitive and Language Development in Extremely Low-Birth-Weight Infants
- Abnormal brain maturation in preterm neonates associated with adverse developmental outcomes
- Predictive Value of Neonatal Magnetic Resonance Imaging in Preterm Infants
- Acquisition Guidelines and Quality Assessment Tools for Analyzing Neonatal Diffusion Tensor MRI Data