
Abstract
SUMMARY: We present a patient undergoing spinal angiography and suspected of having an AVM. During the first injection of nonionic contrast, a nidal AVM supplied by the great anterior radiculomedullary artery at T9 left was found. The second injection at T9 left no longer showed the contrast filling of the AVM. Follow-up angiography showed persistent AVM obliteration with an intact arterial spinal axis. The patient's symptoms resolved. Interaction between nonionic contrast, blood, and vessel wall most likely induced the obliteration.
Abbreviations
- AVM
- arteriovenous malformation
AVMs of the spinal cord are rare congenital vascular disorders characterized by a perimedullary fistula or an intramedullary nidus. The feeding vessels arise from the anterior or posterior spinal arteries with drainage into the perimedullary venous plexus. Spinal AVMs most often present in young adulthood with symptoms of myelopathy or acute neurologic deterioration secondary to intramedullary or subarachnoid hemorrhage. The presence of a spinal AVM is readily diagnosed with MR imaging. Spinal angiography is needed to evaluate the angioarchitecture for treatment planning. Treatment can be endovascular or surgical; both methods carry a serious risk of occluding normal vessels to the cord with consequent ischemic damage and neurologic deficit.1 Spontaneous closure of spinal AVMs has occasionally been described.1–3 We present a case of a spinal AVM that was obliterated during angiography.
Case Report
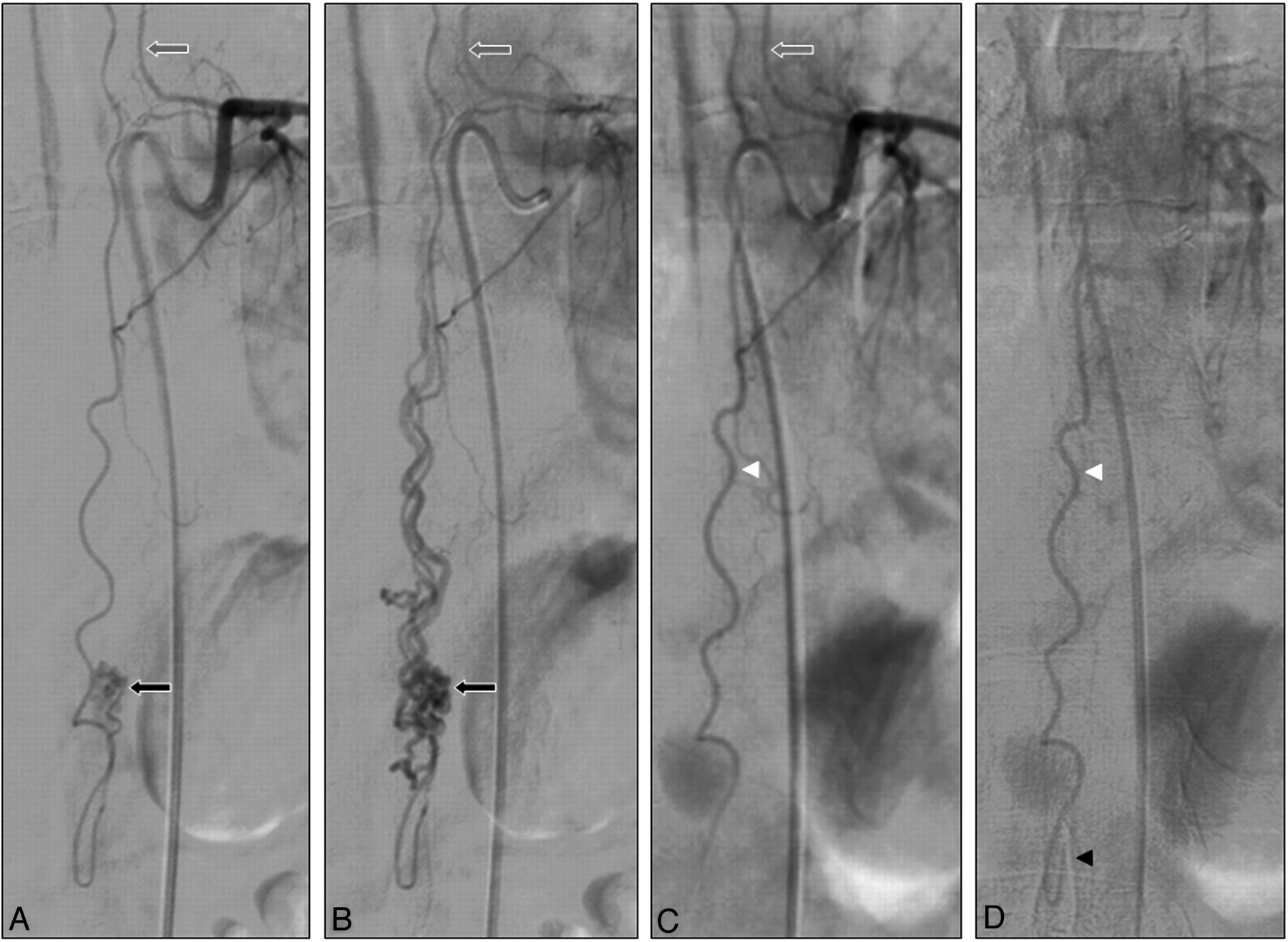
A 35-year-old man presented with painful sensations along his right buttock and thigh. Spinal MR imaging demonstrated a small AVM posteriorly located in the cone with dilated perimedullary draining veins. There were no signs of myelopathy or previous hemorrhages (Fig 1A, -B). Spinal angiography with use of a nonionic contrast agent (Iohexol, Omnipaque 300; GE Healthcare, Eindhoven, the Netherlands) confirmed the presence of the AVM (Fig 2A, -B), with the anterior spinal artery arising from the intercostal artery at T9 left as a single feeder to the nidus; the adjacent intercostal and lumbar arteries did not supply the AVM. The anterior spinal artery coursed under the distal part of the conus to supply the posteriorly located AVM nidus. Most surprising, during the second selective injection at the same pedicle, slow flow in the anterior spinal artery was noticed without visualization of the nidus (Fig 2C, -D). Also injections 10–15 minutes later and additional injections in the adjacent segmental arteries failed to allow visualization of the AVM. The procedure was terminated. In the following days, the patient's symptoms gradually improved, and he was discharged home. Three months later all symptoms had resolved. Follow-up MR imaging and MR angiography4,5 at 3 and 6 months and spinal angiography at 3 months confirmed the lasting complete obliteration of the spinal AVM with an intact anterior spinal axis (Fig 3A−D).

A and B, Sagittal T2-weighted MR images showing tortuous enlarged perimedullary and radicular veins (white arrows) and the posteriorly located AVM nidus (black arrow, B).

A and B, Spinal angiograms showing the great anterior radiculomedullary artery at T9 left (gray arrow) supplying the AVM in the arterial (A) and venous (B) phase. Note that the anterior spinal artery runs all the way down and around the conus to supply the posteriorly located AVM (black arrow). C and D, Later injections at the same pedicle show no contrast filling of the AVM in the arterial (C) and venous phase (D) and a patent anterior spinal artery (white arrowhead), which runs around the conus (black arrowhead, D).

A and B, Pre- (A) and postangiography (B) T2-weighted MR images showing complete disappearance of the tortuous enlarged veins and a small remnant of the AVM (black arrow, B). C, High-resolution MR angiogram demonstrates the radiculomedullary artery at T9 left (gray arrow) with a patent anterior spinal artery (white arrowhead). D, Spinal angiogram confirms persistent obliteration of the AVM with a patent anterior spinal artery (white arrowhead).
Discussion
Spontaneous obliteration of central nervous system AVMs has occasionally been described.6–8 Most of these cases were cerebral AVMs that thrombosed after symptomatic intracerebral or subarachnoid hemorrhage. This spontaneous thrombosis of a cerebral AVM may be explained by reduction of blood flow as a result of compression on the proximal draining veins by the hematoma or edema, feeding artery occlusion through vasospasm, thromboembolism, or systemic coagulation disorders.9
Spontaneous obliteration of spinal AVMs has been described in only 3 cases. One spinal AVM at the T11–12 level thrombosed after hemorrhage. However, in this case, a previous angiogram was not available and surgical exploration was not performed.2 The second case involved complete thrombosis of a perimedullary spinal cord AVM at the T11-L1 level. The thrombosis probably occurred soon after diagnostic angiography and was associated with neurologic deterioration. MR imaging and angiography performed 1 week later revealed complete occlusion of the lesion. Thrombosis of the dominant draining vein triggered by contrast injection was believed to be the most probable cause of the observed phenomenon.9 The third case was an angiographically confirmed spinal AVM at the T12-L1 level that was left untreated. The patient returned 3 years later with sudden paraparesis and bladder retention. Repeat angiography demonstrated complete thrombosis of the AVM, also at follow-up. The patient did not recover completely. It was thought that thrombosis of the draining veins, triggered by the interaction of genetic and hemodynamic factors, was the most probable cause.1
Obliteration during angiography with confirmation 3 months later, as in our case, has not been described previously, to our knowledge. The mechanism that led to thrombosis of the AVM remains unclear. Possible mechanical explanations are thromboembolism, dissection of the vessel wall, and vessel spasm. However, in our case, dissection of the vessel wall or vasospasm did not occur, and there were no thrombi visualized on the angiogram. Nonionic contrast agents, as used in our patient, can induce coagulation via activation of platelets, aggregation of red blood cells, changes in the endothelium, and changes of the osmolality and ionic strength.3,10 We believe this toxic effect of the contrast agent is the most likely explanation for the acute thrombosis. The patient's symptoms resolved soon after obliteration of the AVM, unlike in the 2 previously documented cases. Apparently, the thrombosis of the AVM remained restricted to the nidus itself with unaffected patency of the anterior spinal axis.
It is suggested that spontaneously thrombosed AVMs may recanalize and that follow-up angiographic evaluation is recommended, preferably after 2 months or later.7 We performed follow-up angiography at 3 and 6 months, which showed persistent complete occlusion of the AVM by both MR and conventional angiography.
References
- Received September 1, 2010.
- Accepted after revision October 15, 2010.
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.