
Abstract
BACKGROUND AND PURPOSE: Computed tomography is an essential modality for imaging of the temporal bone. Newest generation scanners allow the coverage of large examination volumes with a single gantry rotation. The objective of this study was to compare a 128-section SST (1 single rotation of the x-ray tube) with conventional spiral MSCT (ultra-high-resolution mode) for imaging of the temporal bone.
MATERIALS AND METHODS: Fifty-four temporal bones in 27 patients were scanned with both a conventional MSCT and 128-section SST. After blinding and randomization of both examinations, 2 observers assessed the visualization of 38 anatomic structures (eg, various segments of the facial nerve canal, mallear ligaments) by using multiplanar reconstructions in the axial and coronal planes. The differences in evaluation scores obtained for the 2 techniques were analyzed by using a Wilcoxon signed rank test, with a P value of < .05 considered significant. For both methods, imaging time and radiation exposure were noted.
RESULTS: Overall visualization of anatomic structures did not differ significantly between the 2 techniques (P > .05). When we compared the anatomic structures separately, there was better visualization of the lateral mallear ligament with MSCT, whereas the cochlear septa were ranked higher with SST (P < .05). Imaging time and average DLP for MSCT were 12.3 seconds and 306 mGy cm, respectively; for SST, values they were 1 second and 64 mGy cm, respectively (ie, a dose reduction of 79%).
CONCLUSIONS: For imaging of the temporal bone with adequate diagnostic quality, 128-section SST can be used. The main advantages over MSCT are the dramatic reductions of imaging time and radiation exposure, which are particularly important when scanning uncooperative patients or children.
ABBREVIATIONS:
- CTDIvol
- CT dose index
- DLP
- dose-length product
- MPR
- multiplanar reformations
- MSCT
- multisection CT
- SST
- single-shot technique
CT is an essential method for imaging of the temporal bone.1⇓⇓–4 Ongoing developments in CT led to a steady rise in the number of detectors (multidetector CT) and, therefore, an increase in examination volume within 1 rotation of the x-ray tube. The latest generation of scanners allows coverage of whole organs with a single gantry rotation.5 The major advantage is a dramatic reduction of motion artifacts and radiation exposure.
The aim of this study was to evaluate a 128-section SST, in which the whole temporal bone can be covered with a single tube rotation, and to compare this with conventional spiral MSCT in terms of image quality, examination time, and radiation exposure.
Materials and Methods
Patients
From February 2008 to March 2009, 27 patients (16 men, 11 women) referred to the department of radiology for CT of suspected inflammation or tumors of the temporal bone were included in the study after they gave their written informed consent. Ages ranged from 33 to 84 years (mean, 51 years). Only patients not suitable for MR imaging were included. The study was conducted under an institutional review board–approved protocol.
Imaging Technique
All examinations were performed on a 128-section CT system (Somatom Definition AS+; Siemens Healthcare, Erlangen, Germany). All included patients underwent our standard unenhanced MSCT, followed by SST after intravenous injection of iodinated contrast media (Imeron 350 mg/ml; Bracco Altana Pharma, Konstanz, Germany). MSCT of the temporal bone is routinely performed in the ultra-high-resolution mode, using a special grid in front of the detector array to increase spatial resolution. The data of SST were acquired within a single rotation of the x-ray tube, by using 128 sections with a total volume coverage of 38.4 mm. Technical details for both MSCT and SST are given in Table 1.
Technical details for MSCT and SST
Both imaging time and dose (DLP, CTDIvol) were compared between the 2 techniques.
Image Evaluation
The examinations were reviewed on a dedicated CT workstation (syngo Multimodality Workplace, Siemens Healthcare) by using MPRs in the axial and coronal planes. Because the image thickness of MSCT was 0.4 mm and of SST was 0.75 mm, all examinations were evaluated at a constant MPR thickness of 0.8 mm; windowing was 4000 HU at a center of 700 HU. A board-certified radiologist (S.A.S.) with >5 years of experience in imaging of the temporal bone and a resident (S.E.) evaluated the examinations after blinding and random ordering in a consensus reading. Before the actual evaluations, both S.A.S. and S.E. trained for the assessment process by using dedicated literature about the CT anatomy of the temporal bone.6 The training cases were not included in the study.
For the evaluation of the CT images of the temporal bone, 38 anatomic structures were chosen (Table 2), in accordance with previously published studies.1,2,4,7
Evaluated anatomic structures of the temporal bone
The assessment of each anatomic structure was performed by using the following scale: 1 = not visible because of insufficient image quality, 2 = visible but not diagnostic, 3 = visible and diagnostic.1 Structures that were not detectable because of disease or surgery were classified as 4 (Table 3) and were excluded from statistical analysis as “missing data.”
Score scheme for the assessment of the detectability of each anatomic structure
Statistics
The difference in the visibility of the defined anatomic structures in MSCT and SST was compared by using a Wilcoxon signed rank test; a P value <.05 was considered significant. A normal distribution was excluded by using the Kolmogorov-Smirnov test (P < .05). Bonferroni correction was applied to compensate for effects of multiple testing. All statistical analyses were performed by using dedicated software, the Statistical Package for the Social Sciences, Version 14.0 (SPSS, Chicago, Illinois).
Results
Fifty-four temporal bones from 27 patients scanned with both SST and MSCT were evaluated by the readers. Category 4 (not detectable because of disease or surgery, 3.3% of the entire dataset) was excluded from statistical analysis as missing data. No SST was degraded by motion artifacts.
Overall visualization of the 38 anatomic structures did not differ significantly between SST and MSCT (P < .05) (Figs 1⇓–3). Thereafter, a Wilcoxon signed rank test in combination with a Bonferroni correction was applied to compare the visualization of each particular structure with both techniques (Table 4).

Temporal bone axial MPR, section thickness 0.8 mm, in both SST (A) and MSCT (B). The anterior mallear ligament (1), malleus head (2), incus body (3), and incudomallear articulation (4) can be seen clearly with both imaging techniques.

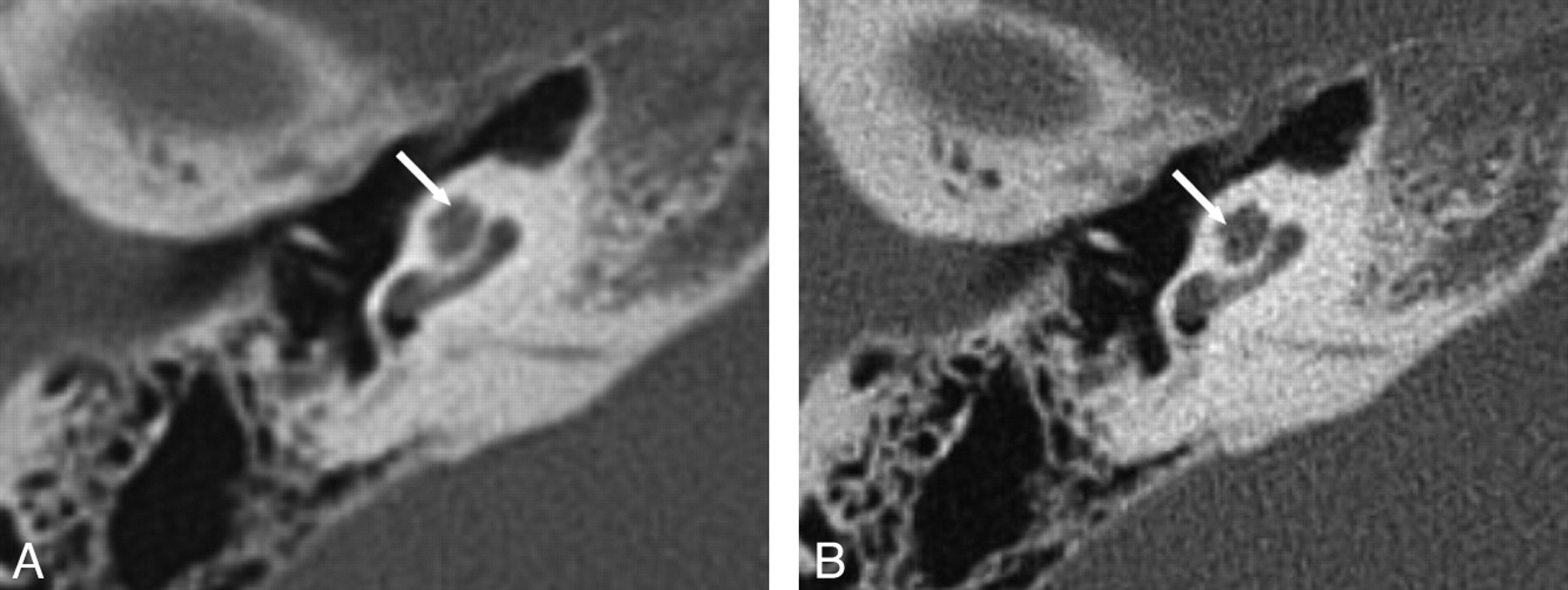
Temporal bone axial MPR, section thickness 0.8 mm, in both SST (A) and MSCT (B). The stapes crura (arrow) can be seen clearly with both imaging techniques.

Facial nerve canal axial MPR, section thickness 0.8 mm, in both SST (A) and MSCT (B). The geniculate ganglion (1), labyrinthine segment (2), and the tympanic segment (3) of the facial nerve can be seen in diagnostic quality with both imaging techniques. Note the status postmastoidectomy.
Difference between methods
After the Bonferroni correction, a significant difference was found between SST and MSCT for the lateral mallear ligament (Fig 4) and the bony septum between the upper and middle turn of the cochlea (Fig 5). The former was seen more clearly with MSCT, whereas the latter was seen better with SST.

Temporal bone coronal MPR, section thickness 0.8 mm. The lateral mallear ligament can hardly be seen with SST (A), whereas it is clearly shown with MSCT (B).

Temporal bone axial MPR, section thickness 0.8 mm. The bony septum between the apical and middle turn of the cochlea (arrows) can be seen more clearly with SST (A) than with MSCT (B), where it can hardly be found.
Radiation Dose and Imaging Time
The average CTDIvol was 50.3 mGy for MSCT and 16.8 mGy for SST. The average DLP was 306 mGy cm for MSCT and 64 mGy cm for SST.
Imaging time was 12.29 seconds for MSCT and 1 second for SST.
Discussion
High-resolution MR imaging and MSCT are the preferred tools for imaging the temporal bone. While high-resolution MR imaging has the advantage of excellent soft-tissue resolution, high-spatial-resolution MSCT is better at visualizing the delicate osseous structures and, thus, is the basis for the diagnosis of developmental anomalies, traumas, acute or chronic infections, and masses.1⇓⇓–4 Although the scanning time with modern MSCT scanners is short, especially in contrast to MR imaging, the patient must still remain motionless during the image acquisition, which can be a problem in uncooperative patients or children. Another disadvantage of MSCT is that it exposes patients to rather high levels of ionizing radiation.
With the introduction of wider detector arrays, the SST (in which only 1 rotation of the tube-detector system is performed for data acquisition) became feasible for imaging whole-organ systems (eg, the heart or brain) or anatomic regions such as the temporal bone. The SST data in this study were acquired by using a 128-section MSCT system with a total volume coverage of 38.4 mm. Because the whole temporal bone is scanned with a single gantry rotation, imaging times of ≤1 second can be achieved. Therefore, even moderately cooperative patients could be examined with SST. Moreover, with our SST protocol, a dramatic decrease in radiation exposure could be achieved. As a negative effect, the higher section thickness of our SST resulted in an inferior resolution of the sections compared with MSCT, which was performed in the ultra-high-resolution mode using a special grid in front of the detector array to reduce section thicknesses to 0.4 mm.
The aim of this study was to compare SST with MSCT to determine whether a compromise in the resolution of the SST would result in a reduced diagnostic value.
Although SST subjectively resulted in examinations that had less “sharp” images than MSCT using the ultra high resolution grid, the statistical comparison revealed no significant difference in the overall judgment of diagnostic image quality, whereas the separate evaluation showed a significant difference in 2 of 38 structures (5%).
The bony septum between the apical and middle turn of the cochlea could be judged significantly better with SST. The integrity of the latter together with, for example, the entire cochlear morphology is of special importance in the preoperative assessment of the inner ear before cochlear implantation8⇓–10 or for the diagnosis of labyrinthitis ossificans.11 Using SST could be an advantage in these patients.
The second anatomic structure that showed a significant difference between SST and MSCT was the lateral mallear ligament, which was imaged more clearly with MSCT. Because either fixation or detachment of the mallear ligaments may lead to impaired transduction of acoustic stimuli, a proper visualization of these delicate anatomic structures is necessary12 and can be achieved with high-resolution CT.13 Therefore, on the basis of our data, we recommend imaging of the mallear ligaments with MSCT rather than SST.
One major advantage of SST is its significantly shorter time of image acquisition. Our SST protocol took only 1 second compared with a duration of 12.29 seconds in our MSCT protocol. This decrease in imaging time of 92% could be of particular use in uncooperative persons and children, who sometimes have to undergo sedation or general anesthesia with all its drawbacks and risks.14,15 On the other hand, moving artifacts may theoretically lead to repetitive scans, which means additional radiation exposure.
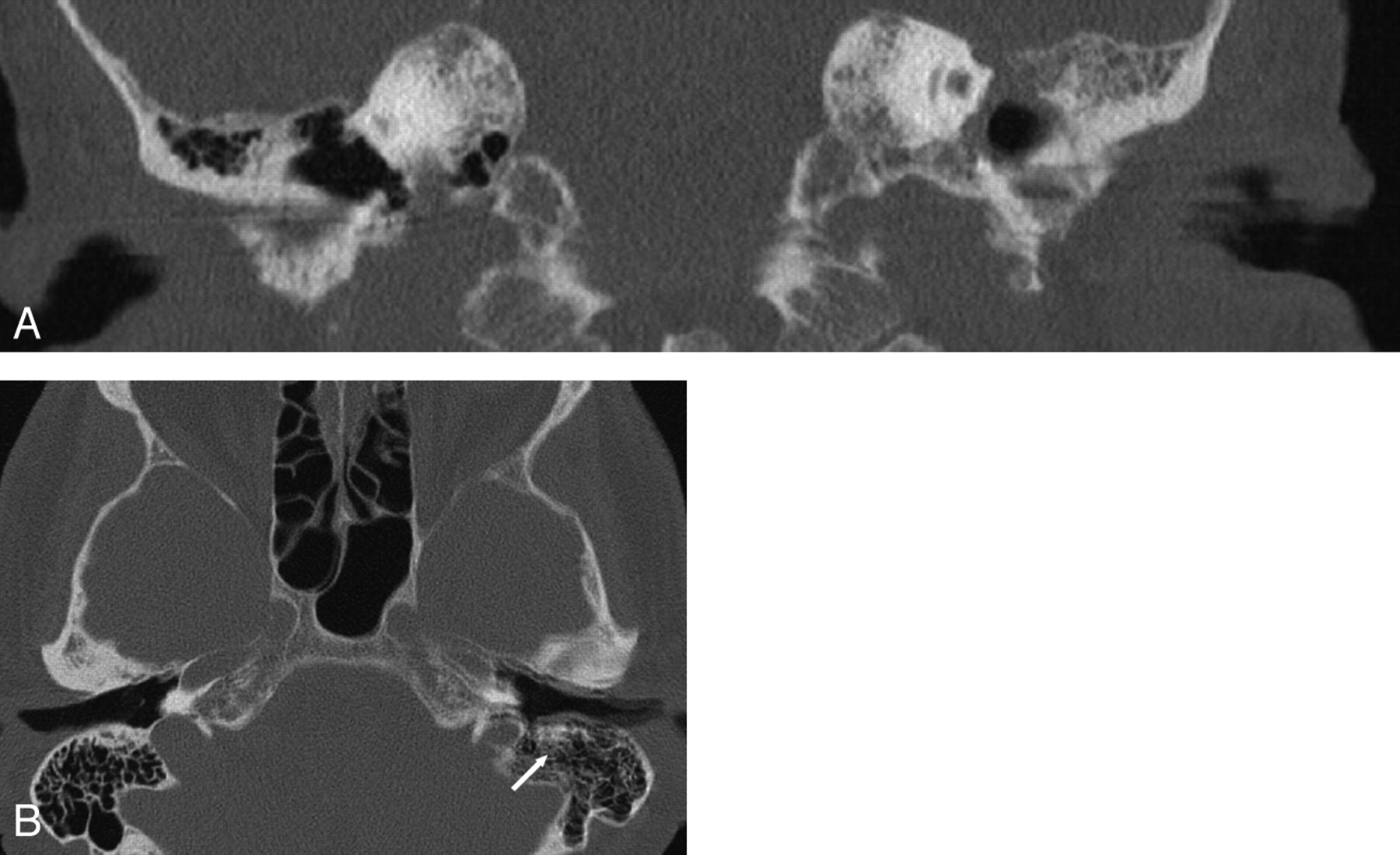
The evaluation of our examinations showed no moving artifacts in the SST scans, whereas the image quality of MSCT was decreased due to patients' moving in 2 cases (Fig 6). Nevertheless, in both cases, image quality was sufficient to establish a diagnosis; thus, the examinations did not need to be repeated.
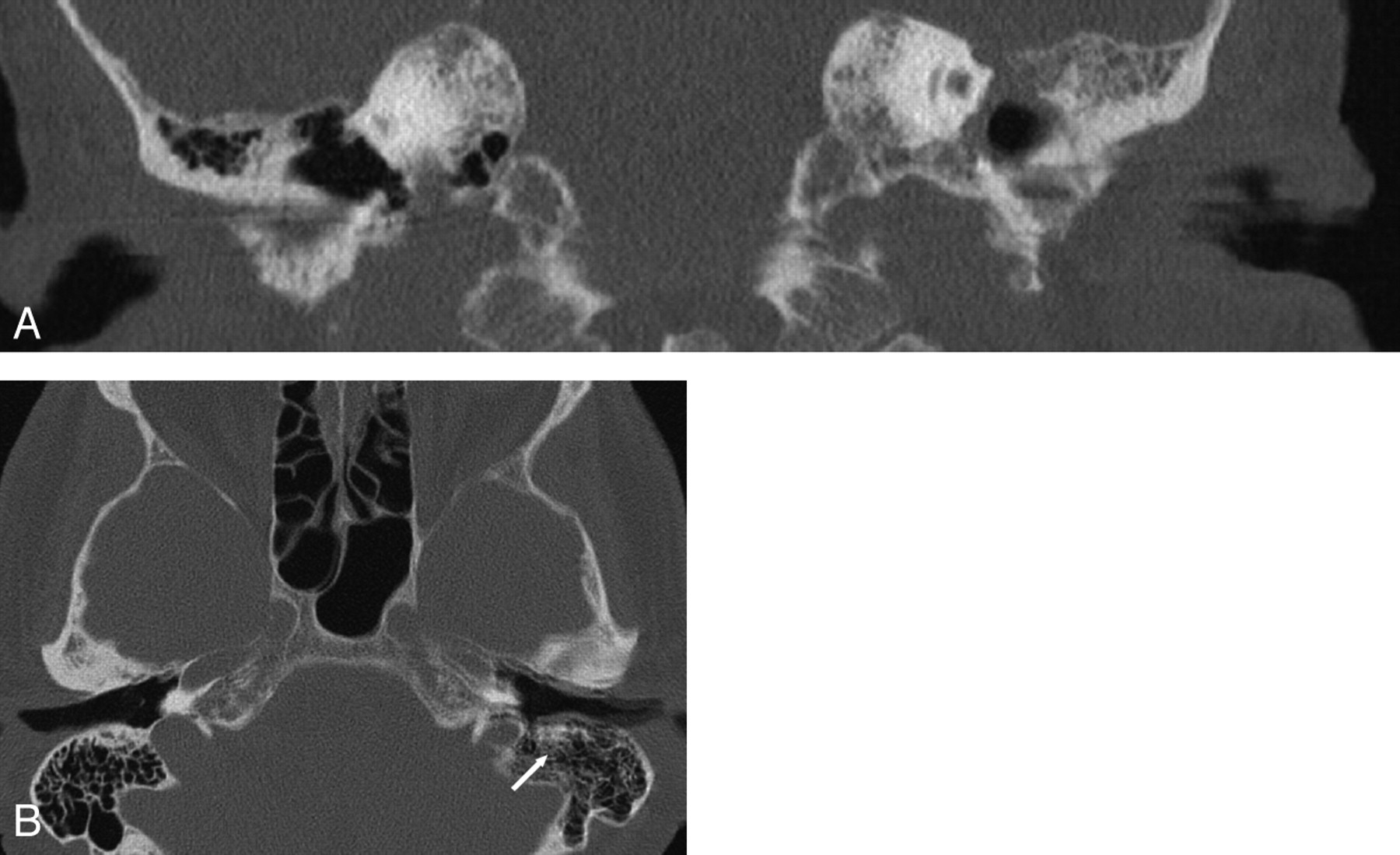
MSCT of the temporal bone, coronal (A) and axial (B) MPR, section thickness 0.8 mm. No moving artifacts are found in the SST scans, whereas the image quality of MSCT is decreased due to the patients moving in 2 cases (A and B). In 1 of those 2 individuals, the mastoid segment of the facial nerve canal (arrow) can barely be seen on the left side due to motion artifacts (B). However, image quality was sufficient to establish a diagnosis in both patients; thus, the examinations did not need to be repeated.
CT plays a major role in overall radiation exposure of patients. Therefore, it would be desirable to find radiation-saving techniques for CT. In this study, SST led to a reduction of the CTDIvol and DLP of 67% and 79%, respectively, compared with MSCT with a comparable diagnostic quality and, thus, could be an interesting alternative.
A limitation of this study is that the highest possible spatial resolution of the MSCT protocol was not assessed. Whereas SST used a collimation of 0.75 mm, collimation was 0.4 mm with MSCT. However, image evaluation was performed with a constant section thickness of 0.8 mm for both SST and MSCT by using MPRs; thus, the 2 series were made comparable.
Moreover, a possible influence of the slightly different milliampere-second (250 in SST versus 230 in MSCT) and FOV (200 in SST versus 141 in MSCT) on image quality requires discussion. Subsequent studies should be performed with image acquisition at constant section thicknesses, FOVs, and exposure parameters, to confirm our findings.
The evaluation was performed with a windowing of 4000 HU at a center of 700 HU; therefore, we do not think the contrast that was given for SST had any influence on the results of our study.
Because subjective image quality was different in SST and MSCT, a possible influence of this nonintended “unblinding” of the studies on the evaluation must be borne in mind. Although all examinations were performed to examine pathologies at the temporal bone, the visualization of these pathologies was not evaluated in this study. It is not clear whether using this new technique would be equally informative compared with MSCT in a specific disease process or patient population. This question has to be addressed in further investigations.
Conclusions
Our data show that SST and MSCT of the temporal bone do not differ significantly in terms of diagnostic quality if evaluated at a constant section thickness. In only 2/38 anatomic structures was a significant difference found, with MSCT being superior in 1 of those 2 instances. The shorter imaging time of SST may have particular application in uncooperative patients and children; in addition, all patients can benefit from the dramatic reduction of radiation exposure compared with MSCT.
Footnotes
-
Paper previously presented at: Annual Meeting of the Radiological Society of North America, November 28-December 3, 2010, Chicago, Illinois; Annual Meeting of the European Congress of Radiology, March 4–8, 2010, Vienna, Austria; and Annual Meeting of the German Congress of Radiology, May 12–14, 2010; Berlin, Germany.
References
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.