
Abstract
SUMMARY: Although radiography of the spine began shortly after Roentgen's discovery in 1895, there was little written in the medical literature about spine imaging until nearly 25 years later with the development of myelography, first by using air and then a variety of positive contrast agents. The history of spine imaging before CT and MR imaging is, in large part, a history of the development of contrast agents for intrathecal use. The advent of CT and, more important, MR imaging revolutionized spine imaging. The spinal cord and its surrounding structures could now be noninvasively visualized in great detail. In situations in which myelography is still necessary, advances in contrast agents have made the procedure less painful with fewer side effects. In this historical review, we will trace the evolution of spine imaging that has led to less invasive techniques for the evaluation of the spine and its contents and has resulted in more rapid, more specific diagnosis, therapy, and improved outcomes.
ABBREVIATION:
- LP
- lumbar puncture
There was very little in the medical literature about spine imaging until nearly 25 years after Roentgen's discovery of the x-ray in 1895. The development of contrast studies of the spine in the 1920s, first by using air and later various radiopaque contrast agents, was the first major development. During the next 50 years, a variety of contrast agents was introduced with the goal of improving diagnostic specificity with less toxicity. The advent of CT and MR imaging dramatically changed the way the spine was imaged. These discoveries have advanced the field of neuroradiology and improved the lives of patients via easier, safer, more rapid diagnosis and treatment.
The Beginning: Spine X-Rays
Unlike imaging of the skull and brain, about which textbooks were published as early as 1912, there is very little in the medical literature on spine imaging until the 1920s.1 Historic reviews indicate spine x-rays came into use shortly after Roentgen's discovery in 1895.2 The main use was to identify fractures and foreign bodies.3,4 As early as 1897, the noted neurosurgeon Harvey Cushing, in his first publication, reported on a patient with Brown-Sequard syndrome after a gunshot wound, in which spine x-rays showed the bullet lodged in the C6 vertebra.5 It took at least 10–15 minutes, if not longer, to obtain an exposure of the spine, and there was no way to angle the x-ray tube or eliminate scattered radiation.6⇓–8 The reason for the dearth of literature on spine imaging before approximately 1920 is not entirely clear. Bull7 suggests that clinical localization of spinal lesions presented less of a dilemma than intracranial lesions; thus, there was little impetus to develop imaging of the spine beyond x-rays. Others suggest, however, that little useful information was obtained from early spine x-rays beyond identifying fractures and foreign bodies.2 Tomography was introduced as early as 1914.9 This allowed the detection of subtler abnormalities such as complex fractures, bone fragments within the spinal canal, and cortical erosions; however, it was still only osseous changes that were detectable.8,10 Despite these limitations, spine x-rays have remained a mainstay of imaging for a variety of traumatic and nontraumatic conditions of the osseous spine, unlike skull x-rays, which are now virtually obsolete.
Contrast Studies of the Spinal Canal
Walter E. Dandy, the noted neurosurgeon, published the first description of pneumoencephalography and its use in diagnosing intracranial tumors and hydrocephalus in 1919.11 In this article, he noted that the normal spinal cord could be seen outlined by the air injected into the spinal canal. He postulated that the same technique could be used to localize spinal cord tumors with the air column extending up to the level of the lesion. However, he did not publish any more on this topic until 1925.12 In 1921, the injection of air into the subarachnoid space followed by x-ray examination was described independently by 2 Scandinavian physicians. Hans Christian Jacobaeus, a Swedish internist, reported on the use of pneumomyelography to diagnose spinal cord tumors.13 This development evolved from his earlier unsuccessful attempts to treat tuberculous meningitis by replacing 100 mL of CSF with air.13,14 Sofus Wideröe, a Norwegian surgeon, described a similar procedure to diagnose a spinal cord tumor.15
A year later, French physician, Jean-Athanese Sicard, and his student, Jacques Forestier, reported on the intrathecal use of iodized poppy seed oil, Lipiodol (Andre Guerbet, Aulnay-sous-Bois, France), for diagnosing spinal masses.14,16 This was a somewhat fortuitous development. Although it was known at the time that Lipiodol was radiopaque, Sicard injected it into lumbar muscles or the epidural space to treat sciatica and other neuralgias.16,17 Occaionally, he took x-rays after the epidural injection of Lipiodol to assess tumor or infection.16 It was by accident that a student of Sicard injected the Lipiodol into the thecal sac.17 After ensuring that there were no ill-effects to the patient, Sicard looked at the patient's spine on the fluorescent screen and saw that the Lipiodol had descended to the bottom of the spinal canal. Sicard then placed the patient in the Trendelenburg position and was able to see the cranial flow of Lipiodol within the dural sac.14,17 A year later, Sicard and Forestier began injecting Lipiodol into the subarachnoid space by cisterna magna puncture.17 In 1932, Sicard and Forestier published a book on the diagnostic and therapeutic uses of Lipiodol, which, in addition to myelography, included imaging of the respiratory, gastrointestinal, and genitourinary systems.18
In 1925, Dandy reported on more than 30 spinal cord lesions that had been localized by gas myelography; however, he was aware of Sicard's discovery and even indicates in the article that he had used Lipiodol himself via both LP and cisternal puncture.12 Dandy preferred injecting the Lipiodol by cisternal puncture because he thought it was more comfortable for the patient compared with LP, for which the patient had to lie head down.12 The same year, an American neurosurgeon, William Mixter, also reported on the use of Lipiodol in diagnosing spinal cord tumors.19
Lipiodol was originally developed in 1901 for therapeutic use, which in addition to the aforementioned treatment of sciatica and neuralgias, included syphilis, cardiovascular and respiratory diseases, leprosy, and goiter.20 Its use for myelography was widely accepted in France after the publication of Sicard and Forestier's article. However, its acceptance in other countries was tempered by concern over its safety.21 Even in their original article, Sicard and Forestier noted that patients experienced pain for 2–3 days after intrathecal injection of Lipiodol.16 Later, it became known that it induced inflammatory changes and arachnoiditis.17,21 Because of its slow absorption by the body, there was also the concern that the retained Lipiodol could become encapsulated and form pseudotumors.21 Lipiodol also separated into globules when mixed with CSF, which led to fragmentation of the contrast column.8 Despite these drawbacks, Lipiodol continued to be used mainly to diagnose spinal cord tumors and cord compression in the late 1920s and early 1930s.22 Because these conditions were relatively rare, many clinicians in the United States at the time thought that the benefits of making a correct diagnosis with Lipiodol myelography likely outweighed the complications in these infrequent situations.22,23
Introduction of Additional Contrast Agents
In 1931, Christian Georg Schmorl published his study on disk degeneration by using both radiographic and pathologic findings.24 Three years later, Mixter and Barr published their classic article on ruptured (their preferred terminology) intervertebral disks as a cause of radicular symptoms and sciatica, with surgery being the preferred treatment.25 Before this, radicular symptoms were generally thought to be due to cartilaginous neoplasms. Most of the patients in their series had a Lipiodol myelogram before the operation. Two years later, Hampton and Robinson published their classic article on the myelographic findings of ruptured intervertebral disks (Fig 1).26 These developments led to an increased demand for myelography, for which Lipiodol was the only available positive contrast agent.22,23 In 1941, Kubik and Hampton published the first description of removing iodized oil by lumbar puncture after myelography to prevent its irritating effects. The authors hoped this technique would alleviate some of the trepidation associated with myelography and allow more patients with disk herniations to be correctly diagnosed and treated.27

Myelogram in a 30-year-old man with radicular pain. A, Lateral lumbar myelographic image shows a typical extradural defect indenting the ventral dural sac at L4-L5 (arrow). B, Frontal lumbar myelographic image shows the defect, which is also resulting in poor filling of the right L5 nerve root sleeve (black arrow). Note that the needle remains in place (white arrow), presumably for removing the contrast.
During this time period, there were additional attempts to develop a myelographic contrast agent that would provide good visualization without side effects or the need for removal.23 In the late 1930s and early 1940s, articles by William Nosik proposed using thorium dioxide (Thorotrast Chemische Fabrik von Heyden, Dresden, Germany) for myelography followed by what was termed forced cerebrospinal drainage of the CSF containing thorium dioxide.28 The use of thorium dioxide for myelography never gained wide acceptance because of concerns over it nonabsorbable radioactive properties.22 There are case reports of serious unfortunate complications associated with its use for myelography, including severe arachnoiditis and spinal tumors, including meningioma and schwannoma.29,30 In Sweden, the iodinated water-soluble contrast agent methiodal (Abrodil, Schering, Berlin-Wedding, Germany) was introduced in 1931; however, it was so irritating that it could only be used in the lumbar region and then only under spinal anesthesia.22,31
Because of the relatively poor options for positive myelographic contrast agents, gas myelography remained in use in many places, especially Sweden.32 CSF needed to be drained from the spinal canal and up to 90 mL of air introduced, to obtain optimal results.14 Gas and, in some instances, oxygen, because it was rapidly absorbed from the subarachnoid space, were used in myelographic examinations into the early 1970s.32,33 While some thought gas myelography was safer than contrast myelography, it was not totally pain-free for the patient and the diagnostic information obtained was more limited compared with that for positive contrast agents.23
Effort to find a safer myelographic contrast agent resulted in the introduction of iophendylate (Pantopaque, Lafayette Pharmacal, Lafayette, Indiana) in the early 1940s.34 It was less viscous and less prone to globule formation than Lipiodol, thus easier to inject and manipulate throughout the spinal canal and even into the basal cisterns.8 When it was first introduced, it was thought to be slowly absorbable by the body, up to 3 mL/year, though even at that time, aspiration of the agent from the spinal canal was recommended at the end of the procedure.34 Later, it was determined that for all practical purposes, it was not absorbable.22 It was thought somewhat safer than Lipiodol because it could be more easily removed.22 Those who performed myelograms with iophendylate have described the difficulty in removing it because it had to be pooled into 1 globule by gravity and then aspirated with a lumbar puncture needle. The negative pressure on the needle required to withdraw the contrast often resulted in traction on, and sometimes frank aspiration of, a nerve root, resulting in significant patient discomfort.35 Within a few years of its introduction, reports of complications related to iophendylate myelography began to appear, including hypersensitivity reactions, meningitis, and arachnoiditis, which, in some cases, resulted in significant morbidity and even mortality.22 Blood mixing with the iophendylate increased the risk of arachnoiditis, and a bloody spinal tap became a relative contraindication to its use.8 However, some estimate that the frequency of clinically significant arachnoiditis was rare, possibly a fraction of 1 percent, and iophendylate continued to be used for 30 years because no safer agents were developed.14,22
Introduction of Water-Soluble Contrast Agents
The 1960s saw the introduction of new ionic water-soluble contrast agents. Meglumine iothalamate (Conray, Mallinckrodt, St. Louis, Missouri) and meglumine iocarmate (Dimer X, Laboratories AndreGuerbet, Paris, France) could both be used for myelography without spinal or general anesthesia, unlike the earlier used methiodol.36,37 Compared with iophendylate (Pantopaque), these agents provided better filling of the nerve root sheaths.37 While still neurotoxic, they were less so than other ionic water-soluble agents introduced around the same time. Acute side effects associated with their use included muscle spasm, paresthesias, and seizures.37 As with the older contrast agents, adhesive arachnoiditis was a long-term complication.38 Their use was mainly limited to lumbar myelography, they never gained wide acceptance, and the use of Pantopaque and Abrodil continued in the United States and Europe, respectively, into the 1970s. Inadvertent use of other ionic water-soluble contrast agents has resulted in severe complications, including severe muscle spasms, seizures, cerebral edema and hemorrhage, coma, paralysis, hypotension, hyperthermia, rhabdomyolysis, multisystem organ failure, and death.39 Sporadic reports of such inadvertent use have continued into the 21st century. Radiologists must remain vigilant when performing myelography to ensure that only the appropriate contrast agents are used.
Metrizamide (Amipaque, Nyegaard and Company, Oslo, Norway), the first nonionic water-soluble contrast medium for myelography, was introduced in the early 1970s.38 Side effects were milder than those with the ionic water-soluble agents, consisting of mainly nausea and vomiting, though there were infrequent reports of more serious side effects, including seizures, hallucinations, and aseptic meningitis. Unlike Pantopaque, it was not associated with arachnoiditis.38 Use of this agent resulted in excellent delineation of the nerve root sleeves and greater accuracy in the diagnosis of lumbar disk disease compared with Pantopaque.40 It could also be used for cervical and thoracic myelograms (Fig 2). It was absorbed into the blood stream, so it did not need to be removed at the end of the procedure.38

Frontal image from a cervical myelogram showing a typical intradural extramedullary mass. The mass is widening the adjacent subarachnoid space with a meniscus of contrast surrounding the mass (black arrows). The cervical cord is compressed and displaced away from the mass (white arrows).
The following decade saw the introduction of newer nonionic water-soluble agents that are still used today, including iohexol (Omnipaque; Nycomed, Princeton, New Jersey) and iopamidol (Isovue; Bristol-Myers Squibb, Princeton, New Jersey).41,42 These are associated with less toxicity than metrizamide.43 Although not without risk, the side effects are generally milder, consisting mainly of headache. A small percentage of patients develop confusion, radicular pain, and meningismus following their use, and seizures have rarely been reported.42⇓–44
Endomyelography
If a myelogram showed cord enlargement, particularly if the enlarged cord was collapsible or partially collapsible, suggesting a cystic or partially cystic mass, a cord puncture could be performed at the widest part of the cord enlargement. If a cystic mass was encountered, the fluid would be drained and air or positive contrast could be injected. This was then followed by radiography and tomography while the patient's positioned was varied. This was referred to as endomyelography or myelocystography.33,45 The extent of the cyst and the character of the cyst wall could be assessed. If mural nodules were seen in the cyst, these suggested a neoplastic cyst, whereas a smooth cyst wall implied a non-neoplastic process.33,45,46 This procedure was apparently relatively pain free if a syrinx was punctured, perhaps related to extreme thinning of the cord, while puncture of tumoral cysts could be painful.46 Publications pertaining to this procedure indicate that there were no significant complications. Careful myelography needed to be performed first to assess any abnormally enlarged vessels which, in conjunction with an enlarged cord, would suggest an hemangioblastoma or AVM, which was considered a contraindication to performing this procedure.33,46 The first description of this procedure was in 1928, and though it does not appear to have been performed frequently, there are case reports of its use up until the 1980s (Fig 3).46

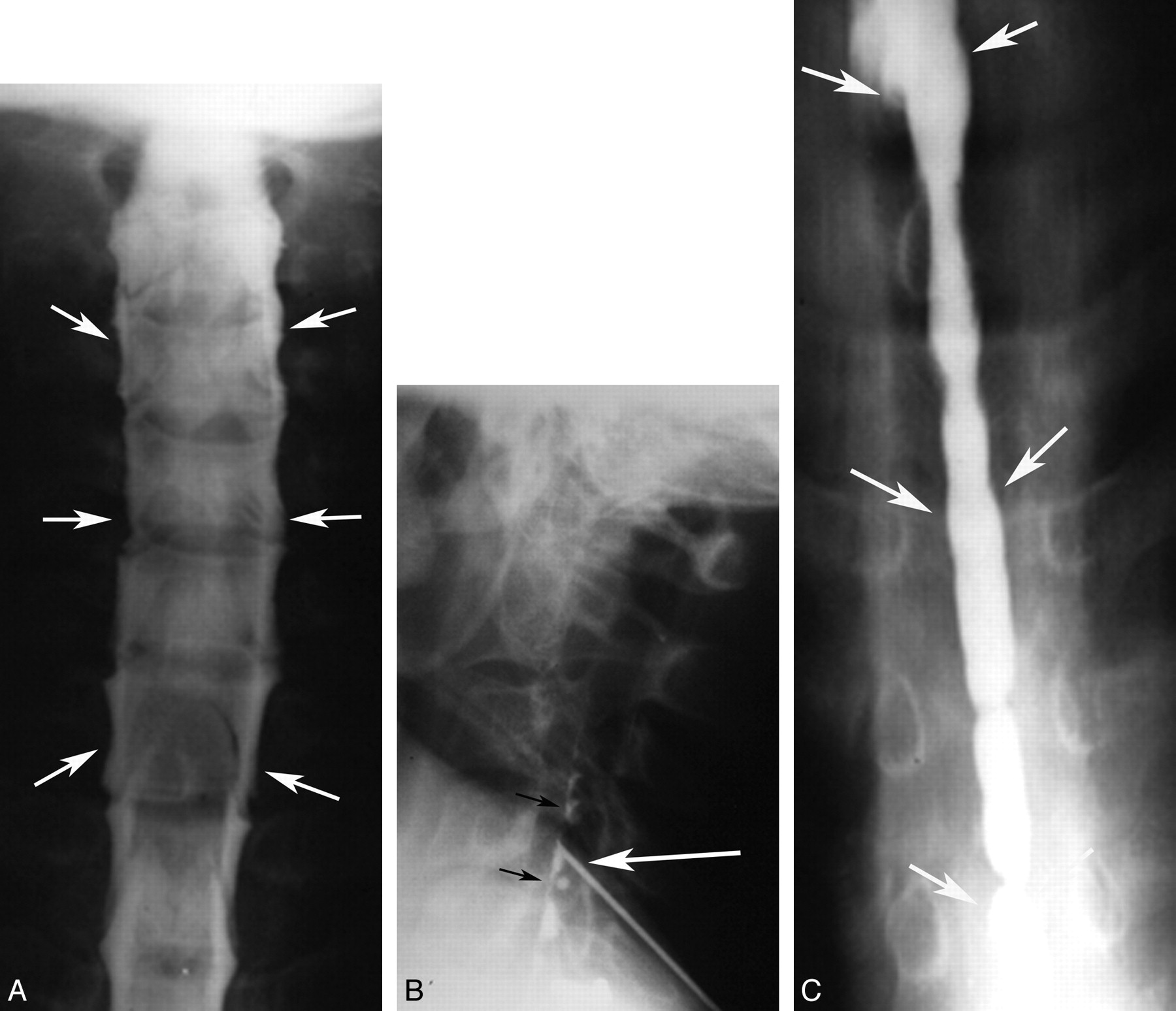
Cervical syrinx cavity demonstrated by myelography and myelocystography. A, Frontal cervical myelographic image shows a typical intramedullary mass with enlargement of the cord and thinning of the surrounding subarachnoid space (arrows). B, Lateral image of the cervical spine obtained during cyst puncture at the C4 level shows a needle tip projecting over the middle of spinal canal (white arrow) with a small amount of contrast in the cyst (black arrows). C4 was chosen as a site of puncture because this was where the cord was most expanded. C, Frontal image of the lower cervical and upper thoracic spine obtained following needle removal, showing contrast with a cystic cavity, compatible with a syrinx (arrows) extending inferiorly to approximately T7. It was not uncommon for the syrinx to be more extensive than suggested by myelography.
Spinal Angiography
Although cerebral angiography was first successfully performed in 1927 by Egas Moniz, it was nearly another 40 years before spinal angiography was attempted.47 Before this, myelography was the main diagnostic technique to diagnose spinal vascular malformations, which were seen as serpiginous filling defects in the contrast column.48 Initial attempts to visualize spinal vascular lesions or the artery of Adamkeiwicz used injections into the subclavian artery or aorta, depending on the location of the suspected lesion.49 Subsequently, selective catheterization of the vertebral, intercostal, and lumbar arteries was described using the Seldinger technique.50 Subtraction techniques that were developed in the 1960s helped in the visualization of the small abnormal vessels associated with spinal vascular malformations.48 Many patients experienced lower extremity spasms during these procedures, which was thought to be related to the neurotoxic effects and hypertonicity of the early ionic water-soluble contrast agents.50,51 The complication rate following spinal cord angiography, including spinal cord injury, was initially high; however, with advances in angiographic techniques and contrast agent formulation, complication rates are now similar to those for cerebral angiography.51 Although CTA and MRA techniques of the spine are now possible, spinal angiography remains the definitive test for diagnosing and, in many instances, guiding the treatment of these lesions (Fig 4).52

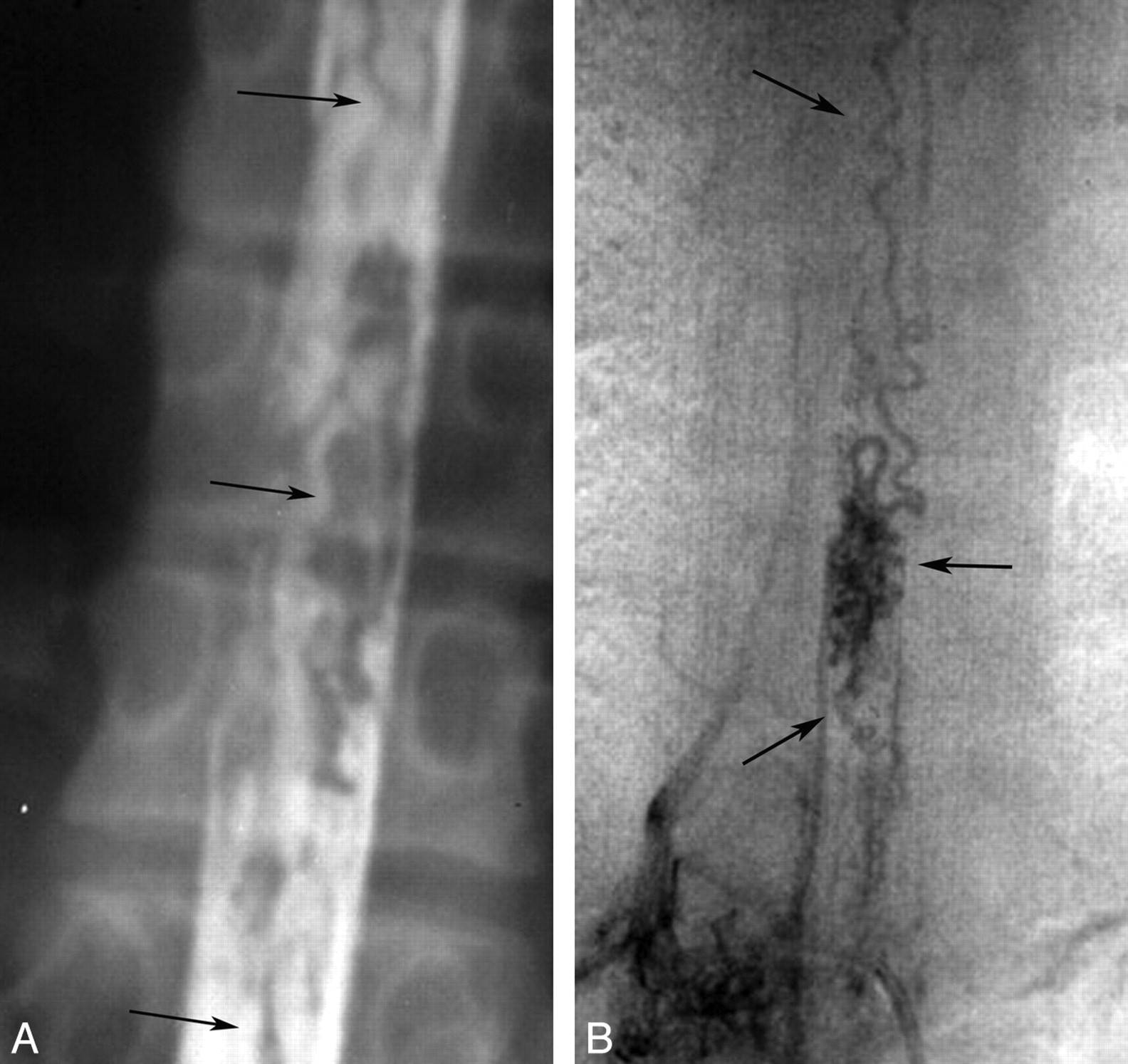
Spinal cord AVM diagnosed with myelography and angiography. A, Frontal myelographic image of thoracic spine shows multiple serpiginous filling defects (arrows) compatible with enlarged vessels from a vascular malformation or vascular neoplasm. B, Frontal image of the thoracic spine from a spinal angiogram shows an abnormal tangle of vessels (arrows) compatible with an AVM.
Cross-Sectional Imaging of the Spine
The first CT scanner introduced in 1973 was only capable of imaging the head.53,54 The following year, Robert Ledley, a dentist by training with an MA in physics, who was a professor of physiology, biophysics, and radiology at Georgetown University, developed the first whole-body CT scanner.55 Ledley, who founded the National Biomedical Research Foundation in 1960, had recently lost his National Institutes of Health funding and was looking for a project to maintain his lab. He was shown a brochure of the original Electric and Musical Industries CT scanner (ACTA Scanner, Pfizer, New York, New York) by a neurosurgeon at Georgetown University.56 Frustrated by the limitations of this scanner and aware of Allan Cormack's work, he determined that he could build a CT scanner by using the convolution image-reconstruction technique that could image the whole body.17,56 The prototype scanner was built with the help of a local machine shop and Cadillac car dealership.56 The first articles on this technique appeared in late 1974 and early 1975, including an article on its use in the diagnosis of syringomyelia by Ledley and neuroradiologist Giovanni Di Chiro.57 The axial images of the spine were 7.5 mm thick with a 2-mm gap.
Additional articles on CT of the spine soon followed, which included descriptions of congenital anomalies, spinal canal stenosis, degenerative changes, spinal canal and spinal cord masses, vascular lesions, bone destruction, and fractures.58 The first report of a postmyelogram CT, referred to as computer-assisted myelography, was in 1976 by Di Chiro and Shellinger, who indicated that the spinal cord outline could be more easily seen in this manner than with plain CT (Fig 5).59 During the next several years, articles describing the efficacy of combining myelography with CT in a variety of pathologic conditions were published.60 In the early 1980s, lumbar spine CT after IV contrast administration was used to aid in the diagnosis of degenerative disease, especially in the cervical spine, in the postoperative lumbar spine to differentiate recurrent disk from scar, and in tumors and inflammatory diseases of the spine.8

Metrizamide CT myelogram. A, Axial image at L5 shows a low-lying tethered cord (arrow). B, Axial image at the level of the sacrum shows an intraspinal lipoma (arrow).
Although the history of MR imaging dates back to the 1940s, the first commercial MR imaging scanner was introduced in 1980 and the first superconducting magnet was put in clinical use in 1981.61 Publications on the clinical use of MR imaging of the spine began appearing in the literature in 1983. These initial studies were performed on 0.15T-0.6T magnets, and spatial resolution and signal-to-noise ratios were poor by today's standards. The minimal section thickness for MR imaging was 1–1.5 cm, and a T2-weighted sequence could take up to 40 minutes to perform. However, the tissue characterization and multiplanar capability allowed delineation of a variety of intramedullary, intradural-extramedullary, and extradural processes without the need for contrast or ionizing radiation.62⇓–64 Technical advances came rapidly, including multisection multiecho techniques, sequence optimization, surface coils, and higher field strength units, which resulted in improved contrast and spatial resolution.65 Gadolinium contrast agents were first suggested in the early 1980s, with FDA approval of gadolinium chelates in 1988, which improved the detection and characterization of many diseases involving the spine.66 For the first time, the spinal cord and cord pathology could be directly visualized rather than the margins of the cord simply being outlined by contrast.
Advances in CT and MR Imaging of the Spine
Technologic advances in CT and MR imaging have continued unabated since their introduction into clinical use. Advances in CT technology have resulted in thinner sections, improved spatial resolution, faster imaging, fewer motion artifacts, and larger areas of coverage.67⇓–69 Although 3D reconstruction of CT images was first attempted in the 1970s, improved spatial resolution with isotropic voxels allowing high-quality multiplanar and 3D reconstructions is a more recent development. Faster scanning allows improved contrast use with angiographic imaging and dynamic scanning.68,69 These advances have resulted in CT of the spine with multiplanar reformatted images having essentially replaced conventional x-rays for the evaluation of spinal trauma, especially in the cervical spine in patients with high risk of injury, due to the improved sensitivity and specificity of CT compared with x-rays.70 CT is also the technique of choice when evaluating the spine for nontraumatic osseous abnormalities. CT myelography remains an important tool in the diagnosis of spinal disease and not just in patients who cannot have MR imaging. CT myelography is useful in the postoperative spine, with fewer artifacts related to surgical hardware than MR imaging, and in assessing spinal canal stenosis, foraminal stenosis, and nerve root compression.71,72 Myelography can be performed in a dynamic fashion, which may be helpful in the diagnosis of spinal stenosis and in evaluating CSF leaks.71 CTA of the spine is now possible and may be helpful in diagnosing and guiding the further management of spinal vascular malformations.73
The advances in CT technology resulting in increasing use have led to concerns over the radiation exposure patients receive during these studies.74 In light of these concerns, CT manufacturers have developed dose modulation and iterative reconstruction techniques that decrease patient dose without sacrificing image quality.75,76 Radiologists need to be advocates for patient safety by using protocols that limit radiation exposure and, when appropriate, substituting examinations without ionizing radiation, such as MR imaging.74
Spinal MR imaging research aimed at acquiring images faster with better contrast and spatial resolution. This led to developments such as fast spin-echo and gradient-echo sequences, echo-planar imaging, k-space substitution, parallel imaging, and phased-array coil technology.77,78 Spatial resolution improved, and 3D imaging with MR imaging became possible. As described in the earlier article in this series on the history of neuroradiology, MRA, DWI, DTI, CSF flow studies, MR spectroscopy, fMRI, and perfusion MR imaging were all introduced. More recently 3T scanners have been introduced into routine clinical work.79 Many of these newer techniques have had limited application in the spine due to technical difficulties that limit image quality, including the high magnetic susceptibility of the structures surrounding the spinal canal, the relatively small size of spinal canal structures, the large craniocaudal extent of the spine, CSF and vascular pulsation, respiration, and swallowing.80 DWI has been applied to the spinal cord and may be helpful in detecting acute cord ischemia as well as other cord lesions.81 MRA of the spine has been shown to be helpful in assessing the spinal vasculature and vascular malformations, particularly as a guide for further endovascular assessment and follow-up after treatment.82 Fetal MR imaging is now routinely used to further evaluate abnormalities seen on prenatal sonography and, in conjunction with fetal surgery, has led to improved outcomes in infants with myelomeningoceles (Fig 6).83,84 These developments have made MR imaging the primary technique used to assess spinal disease.
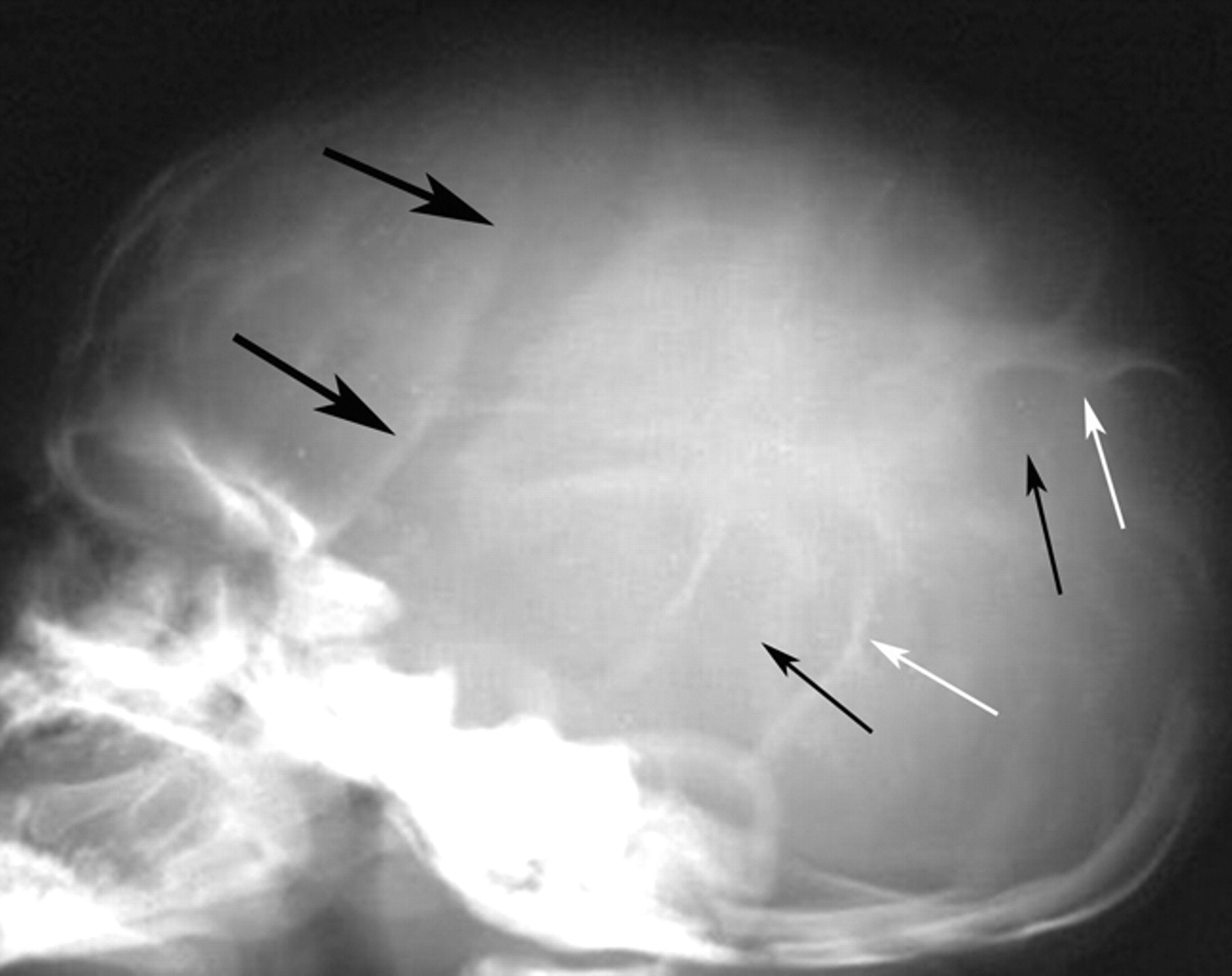
Lateral skull x-ray obtained in a 15-day-old boy born with a lumbar myelomeningocele, which ruptured and was infected. The only treatment available for this infant at this time was antibiotics. Note typical findings of lacunar skull or Lückenschädel, with areas of lucency (short black arrows) surrounded by areas of normal attenuation (white arrows), giving a soap bubble appearance to the skull. There is widening of the coronal suture (large black arrows), concerning for increased intracranial pressure.
Conclusions
To some, imaging of the spine may not be as enticing and imaging advances may not be as dramatic as those of the brain; nevertheless it remains a commonly used (some may even say overused) procedure in all imaging departments. As with imaging of the brain, profound advances have been made in spinal imaging, which have had a positive impact on the diagnosis and treatment of patients. We expect that progress will continue in the future that will lead to even less invasive, safer, and faster more specific diagnostic techniques, resulting in even earlier diagnosis and treatment with a continuing positive impact on patient outcome.
Footnotes
-
Disclosures: Suresh K. Mukherji—UNRELATED: Consultancy: Philips Medical Systems, Comment: Consultant. Douglas J. Quint—UNRELATED: Expert Testimony: Medical legal.
Indicates open access to non-subscribers at www.ajnr.org
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- ABBREVIATION:
- The Beginning: Spine X-Rays
- Contrast Studies of the Spinal Canal
- Introduction of Additional Contrast Agents
- Introduction of Water-Soluble Contrast Agents
- Endomyelography
- Spinal Angiography
- Cross-Sectional Imaging of the Spine
- Advances in CT and MR Imaging of the Spine
- Conclusions
- Footnotes
- References
- Figures & Data
- Info & Metrics
- Responses
- References