
Abstract
BACKGROUND AND PURPOSE: The initial angiographic occlusion rate is the strongest predictor of later rebleeding in previously ruptured coil-embolized cerebral aneurysms. Angiographic estimations of aneurysmal occlusion rates are, however, subjective in nature and confounded by methodologic problems. COR has been developed, and its superiority has been experimentally established to overcome subjective bias. The purpose of this study was to assess the clinical value of COR as a more objective predictor of aneurysm rebleeding when compared with SOR as described in the Raymond Classification.
MATERIALS AND METHODS: We applied COR in a consecutive series of 249 patients. Two DSA projections were selected independently by 2 blinded investigators. In cases of disagreement on the selected projections, a consensus decision was obtained. SOR were determined by 2 independent observers according to the Raymond classification. COR was measured by 2 blinded investigators. Interobserver variations were determined for SOR and COR. COR results were compared with SOR results and stratified as 100%, 99.9%–90%, 89.9%–70%, and <70% occlusion. SOR and COR were evaluated as predictors for aneurysm rebleeding.
RESULTS: Seven aneurysms rebled (2.8%; follow-up, 59 ± 35 months). In 20.9% of all cases, DSA selection was performed by consensus evaluations. Interobserver variations were statistically significant for SOR (P = .0030) but not for COR (P = .3517). Compared with COR, SOR overestimated the degree of aneurysmal occlusion in 81.9% of all cases. Only COR predicted rebleeding (P = .0162).
CONCLUSIONS: Unacceptable interobserver variations were shown for the standard SOR estimations. COR substantially reduced the impact of subjective bias. COR may, therefore, serve as an easily applicable more objective predictor of aneurysm rerupture. The remaining bias of COR, caused by 2D image analysis, may be overcome by use of direct 3D measurements.
ABBREVIATIONS:
- CARAT
- Cerebral Aneurysm Rerupture After Treatment
- COR
- computerized occlusion rating
- GOS
- Glasgow Outcome Score
- NS
- not significant
- OR
- odds ratio
- SOR
- subjective occlusion rates
Endovascular embolization is now the first-line treatment technique for most ruptured intracranial aneurysms.1 The primary disadvantage of coil embolization is a higher rate of aneurysmal rebleeding compared with surgical clipping. Aneurysmal rerupture results in mortality in up to 58% of patients.2,3 At this time, the only predictor of aneurysm rehemorrhage with level 1 evidence is the initial angiographic estimate of percentage occlusion.3 Despite its prognostic importance, the occlusion rate is only subjectively estimated in routine clinical practice. The most commonly used classification of angiographic outcome is that of Raymond4: complete obliteration = class 1, residual neck = class 2, and residual aneurysm = class 3. These estimations may be biased by subjective inaccuracies.
To overcome this subjective estimation bias, COR was introduced, and its validity was established for experimental as well as human aneurysms, each in comparison with histology, showing the intra-aneurysmal morphology with the highest resolution currently available.5⇓⇓–8
In the present study, COR was retrospectively applied to a large human series for assessment of its clinical value as a more objective predictor of aneurysm rebleeding when compared with SOR as described in the Raymond classification.
Materials and Methods
Patients
The study was approved by the local ethics committee. All patients between 18 and 75 years of age who underwent endovascular coiling for a ruptured intracranial aneurysm at the Department of Neurosurgery of the Medical University of Vienna between January 1998 and January 2005 were included in the analysis. Aneurysmal SAH was confirmed by noncontrast head CT or lumbar puncture. Patient data were prospectively entered into a computerized data base.9 From this data base, we extracted demographic data (name, age, sex), clinical baseline characteristics (date of SAH, Hunt and Hess grade,10 Fisher grade11), date of embolization, follow-up (date, Glasgow Outcome Scale score), and dates, if any, of documented aneurysmal rebleeding. Rebleeding was assumed to have occurred if follow-up CT demonstrated increased SAH compared with initial postinterventional CT scans and/or contrast agent efflux of the aneurysm on DSA with or without worsening of the patient's clinical condition.
Procedures
The technique of coiling intracranial aneurysms has been previously described in detail.12 We used standard embolization techniques with Guglielmi detachable coils (Boston Scientific, Natick, Massachusetts), including soft and 3D coil constructs.
Angiographic Evaluations
To minimize the bias caused by image selection, 2 experienced neurointerventional specialists not involved in the aneurysm treatment and blinded to the patient outcomes independently selected the projections for later SOR and COR evaluations. DSA examinations including dynamic sequences were available for all patients. Of the datasets, 2 DSA projections had to be selected for the evaluation. After we analyzed the entire DSA acquisition, the objective was to obtain a DSA projection at the phase of maximum arterial aneurysm perfusion, giving a representative overview of the aneurysm occlusion while focusing on the nonoccluded neck together with the length axis of the aneurysm. In cases of total aneurysm occlusion, the goal was to document the occluded neck on 2 perpendicular projections. In cases of initial disagreement on the projections selected by the 2 investigators, this was arbitrated by a consensus evaluation of both neurointerventional specialists.
Then SOR was estimated (100%, 95%, 90%, 80%, 70%, 60%…) by 2 independent investigators not involved in the aneurysm treatment and blinded to the clinical outcomes and the COR findings.
COR was calculated according to the previously published techniques of Sherif et al.6 With the custom-made software CoilControl-2D (NVTec Neurovascular Technologies, Vienna, Austria), COR was performed by another 2 independent investigators not involved in the aneurysm treatment and blinded to the clinical outcomes and SOR findings. We measured the following parameters:
Total aneurysm area (mm2): Borders of the contrast medium or coil-filled aneurysm and the orifice plane were outlined (Fig 1). If the outline of the aneurysm could not be visualized precisely on the selected DSA images, the aneurysmal contour on the corresponding pretreatment angiogram was superimposed over the postembolization DSA image.
Aneurysm neck width (mm): Distance of the orifice plane, where the cranial borders of the parent arteries merged with the aneurysm outline.
Aneurysm maximum length (mm): The longest distance between the orifice plane and the visible fundus of the aneurysm.
Aneurysm nonoccluded area (mm2): The area filled or refilled by contrast medium within the total aneurysm area was defined on the posttreatment DSA images by using an attenuation-gradient–based calculation. The attenuation range of gray levels of the radiopaque contrast medium in the aneurysm was defined by the attenuation range of the contrast medium in the parent arteries. On the basis of this range within the 256 gray levels of the digital image, the contrast medium–filled area was distinguished and false-color-labeled for measurement (Fig 1).
Finally, the occluded area of the aneurysm was calculated as the difference of “total area” minus “nonoccluded area” and given as percentage COR.
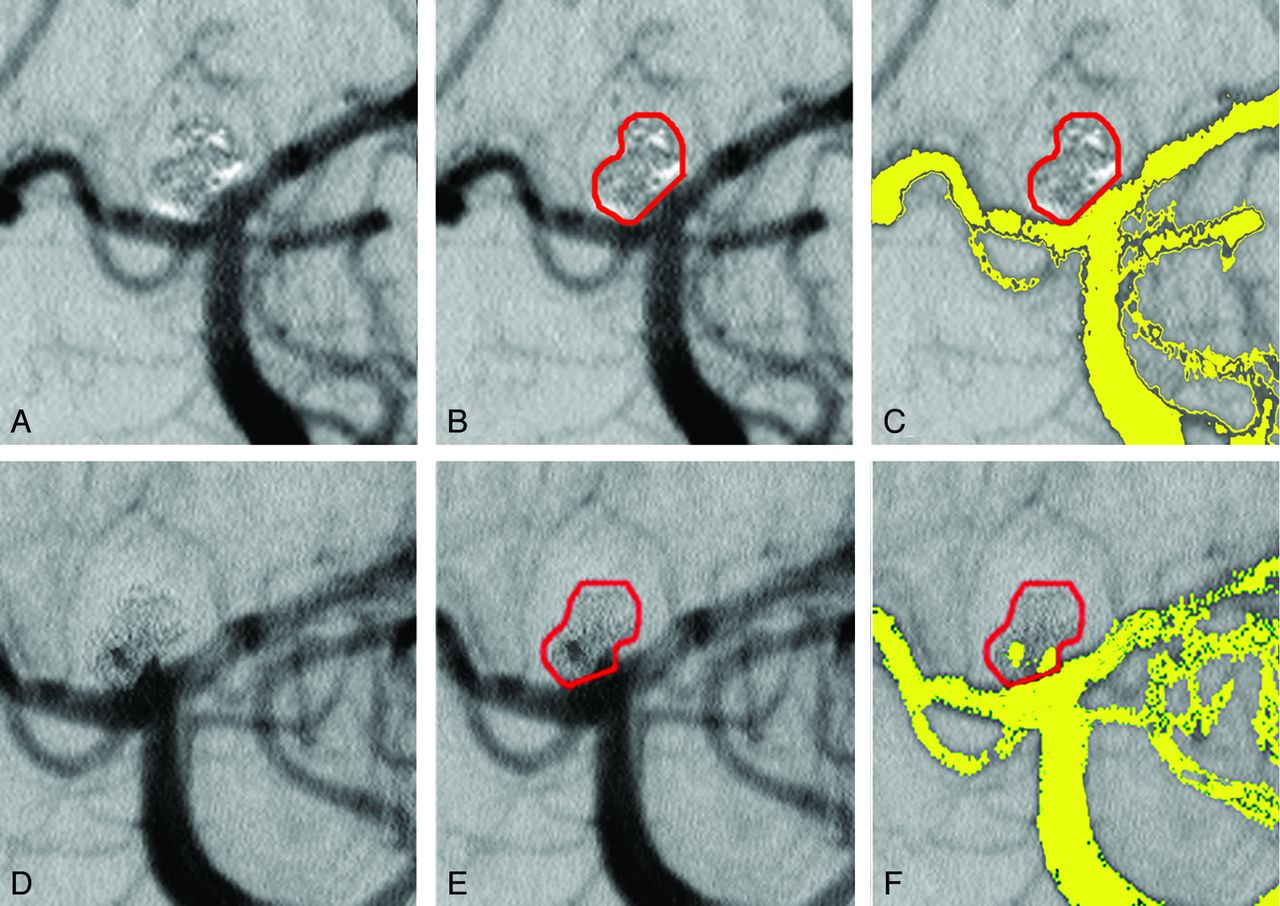
Computerized occlusion rating. A and D, Overview of the 2 selected projections. B and E, Definition of the total aneurysm area (red line), false-color-labeled contrast medium flow (yellow) (C and F), and nonoccluded area within the aneurysm (yellow) (F). This is a typical example demonstrating the need for precise image selection. Solely evaluating the first projection would result in 100% occlusion. As in the first projection (A–C), the occluded part of the aneurysm sac projects over the nonoccluded areas and hides them. A small rotation of the first projection then shows nonoccluded areas at the neck and in the aneurysm sac (D and F).
Statistics
Interobserver variability was calculated for SOR and COR by using the Wilcoxon test. The mean values of both observers were calculated for SOR and COR, aneurysm length, neck width, total aneurysm area, and nonoccluded aneurysm area.
Then COR, classified as 100%, 99.9%–90%, 89.9%–70%, <70%, and SOR classified according to the Raymond scale (1, complete obliteration = 100% SOR; 2, residual neck = 95%–90% SOR; 3, residual aneurysm = <90% SOR) were evaluated as predictors of outcome in univariate Kaplan-Meier analysis (logrank test) with censoring at the time of rebleeding. SOR and COR were compared by using the paired t test.
The clinical baseline parameters (Hunt and Hess grade, Fisher grade, aneurysm location) and aneurysm morphology parameters (size, length, aspect ratio, recanalized area, total area) were compared between reruptured and stable aneurysms by using the paired t test for continuous variables and the Kruskal-Wallis test for categoric variables.
Data are presented as mean ± SD. A P value <.05 was considered significant. SAS 8.02 (SAS Institute, Cary, North Carolina) software was used for all statistical calculations.
Results
Two hundred eighty-two patients met the inclusion criteria. Thirty-three patients were lost to follow-up, resulting in a follow-up rate of 88.3%. Patient characteristics (age, sex, aneurysm location, aneurysm length, neck width, aspect ratio, Hunt and Hess grade, Fisher grade, final GOS) are shown in Table 1. The characteristics of those patients with documented rebleeding of a treated aneurysm are shown in Table 2.
Characteristics of the patients
Characteristics of patients with aneurysm rerupture
A consensus evaluation of the selected DSA projections was necessary in 52 patients (20.9%).
There was statistically significant interobserver variation when using SOR measurements (P = .0030). For COR, the interobserver variation was not significant (P = .3517).
When using the SOR method, 84/56 patients had aneurysms stratified to Raymond class 1 (ie, complete obliteration of the aneurysm), whereas only 15/17 patients were calculated to have 100% aneurysm occlusion when using the COR technique. A similar number of patients were stratified to the class 2 aneurysm occlusion groups (SOR: 136/162 patients; COR: 126/122 patients). Whereas only 25/30 patients were stratified to Raymond class 3 when using the SOR method, the COR technique revealed 106/109 patients harboring residual aneurysms (ie, class 3 lesions). When we compared the mean values of SOR and COR, the SOR method overestimated the degree of aneurysm occlusion in 204 (81.9%) of the cases, with a mean overestimation of 6.24% OR (range, 0%–21.9% OR; P < .0001). In detail, 116 of 144 aneurysms (80.5%) stratified to Raymond class 2 by using the SOR method had <90% occlusion when using the COR technique.
During the follow-up period (59 ± 35 months, mean), 7 aneurysms rebled (2.8%), resulting in 2 deaths (Table 1)000000. Median time to rerupture was 5 days (range, 1–185 days).
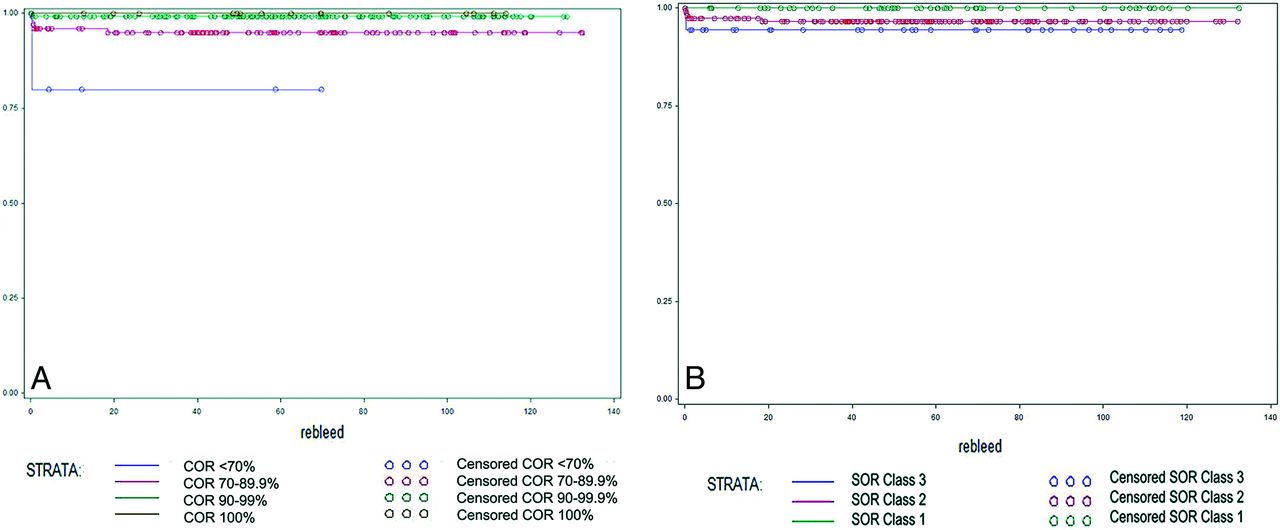
The degree of initial aneurysm occlusion as measured by using the COR technique was strongly associated with the risk of aneurysmal rebleeding. The risk of rerupture as calculated by using COR was 0% following 100% occlusion of the aneurysm, 0.7% for 90%–99.9% occlusions, 5.2% for 70%–89.9%, and 16.7% for occlusions below 70%. These differences again reached statistical significance (P = .0162 by logrank test, Table 3 and Fig 2A). In contrast, the degree of aneurysmal occlusion measured by using the SOR method was not significantly associated with the risk of rebleeding (P = .2466 by logrank test, Table 3 and Fig 2B).
Literature overview of important recent studies on aneurysm rerupture of embolized ruptured cerebral aneurysms
When comparing treated aneurysms that went on to rebleed with those that were clinically silent, we found distinct differences in the angiographic morphology of the lesions, particularly with respect to the size of the aneurysm neck and the aspect ratio. Most interesting, there was no significant correlation between absolute size of the recanalized area or total aneurysmal area with risk of aneurysmal rerupture. In contrast, we found smaller recanalized areas (8.95 versus 9.41 mm2, P = NS), smaller total aneurysm areas (46.41 versus 49.23 mm2, P = NS), and shorter aneurysm lengths (7.34 versus 8.11 mm, P = NS) in patients with aneurysmal rehemorrhage (Table 1).

Kaplan-Meier survival curves of aneurysm rerupture according to COR (A) and SOR (B).
Discussion
Comparison of Computerized versus Subjective Occlusion Ratings
Currently, the method of choice to estimate the degree of initial aneurysmal occlusion is SOR, a technique based on the work of Roy and Raymond.4 In their retrospective observational study of 116 patients with unruptured embolized aneurysms, they demonstrated a statistically significant relationship between the degree of initial aneurysmal occlusion and aneurysm recurrence. In addition to its prognostic value, additional strengths of this classification include its ease of use. It quickly became the standard method for aneurysm occlusion rating and was subsequently adopted for use in ruptured aneurysms.
One of the major dilemmas in the management of aneurysmal recurrence is the difficulty in distinguishing a benign aneurysmal neck remnant from a true residual aneurysm with the potential to enlarge and/or rupture. Because the Raymond classification relies on operator estimation alone, it is potentially biased by subjective inaccuracies. Reported rates of total aneurysmal occlusion (32%13–76%3) and the incidence of aneurysmal neck remnants (17%3–51%13) vary remarkably in the largest recently published series (Table 3); this variation underscores the clinical relevance of the problem. Erroneous overestimation of the initial aneurysmal occlusion by using the SOR method appears likely to confound standardized patient follow-up strategies, resulting in delayed recognition of residual aneurysms and ultimately in potentially preventable rehemorrhages.
Subjective inaccuracies confounding initial aneurysm occlusion assessment were also encountered in the largest available prospective multicenter trial of aneurysm rerupture, the CARAT trial. This study relied on SOR data only3 and introduced a modified subclassification of Raymond class 3 aneurysms (ie, those <90% occluded): Fifty-one patients (5.1%) were 70%–90% occluded, and 17 (1.7%) had a <70% occlusion rate. Moreover, in the surgical arm of the study, representing 70.6% of the total population, aneurysm occlusion was estimated by the surgeon after clipping in those cases in which DSA was not available. We think it is reasonable to question whether intraoperative differentiation among 70%, 80%, and 90% aneurysm occlusion is difficult, if not impossible, without additional imaging. Unfortunately, the CARAT trial does not specify how many patients underwent DSA or comparable intraoperative imaging technologies (eg, intraoperative indocyanine green angiography). According to direct correspondence with the study authors, assessment of these data was difficult; this problem illustrated the practical clinical problems encountered when attempting to classify posttreatment aneurysm occlusions.
To minimize the potential of subjective operator bias, 2D-COR has been introduced. Its validity was previously established for experimental and human aneurysms in comparison with histometric evaluations, displaying the “real” intra-aneurysmal morphology with the highest resolution power currently available.5,6 A major finding of these preliminary studies was the tendency of SOR to overestimate the extent of initial aneurysm occlusion. Particularly as it relates to the misclassification of the clinically ominous Raymond class 3 aneurysms, unacceptably high inaccuracies of SOR and a clear superiority of COR were shown.6
In the present study, 2D-COR was applied to a larger patient series. To assess for potential clinical benefit of 2D-COR over SOR, we compared the degree of interobserver variation for both methods. For 2D-COR, no significant interobserver variations were seen. Comparing SOR with 2D-COR in the present study, we found a tendency toward subjective SOR overestimation of occlusion rates in 81.9%, as has been previously reported.5,6 To our knowledge, the present study has the first data to precisely quantify the subjective interobserver bias inherent in SOR estimations of coil occlusion percentage. When we compared the results derived from the 2D-COR method with our own SOR data and the SOR data available in the literature, it is apparent that a trend exists toward reclassification of SOR class 1 aneurysms to 2D-COR class 2 lesions (99.9%–90%) and of SOR class 2 aneurysms to 2D-COR class 3 lesions (<90%). A possible reason for the discrepant evaluations of aneurysm occlusion derived from the 2 methods may be the higher resolution power of the COR technique (ie, a better gray value definition of the contrast agent). SOR estimation is not as precise as the computerized method, and smaller contrast agent–filled recanalized areas are easily underestimated or unrecognized. Additionally, COR provides a better definition of the aneurysmal border, enabling superimposition of pre- and postembolization images. Furthermore, using a semiautomated computerized technique such as CoilControl-2D (NVTec-Neurovascular Technologies) is helpful to correct for motion artifacts or superimposition of crossing vessels, thereby enhancing data quality. Crucial to profiting from these features is the availability of high-resolution DSA images.
Despite these advantages, 2D-COR remains limited for several reasons. The major shortcoming may be related to the 2D image evaluation of 3D structures. Even when meticulously focusing on the aneurysm neck plane together with the axis length of the aneurysm, it remains difficult to evaluate complex 3D volumetric geometries with only two 2D projection planes. This problem introduces methodologic as well as subjective bias, as demonstrated by the high percentage of necessary consensus decisions in the selection of the DSA projections (20.9%). This methodologic oversimplification of complex angioarchitecture is also a major shortcoming of SOR.7,8
Another possible source of bias may be the selection of the ideal time point of the DSA acquisition. In our experience, it is best to analyze the entire arterial DSA acquisition. The aim should be obtaining a DSA projection at the phase of maximum arterial aneurysm perfusion because this enables improved visualization of the contours of any possible neck remnant.
The shortcomings of 2D-COR could be overcome by direct 3D volumetry on 3D reconstructed datasets. The feasibility and superior precision of this method over 2D evaluations has been shown recently for experimental aneurysms in vivo.14 In the short-term, 2D-COR remains a fast, easy, applicable, and more objective method versus the present standard SOR. After image selection, COR measurements can be performed quickly (within 2–3 minutes), ensuring even peri-interventional clinical applicability. Principally 2D-COR can be performed with any postprocessing software that is directly installed on many DSA units.
The authors consider the 2D-COR technique a significant improvement compared with previously used subjective SOR estimations. It should be seen as a first step toward a more objective and standardized follow-up and risk-prediction strategy for a rapidly growing patient population. Moreover, 2D-COR could easily be applied retrospectively to existing series on the basis of 2D imaging, thus facilitating, for example, interstudy comparisons of the large trials with their extremely differing occlusion rate outcomes.
Aneurysm Rerupture and Initial Occlusion Rates
In the present study, we observed 7 aneurysmal reruptures (2.8%) during a mean follow-up period of 59 ± 35 months. When compared with recently published series,2,3,13,15⇓⇓⇓⇓–20 our rebleeding rate is in the higher range (1.0%20–3.6%13), though this may, at least in part, be explained by our longer length of follow-up. Similar to Sluzewski and van Rooij16 and Jarrti et al,13 most reruptures were seen within the first few days following embolization. Our rerupture-related mortality of 28.5% is relatively low compared with recently reported mortality rates of up to 58%.3 This may be at least partly related to the sensitive definition of rebleeding used the present study, applying criteria comparable with those of Jartti et al,13 who also reported lower mortality rates (14.3%).
The positive correlation between a lower initial aneurysmal occlusion by using the SOR method and a higher risk of aneurysmal rerupture has been seen in many larger recent studies.3,13,15⇓⇓–18 In 3 of these series, this trend was significant.3,15,16 Among these, the prospective multicenter CARAT trial resulted in the first level 1 evidence of this relation, despite its above-mentioned methodologic shortcomings. The relation of the initial occlusion rate and aneurysmal rerupture is apparently so strong that it even persists when the less accurate methods of SOR estimation are applied.
In contrast to the CARAT trial, Kang et al20 reported rerupture rates of 1%, irrespective of the initial degree of aneurysmal occlusion, for all Raymond aneurysm occlusion classes. Of note, successful embolization in the study of Kang et al was not defined by using the Raymond classification but mainly by packing attenuation. The insufficient accuracy of packing attenuation as a clinical parameter has been demonstrated in several publications.6,8 Therefore, packing attenuation was not evaluated in the present study.
An important finding of the present study is the robust statistically significant correlation of initial aneurysmal occlusion as measured by the 2D-COR technique and the subsequent risk of aneurysmal rerupture (P = .0162). In contrast to the published literature (Table 3), our population had a zero percentage rerupture risk for aneurysms with a 100% initial COR occlusion. The most likely explanation for this finding is the low number (n = 15) of COR-estimated 100% occlusions in our series. The only recent series without any instances of SOR class 1 aneurysm rerupture was that of Choi et al,21 a series of 91 patients with a mean follow-up of 34.4 months.
Finally, when comparing stable and reruptured aneurysms, we found considerable smaller nonoccluded areas, smaller total aneurysm areas, and shorter aneurysm lengths in patients with aneurysmal rerupture (Table 1). Therefore, small remnants and small aneurysms have the potential to be as dangerous as large ones. These results support the findings of Sluzewski and van Rooij,16 who found an inverse statistically significant relation of aneurysm rerupture with aneurysm length.
Limitations
The present study is limited by the retrospective single-center study design with a lower number of included patients compared with the largest available series.2,3 Statistical power is limited by the low number of documented instances of aneurysmal rehemorrhage. As previously discussed, 2D-COR, in its current form, relies on the evaluation of 2D images for the assessment of a 3D aneurysmal structure; therefore, a subjective bias in both the selection of the evaluated DSA projections and the time point of acquisition remains possible. Future systems enabling 3D COR evaluation will remove most of these theoretic biases.
Conclusions
For the evaluation of ruptured embolized aneurysms, the present clinical standard of subjective estimations of the coil occlusion rate results in unacceptably high interobserver variability. The new 2D-COR technique substantially reduces the impact of this subjective operator bias, thus serving as a more objective predictor of aneurysm rerupture. The remaining bias of 2D-COR, resulting from the inherent limitations of a 2D evaluation of 3D structures, may eventually be overcome by direct 3D volumetry of reconstructed 3D datasets. 2D-COR should be seen as a first step toward a more objective and standardized follow-up and risk prediction strategy for a rapidly growing patient population. In the short-term, 2D-COR may serve as an easily applicable, fast, and accurate tool in routine clinical practice.
Footnotes
Disclosures: Camillo Sherif—RELATED: shareholder of NVT Neurovascular Technologies, Ltd. Camillo Sherif also received scientific financial support from Boston Scientific Corporation, S&T Mircoinstruments, and Johnson & Johnson Inc. Andreas Gruber, Christian Dorfer, and Gerhard Bavinszki—RELATED: Support for Travel to Meetings for the Study or Other Purposes: received assistance with travel and meeting expenses from Boston Scientific Corp. Eva Lahnsteiner—RELATED: received research support for software development of the program CoilControl, which was used during the study. The other authors have no conflicts of interest.
References
- Received March 19, 2011.
- Accepted after revision October 25, 2011.
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Computerized Angiographic Occlusion Rating for Ruptured Clipped Aneurysms is Superior to Subjective Occlusion Rating
- An update to the Raymond-Roy Occlusion Classification of intracranial aneurysms treated with coil embolization
- Is long-term follow-up of adequately coil-occluded ruptured cerebral aneurysms always necessary? A single-center study of recurrences after endovascular treatment