
Abstract
BACKGROUND AND PURPOSE: Leukoaraiosis is a common finding among patients with ischemic stroke and has been associated with poor stroke outcomes. Our aim was to ascertain whether the severity of pre-existing leukoaraiosis is associated with outcome in patients with acute ischemic stroke who are treated with endovascular stroke therapy.
MATERIALS AND METHODS: We retrospectively analyzed data from 129 consecutive, prospectively enrolled patients with stroke undergoing endovascular stroke therapy at a single tertiary care center between January 2006 and August 2013. Leukoaraiosis was assessed as supratentorial white matter hypoattenuation on admission head CT and graded as 0–2 (absent-to-moderate) versus 3–4 (severe) according to the van Swieten scale. We dichotomized the 90-day mRS into good (0–2 or return to baseline) versus poor (3–6) as the primary study outcome. Incremental multivariable logistic regression analyses were performed to identify independent predictors of a poor 90-day outcome.
RESULTS: In all multivariable models, severe leukoaraiosis was independently (P < .05) associated with a poor outcome at 90 days (fully adjusted model: OR, 6.37; 95% CI, 1.83–12.18; P = .004). The independent association between leukoaraiosis and a poor outcome remained when the analysis was restricted to patients who were alive at discharge (n = 87, P < .05). Last, among patients who were alive at discharge, those with severe leukoaraiosis had significantly less frequent improvement on the mRS from discharge to 90 days compared with patients with absent-to-moderate leukoaraiosis (P = .034).
CONCLUSIONS: The severity of pre-existing leukoaraiosis is independently associated with 90-day functional outcome in patients with stroke who underwent endovascular stroke therapy. These results highlight the need to further explore leukoaraiosis as a promising surrogate marker for poor outcome after endovascular stroke therapy to improve risk assessment, patient selection, and early prognostic accuracy.
ABBREVIATION:
- EST
- endovascular stroke therapy
Thrombolysis with IV rtPA remains the only proved therapy for acute ischemic stroke.1 However, its efficacy is limited by several variables, including a narrow treatment time window and reduced efficacy with larger thrombus burden.1,2 In particular, proximal large intracranial artery occlusion portends a poor prognosis and poses a substantial therapeutic challenge.3 Endovascular approaches to recanalization may allow more frequent and rapid recanalization of the target vessel, which is critical for achieving better outcomes.2,3 However, despite the acceptable safety of endovascular approaches, definitive proof of superiority over IV thrombolysis in achieving good functional outcomes remains to be established.1,3 Understanding factors that influence outcome in patients undergoing endovascular stroke therapy (EST) is paramount to help improve selection of patients most likely to benefit from this therapy.2
While numerous studies have focused on procedural aspects, treatment window, and neuroimaging signatures of acute tissue injury, little is known regarding the potential contribution of preexisting white matter rarefaction (leukoaraiosis) on outcome.3⇓–5 Yet, leukoaraiosis is frequently encountered in the elderly6,7 and is well-known to contribute to worse outcomes after acute ischemic stroke.7,8 Given the expected tripling of the number of persons aged 60 or older in developed nations by 20509 and the increasing prevalence of stroke with advancing age,10,11 it is expected that an increasing number of patients with pre-existing leukoaraiosis will be treated with EST.12 Accordingly, it is important to understand the potential contribution of leukoaraiosis to functional outcome after EST.
To address this issue, we tested the hypothesis that the severity of pre-existing leukoaraiosis is associated with outcome as assessed by the 90-day mRS in consecutive patients with acute ischemic stroke treated with EST.
Materials and Methods
Study Population
This study was reviewed and approved by our institutional review board. We retrospectively analyzed 129 consecutive, prospectively collected patients with acute ischemic stroke who underwent EST at a single academic stroke center from January 2006 to August 2013. Of note, 42 (33%) studied subjects have been included in prior investigations.8,13 We adhered to the STrengthening the Reporting of OBservational studies in Epidemiology guidelines (www.strobe-statement.org).
All patients underwent head CT and CTA at admission. Demographics, NIHSS scores, laboratory data, comorbidities, preadmission medications, and stroke etiology (by using the Trial of Org 10172 in Acute Stroke Treatment classification),8,13 after completion of diagnostic evaluation, were collected on all patients. mRS scores were assessed at the time of presentation (preadmission mRS), discharge, and at 90 days by a stroke-trained physician or stroke study nurse, certified in mRS.8 When the mRS was unavailable, the same observers reconstructed the score from the case description, according to the mRS criteria.8
Neuroimaging Protocol
All CT sequences were obtained on a 64-detector row scanner (Brilliance; Philips Healthcare, Best, the Netherlands). CT was performed in a nonhelical mode at 120 kV(peak) and 200 mA, with data reconstruction at 5-mm axial sections. CTA was performed by using 64 × 0.625 mm detector configuration with a pitch of 0.673 from the arch of the aorta to the vertex by using 120 kV(p), 300 mA, and 0.5-second rotation time. Patients received 60–80 mL of iopamidol (Isovue 370; Bracco Diagnostics, Princeton, New Jersey) in the antecubital vein at a rate of 4 mL/s through a power injector followed by 40 mL of saline. 3D orthogonal MIP images were created in 3 planes.
Digital Subtraction Angiography
All endovascular procedures were performed by senior neurointerventionalists by using a biplane angiography unit with 3D rotational angiography capability (Allura Xper FD20/20; Philips) with patients under conscious sedation or general anesthesia. Endovascular access was obtained by a standard transfemoral approach.
Image Review and Analysis
CT and CTA were reviewed independently by experienced readers blinded to both clinical data and any follow-up scans. Variable window width and center-level settings were used for optimal ischemic hypoattenuation detection with CT and CTA.8,13
Leukoaraiosis was retrospectively defined by 2 readers (N.H. and J.Z.) as supratentorial white matter hypoattenuation on admission noncontrast head CT according to the STandards for ReportIng Vascular changes on nEuroimaging criteria,14 and it was graded on a 5-point van Swieten scale as previously described in detail (On-line Fig 1).15 Disagreements in readings were resolved by consensus. In the present study, leukoaraiosis was separately assessed in each hemisphere, but only the score from the nonischemic hemisphere was considered after unblinding. Hemorrhagic transformation on follow-up imaging was determined according to the European Cooperative Acute Stroke Study definition.16
Angiography-based collateral flow was graded from 0 (no collaterals) to 4 (complete) before EST,17 and final recanalization was assessed according to the TICI classification as previously defined.17 The time to recanalization was defined as the time from symptom onset (or last time known well) to the final attempt at recanalization.
To avoid classification bias and to minimize interrater variability,8 we also dichotomized the degree of leukoaraiosis (van Swieten scale 0–2 [absent-to-moderate] versus 3–4 [severe]), the presence of collaterals (grades 0–2 [poor] versus 3–4 [good]), recanalization (TICI 0–2a [poor] versus 2b-3 [good]), and the presence versus absence of parenchymal hemorrhage (parenchymal hemorrhage 1 and parenchymal hemorrhage 2) for statistical purposes.
Last, to assess the potential association among leukoaraiosis, infarct volume, and outcome, manual lesion assessment13,15 was conducted in patients who had follow-up imaging within 7 days of stroke onset (MR imaging: n = 43; CT: n = 25), allowing reliable measurements.
Statistics
Weighted κ statistics were used to determine the degree of inter-rater agreement in the van Swieten scale assessment in all 129 included patients and to determine κ values as previously defined.13 In addition, intrarater agreement was assessed in 65 randomly chosen patients who were graded 5 months apart by an experienced reader (N.H.).
Unless otherwise stated, continuous variables are reported as mean ± SD or as median (interquartile range). Categoric variables are reported as proportions. Between-group comparisons for continuous variables were made with the unpaired t and Mann-Whitney U tests, as appropriate. Categoric variables were compared by using the χ2 or Fisher exact test as appropriate.
Primary Analysis.
We defined the 90-day mRS dichotomized into good (0–2 or return to baseline) versus poor (3–6) as the primary study outcome. To test the hypothesis that the degree of leukoaraiosis was independently associated with outcome, we created several incremental multivariable logistic regression models as follows: first unadjusted (model 1); then adjusted for admission variables: age, NIHSS, atrial fibrillation, creatinine level, low-density lipoprotein cholesterol, random blood sugar (model 2); then additionally adjusted for endovascular variables: poor recanalization, time to recanalization, poor collateral grade (model 3); and finally additionally adjusted for the presence of parenchymal hemorrhage (model 4). We then repeated all analyses, entering leukoaraiosis severity, collateral grade, and degree of recanalization as ordinal variables.
Secondary Analyses.
We performed preplanned sensitivity analyses for predictors of a good (0–2 or return to baseline) versus poor (3–6) mRS at 90 days in patients who were alive by the time of discharge (n = 87). Furthermore, we compared the frequency of any improvement (defined as an improvement by ≥1 point on the mRS between discharge and 90 days) in patients with absent-to-moderate versus severe leukoaraiosis who were alive at the time of discharge. Last, we conducted multivariable linear regression analysis with backward elimination of factors independently associated with the final infarct volume. We performed multivariable logistic regression analyses (by using bootstrapping for more stable results, given the limited number) to assess whether leukoaraiosis and infarct volume were independently associated with a poor 90-day outcome.
Collinearity diagnostics were performed for all multivariable logistic and linear regression models. Associations are presented as ORs with corresponding 95% confidence intervals. The Hosmer-Lemeshow goodness-of-fit statistic was used to assess all models for final fit. Two-sided significance tests were used throughout, and a 2-sided P < .05 was considered statistically significant. All statistical analyses were performed by using SPSS Statistics 20.0.0 (IBM, Armonk, New York).
Results
During the study period, 3057 patients were admitted with a diagnosis of acute ischemic stroke. Of these, 142 patients were treated with EST. Thirteen patients were lost to follow-up. Data were complete for all included patients except for collateral grade, which could not be assessed in 8 patients due to proximal internal carotid artery occlusion and absent contralateral injection before the intervention.
Free marginal κ values for interobserver agreement indicated moderate and almost perfect agreement for graded (κ = 0.50) and dichotomized leukoaraiosis severity (κ = 0.91), respectively.13 Intraobserver agreement was substantial and almost perfect for graded (κ = 0.78) and dichotomized leukoaraiosis severity (κ = 0.89), respectively.
Factors Associated with Leukoaraiosis Severity (Unadjusted)
Baseline characteristics of the 129 included patients stratified by leukoaraiosis severity and outcome are summarized in On-line Table 1. Severe leukoaraiosis was associated with greater in-hospital mortality (P = .001), worse mRS scores at discharge (P = .003), and worse 90-day outcome (P = .001, Fig 1). Furthermore, patients with severe leukoaraiosis were more likely to have experienced a prior stroke or TIA (P = .002), atrial fibrillation (P = .001), coronary artery disease (P = .030), or peripheral vascular disease (P = .009), were older (P < .001), less frequently underwent mechanical thrombectomy, and had more frequent cardioembolic strokes (P = .005) and strokes of other or undetermined pathogenesis (P = .039).
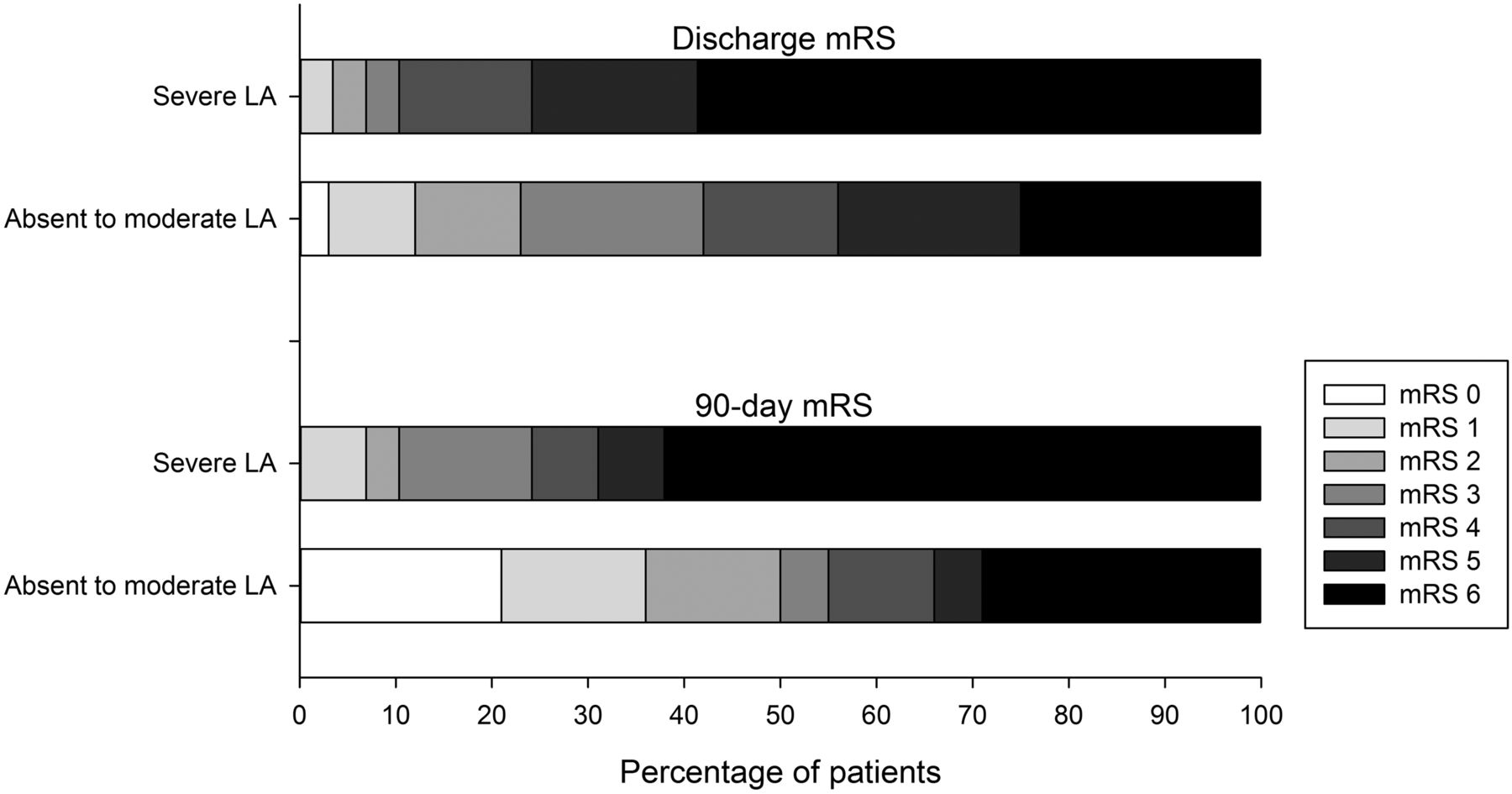
Functional outcome at discharge and at 3 months according to leukoaraiosis (LA) severity (unadjusted). Scores of ≤2 or return to baseline on the mRS are considered a good outcome (darker shades indicate worse outcomes).
There was a weak inverse relation between leukoaraiosis and collateral grade (ie, patients with worse leukoaraiosis had better collaterals; graded: r = −.218, P = .016; dichotomized: r = −.265, P = .003). There was no association between the severity of leukoaraiosis and the degree of recanalization (graded: r = 0.083, P = .351; dichotomized: r = 0.029, P = .743).
Factors Associated with a Poor 90-Day Outcome (Unadjusted)
Poor 90-day outcome (On-line Table 2) was associated with older age (P < .001) and worse leukoaraiosis (graded: P = .005; dichotomized: P < .001) and higher admission NIHSS scores (P < .001), glucose levels (P = .032), creatinine levels (P = .02), and low-density lipoprotein levels (P = .031), good recanalization (P = .023), the presence of atrial fibrillation (P = .014), and the presence of parenchymal hemorrhage16 (parenchymal hemorrhage 1 and parenchymal hemorrhage 2, P = .001). The association between leukoaraiosis severity and 90-day outcome was similar across the endovascular modalities used (On-line Fig 2).
Primary Analysis: Multivariable Analysis of Factors Associated with the 90-Day Outcome
The association between severe leukoaraiosis and poor 90-day outcome remained after adjusting for pertinent covariates (Table). The association of leukoaraiosis with outcome remained when leukoaraiosis severity, degree of recanalization, and collateral grade were entered as ordinal variables in all models (P < .01, not shown).
Multivariable logistic regression analysis of factors independently associated with a poor 90-day outcome
Secondary Analyses
Association between Leukoaraiosis and Outcome among Patients Alive at Discharge.
By the time of discharge, 33% (n = 42) of patients had died (Fig 1, all because of “withdrawal of care”). To gain a better understanding of whether leukoaraiosis can serve as a useful independent prognostic factor for outcome in patients who did not have early withdrawal of care (which may be related to factors independent of measured patient characteristics), we then repeated the logistic regression analyses in patients who were alive by discharge (n = 87). These analyses yielded similar results, showing an independent association between severe leukoaraiosis and poor outcome (unadjusted P = .001; adjusted P < .05, not shown).
Association between Leukoaraiosis and Recovery among Patients Alive at Discharge.
Among patients who were alive at discharge, those with severe leukoaraiosis had significantly less frequent improvement on the mRS from discharge to 90 days compared with patients with absent-to-moderate leukoaraiosis (OR, 3.69; 95% CI, 1.05–12.99; P = .034; Fig 2). Given the limited number of subjects in the outcome category, multivariable analysis to adjust for covariates was not attempted.

Functional improvement of patients who were alive at the time of discharge (n = 87) according to leukoaraiosis severity (unadjusted). Compared with patients with absent-to-moderate leukoaraiosis, patients with severe leukoaraiosis are significantly less likely to have any improvement on the mRS from discharge to 90 days (50% versus 79% of surviving patients [21% versus 59% of all patients, respectively]; P = .034; darker shades indicate less improvement).
Association among Infarct Volume, Leukoaraiosis, and Outcome.
Among patients with follow-up imaging (n = 68), those with severe leukoaraiosis (n = 11) had significantly larger infarcts compared with patients with absent-to-moderate leukoaraiosis (152 ± 145 mL versus 51 ± 68 mL, P = .044). Patients with a poor outcome (n = 29) had significantly larger infarcts compared with patients with a good outcome (131 ± 111 mL versus 20 ± 16 mL, P < .001). Multivariable linear regression analysis (including age, admission NIHSS, leukoaraiosis, time to recanalization, degree of recanalization, collateral grade, random blood sugar, atrial fibrillation, use of antihypertensive medications, and glycated hemoglobin) indicated that leukoaraiosis (P < .001), degree of recanalization (P < .001), and age (P = .036) were independently associated with the final infarct volume (not shown). Last, multivariable logistic regression (including age, leukoaraiosis, infarct volume, and admission NIHSS score) indicated that severe leukoaraiosis (P = .035), infarct volume (P = .006), and age (P = .004) were independently associated with a poor outcome (not shown).
Discussion
We demonstrate that pre-existing leukoaraiosis severity is associated with a poor 90-day outcome after EST, independent of established predictors of stroke outcome.
This finding is important because translating favorable angiographic results of endovascular treatment to correspondingly robust clinical outcomes is needed. Because endovascular approaches to acute ischemic stroke treatment are increasingly offered to older patients, despite a higher risk of poor outcome compared with younger patients,12 appropriate patient selection beyond procedural aspects represents an important goal in this population.
Imaging biomarkers are of particular interest, given that neuroimaging is a prerequisite to patient selection for acute therapy. Leukoaraiosis may represent a viable biomarker because it can be determined by standard neuroimaging and has been consistently shown to predict a higher risk for poor poststroke outcome.5⇓⇓–8,15,18
How leukoaraiosis contributes to worse poststroke outcomes is incompletely understood. For example, leukoaraiosis has been associated with a greater risk for parenchymal hemorrhage after EST, which is a predictor of poor poststroke outcome.4 However, in the current study, we did not note a significant association between leukoaraiosis and parenchymal hemorrhage risk, possibly because we included patients treated with newer generation devices, which may have a lower risk for hemorrhagic transformation19 and our study was likely underpowered to detect a significant association. Although our results are consistent with a retrospective analysis of patients treated with EST,5 further research is required to elucidate the potential association between leukoaraiosis and the risk for hemorrhagic transformation in this patient population.
An alternate explanation for poor outcomes in patients with leukoaraiosis may be chronic cerebral hypoperfusion that results in reduced cerebral ischemic resilience and thus greater final lesion volumes,20 which are a known outcome predictor after EST.21 Indeed, we and others have previously shown that leukoaraiosis severity is associated with a larger ischemic core, mismatch lost, and final infarct volume, supporting this hypothesis.13,15,22 Indeed, subgroup analyses in patients with available follow-up imaging indicated that worse leukoaraiosis independently predicted larger infarct volumes. However, because infarct volumes could not be measured in all patients, additional studies are required to confirm the association among leukoaraiosis, infarct volume, and outcome. Furthermore, because the impact of leukoaraiosis on poststroke outcome was only partially explained by larger infarct extent in this and prior studies,18 it appears likely that the loss of compensatory network integrity results in decreased cerebral plasticity. For example, decreased integrity of fiber tracts within the unaffected hemisphere and purported compensatory pathways (such as the corticorubrospinal system) have been shown to impair poststroke recovery.23,24 Accordingly, global white matter changes such as those caused by leukoaraiosis are expected to adversely affect the potential for poststroke recovery. However, although several studies have linked leukoaraiosis to poor functional outcomes, there is a paucity of data regarding the degree of poststroke recovery, particularly in patients with large-artery occlusion.25⇓–27
In this respect, our observation of significantly decreased long-term recovery in patients having undergone EST with severe leukoaraiosis is a novel and important finding, supporting the hypothesis that leukoaraiosis disrupts cerebral connectivity and plasticity. Considering that most patients undergoing EST have early functional deficits,3 it is critical to understand factors that modulate recovery. Our findings highlight the clinical importance of investigating leukoaraiosis in patients with stroke to better understand its predictive value for functional recovery after stroke.
The strengths of the present study relate to the relatively large sample size, a well-defined patient population, investigation of variables that have been associated with poststroke outcome, and blinded imaging assessment. Our study has limitations related to its retrospective design and should be considered hypothesis-generating. EST was not standardized across patients, and most patients were treated with multiple modalities with or without rtPA. For this reason, it was not feasible to adjust our analysis to account for the various treatment approaches or perform subgroup analyses. Nevertheless, exploratory analysis indicated a similar association across treatment modalities. This finding is consistent with the presumed pathophysiology and described association with poor poststroke outcomes in numerous studies across heterogeneous patient populations, allowing better generalization of our results.4,8,18 Misclassification of leukoaraiosis severity is possible given the CT-based grading system. However, although MR imaging has a higher sensitivity and specificity to research leukoaraiosis compared with CT,14 the latter is more broadly available and routinely used in the hyperacute setting to evaluate patients with stroke. Furthermore, as noted, the classification used in our study is easy to perform, had a high inter- and intraobserver agreement, and does not require extensive postprocessing.8,13 Last, although our data show a strong association between leukoaraiosis and outcome, a causal relationship remains to be fully established.
Conclusions
In summary, with a projected increase in the occurrence of strokes, especially among the elderly,9⇓–11 clinicians will be increasingly12 faced with the issue of appropriately selecting elderly patients with severe strokes for EST. Our data provide preliminary evidence that patients with severe pre-existing leukoaraiosis are at high risk for a poor functional outcome after EST. Given absent association with parenchymal hemorrhage and favorable outcome in a small subset of patients, the presence of severe leukoaraiosis currently does not justify exclusion from EST. Nevertheless, these results highlight the need to further explore leukoaraiosis as a promising surrogate marker for poor outcome after EST to improve risk assessment and aid in discussing expectations of different outcome types with family members. Further study is required to confirm our findings and investigate underlying mechanisms.
Footnotes
Disclosures: Muhib A. Khan—UNRELATED: Payment for Development of Educational Presentations: Cyberrounds, for the development of a Continuing Medical Education on atrial fibrillation and newer oral anticoagulants.
References
- Received March 27, 2014.
- Accepted after revision May 12, 2014.
- © 2014 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The whole day matters after stroke: Study protocol for a randomized controlled trial investigating the effect of a 'sit less, move more, sleep better program early after stroke
- Leukoaraiosis and acute ischemic stroke: 90-day clinical outcome following endovascular recanalization, with proposed "L-ASPECTS"
- Association of White Matter Lesions and Outcome After Endovascular Stroke Treatment
- Relationship of white matter lesion severity with early and late outcomes after mechanical thrombectomy for large vessel stroke
- White Matter Disease and Outcomes of Mechanical Thrombectomy for Acute Ischemic Stroke
- White matter hyperintensity burden in patients with ischemic stroke treated with thrombectomy
- Leukoaraiosis severity and outcomes after mechanical thrombectomy with stent-retriever devices in acute ischemic stroke
- Leukoaraiosis Attenuates Diagnostic Accuracy of Large-Vessel Occlusion Scales
- Endovascular treatment of acute ischemic stroke in nonagenarians compared with younger patients in a multicenter cohort
- Leukoaraiosis, intracerebral hemorrhage, and functional outcome after acute stroke thrombolysis
- Impact of Leukoaraiosis Burden on Hemispheric Lateralization of the National Institutes of Health Stroke Scale Deficit in Acute Ischemic Stroke
- Response to Letter Regarding Article, "Leukoaraiosis Burden Significantly Modulates the Association Between Infarct Volume and National Institutes of Health Stroke Scale in Ischemic Stroke"
- Cerebral Computed Tomography-Graded White Matter Lesions Are Associated With Worse Outcome After Thrombolysis in Patients With Stroke