
Abstract
SUMMARY: Cosmetic rhinoplasty encompasses a diverse group of procedures, including alteration of the radix, nasal dorsum, nasal tip, and nasal base; premaxillary augmentation; septoplasty; and combinations thereof. Similarly, many different types of grafts and alloplastic materials can be used in cosmetic rhinoplasty, such as cartilage, bone, silicone, porous polyethylene, expanded polytetrafluoroethylene, and calcium hydroxylapatite. Complications of rhinoplasty that can be observed on imaging include retained metallic surgical instrument fragments, infection, implant extrusion, nerve impingement by implants, nasal valve collapse, and implant deformity. Knowledge of the basic surgical procedures and potential complications of cosmetic rhinoplasty is important for adequately interpreting postoperative radiologic imaging studies.
ABBREVIATION:
- K-wires
- Kirschner wires
Cosmetic rhinoplasty consists of surgically modifying portions of the nose to ameliorate its appearance, while maintaining its function. The procedure is the second most commonly performed cosmetic surgery, with 243,772 cases recorded in 2011 in the United States.1 Thus, it is not uncommon to encounter the sequelae of rhinoplasty on head and neck imaging. The imaging characteristics of the different types of rhinoplasty, augmentation materials, and associated complications are reviewed.
Types of Surgery
Rhinoplasty can be performed for cosmetic or functional purposes. The surgery can be classified as primary (performed for the first time) or secondary (revision), in which patients return for additional surgery to address over-resection, under-resection, delayed effects of shrink-wrapping, functional problems, and other complications.2⇓⇓–5 Furthermore, rhinoplasty can be performed via external (open) or endonasal (closed) approaches. Ultimately, rhinoplasty encompasses a diverse group of procedures, including the following types of techniques:
Radix modification consists of reduction versus augmentation (Fig 1). The radix is typically altered in harmony with the nasal dorsum and tip. A rasp or osteotome can be used for reduction, while various implants and grafts can be used for augmentation.2,6
Nasal dorsum surgery consists of dorsal hump reduction versus augmentation. Reduction surgery consists of excising excess osteocartilaginous septum by using a rasp or chisel.2,7 The resected tissue can sometimes then be used as a columella strut, tip graft, or for radix augmentation.2 On the other hand, augmentation can be performed with autografts or alloplastic implants (Fig 2).
Tip modification procedures include elevation by using a columellar strut, shield or tip grafts, volume reduction via cartilage trimming, and altering the definition and projection (Fig 3).7
Nasal base surgery includes narrowing the wide columella, wedge resection, nostril sill resection, rim excision, alar reshaping with a graft, and columella excision or grafting.2 Augmentation of the columella is often performed in conjunction with nasal dorsum augmentation and can be accomplished by using L-strut implants (Fig. 4)
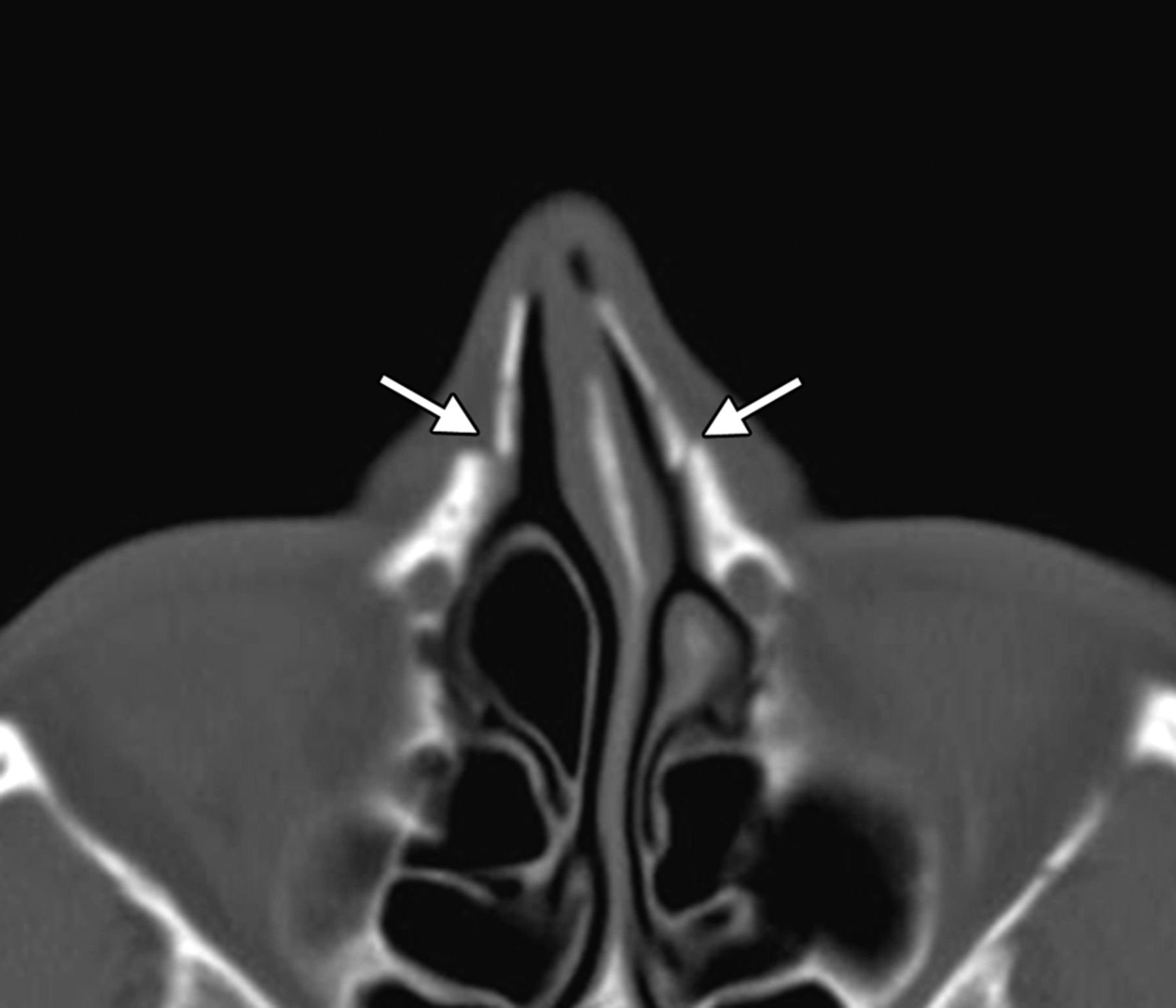
Lateral osteotomy consists of creating fractures of the nasal processes of the maxillae and shifting the lateral nasal walls to narrow a wide nose, widen a narrow bony pyramid, straighten a deviated nose, and close an open roof deformity.8 The osteotomy sites are initially visible on CT as radiolucent defects and perhaps mild displacement of the nasal processes (Fig 5). Osteotomies are sometimes performed as a greenstick-type fracture, resulting in stable bone stumps.9 The osteotomies generally heal by 6 months, and remodeling can be observed on CT.10
Premaxillary augmentation can be performed as an adjunct to rhinoplasty to treat an excessively deep infranasal sulcus (premaxillary underprojection) and acute nasolabial angle. This can be accomplished by using autografts of implants positioned in the midline just inferior to the anterior nasal spine of the maxilla (Fig 6).11,12 The implants can have a linear or bat-wing configuration.12

Radix implant. Axial CT image shows a bone graft positioned at the level of the nasal radix, secured by a metal plate and screws (arrow).

Dorsal nasal implant. Sagittal CT image shows a hyperattenuated expanded polytetrafluoroethylene nasal dorsum implant (arrow).

Tip augmentation with a columellar strut graft. Axial (A) and sagittal (B) CT images show hyperattenuated grafts within the infratip lobule and columella (arrows).

Silicone L-strut implant. Sagittal CT image shows the hyperattenuated L-shaped Silicone implant extending from the nasal dorsum to the columella.

Lateral osteotomy. Axial CT image shows defects in the bilateral nasal processes of the maxillae (arrows). The lateral nasal walls are displaced medially (in-fractures).

Premaxillary implant. Axial (A) and coronal (B) CT images show a hyperattenuated strip of silicone (arrows) positioned in the midline anterior to the nasal spine of the maxilla.
Rhinoplasty can also be performed in conjunction with septoplasty for correcting concurrent nasal septal deviation (septorhinoplasty) and other cosmetic facial interventions to optimize esthetic balance.13 Septoplasty usually appears as a straight and thin septum without spurs on imaging (Fig 7).

Septorhinoplasty. Axial CT image shows a very straight and thin nasal septum (arrowheads). A bone graft is present within the nasal dorsum (arrow).
Types of Graft and Implant Materials
A variety of materials are available for rhinoplasty, including autografts and alloplastic materials. Graft materials include bone and cartilage, which can be harvested from septal cartilage, auricular conchal cartilage, costal cartilage, calvarial bone, iliac crest bone, and costal bone and acellular dermal graft (AlloDerm; BioHorizons, Birmingham Alabama).14⇓⇓–17 “Turkish Delight ” is a unique graft composed of diced cartilage mixed with a small amount of blood and wrapped in Surgicel (Ethicon, Raleigh North Carolina).18 Overgrafting is often intentionally performed with certain graft materials, especially AlloDerm, to compensate for eventual resorption and atrophy.14 However, cartilage transplanted with perichondrium has been shown to induce growth of new cartilage or bone.19 On CT, cartilage appears as soft-tissue attenuation, though calcification or ossification may form, rendering the graft hyperattenuated.20 The cortex of bone grafts is hyperattenuated on CT, though the size and attenuation can diminish with time with resorption of the graft.20 Bone grafts may contain marrow elements, which have soft-tissue attenuation on CT and can display fat signal characteristics on MR imaging.20
Alloplastic implants used in facial cosmetic surgery include silicone (Silastic; Dow Corning, Auburn, Michigan), polyamide mesh (Supramid; S. Jackson, Alexandria, Virginia), polyethylene tetraphthalate mesh (Mersilene; Ethicon), expanded polytetrafluoroethylene (Gore-Tex; W.L. Gore & Associates, Newark, Delaware), and high-attenuation porous polyethylene (Medpor; Stryker, Mahwah, New Jersey).14,21⇓⇓⇓–25 Silicone and expanded polytetrafluoroethylene are similarly hyperattenuating, intermediate in attenuation between soft tissue and bone.20 On the other hand, high-attenuation porous polyethylene is hypoattenuating with attenuation intermediate between soft tissue and fat, and it has intermediate signal on T1 and T2 MR imaging sequences.20 The material can appear to enhance due to fibrovascular in-growth.
Filler agents, such as calcium hydroxylapatite (Radiesse; Merz Aesthetics, San Mateo, California), can be used for minimally invasive cosmetic rhinoplasty or to modify prior rhinoplasty.26,27 The fillers can be injected by using a linear, threading, fanning, or cross-hatching technique.27 Calcium hydroxylapatite displays high attenuation on CT (Fig 8).28

Rhinoplasty with filler. Axial (A) and coronal (B) CT images show hyperattenuated hydroxylapatite filler (arrows) to the right of the Silastic nasal dorsum implant. Note the deviated nasal septum.
Metallic Kirschner wires can be used for restoration of an impacted nasal pyramid, fixation of intraoperative nasal septum fractures, and stabilization of costal cartilage grafts.29⇓–31 K-wires can be implanted in the nasal dorsum, columella, or both because in an L-strut configuration, a wire is positioned along the dorsum (Fig 9). The columellar K-wires are typically inserted into a maxillary drill hole in the area of the nasal spine, adjacent to the incisive canal.

Kirschner wire strut. Axial (A) and coronal (B) CT images show a metallic wire (arrow) extending along the nasal dorsum and nasal base, where it inserts into the maxilla, lateral to the incisive canal.
Complications
Complications of rhinoplasty that can be found on imaging include retained metallic surgical instrument fragments, infection, implant extrusion, cranial nerve impingement by implants, nasal valve collapse, and implant deformity.21
Surgical paraphernalia used in rhinoplasty are rarely retained during surgery. This can occur, for instance, as a result of osteotome breakage during nasal osteotomy, leaving behind a fragment that can be difficult to find intraoperatively. However, radiographs can readily confirm and localize retained metallic foreign bodies (Fig 10).

Retained osteotome fragment. Frontal (A) and lateral (B) radiographs show the retained metallic fragment (arrows) at the left lateral osteotomy site. Note the nasal-tip bone graft.
Infection is the most common objective complication of rhinoplasty and can occur early or late postoperatively.32 This complication is more common with alloplastic implants than autografts.14 The postoperative infections most often remain localized to the skin and subcutaneous tissues of the nose but occasionally extend intracranially or result in generalized septicemia.32 MR imaging or CT can be used to delineate the extent of infections, which can appear as fluid collections, sclerosis and enhancement of osseous structures, and soft-tissue inflammatory changes (Fig 11). Infection predisposes to skin ulceration and implant extrusion (Fig 12).33,34

Implant infection. Sagittal postcontrast CT image shows a small fluid collection and associated inflammatory changes (arrow) in the nasal dorsum surrounding the implant.

Implant extrusion. Sagittal CT image shows a porous polyethylene dorsal nasal implant (arrow) projecting through a cutaneous defect.
Lip dysesthesia can occur after certain types of rhinoplasty, but this is expected to resolve within 6 weeks without functional sequelae.35 However, inadvertent drilling and insertion of columellar K-wires into the incisive canal can lead to dysesthesia in the distribution of the nasopalatine nerve. This complication can be observed on CT (Fig 13).

Nerve impingement. The patient presented with dysesthesias in the maxillary nerve distribution after rhinoplasty. Sagittal CT image shows that the K-wire traverses the incisive canal at the expected location of the nasopalatine nerve (arrow).
Various types of deformities have been described following cosmetic rhinoplasty, including nasal valve collapse, inverted-V deformity, saddle nose deformity, open roof, stairstep deformity, hourglass deformity following dorsal hump surgery, and shrink-wrap effect of the soft tissues after nasal tip surgery.13,36⇓–38 Postoperative deformity can also result from warping of grafts, particularly undiced cartilage grafts.39 Furthermore, trauma can compromise the structural integrity and alignment of grafts and implants (Fig 14).

Deformed K-wire. The patient presented with trauma to the nose. Submentovertex radiograph shows a bend in the K-wire (arrow).
Postoperative nasal valve collapse can lead to dynamic or static obstruction and is evidenced by a decreased nasal valve angle, which is normally 10°-15°.36,38,40 The nasal valve angle can be more reliably determined on CT than via endoscopic methods (Fig 15).41 Furthermore, nasal-base-view reformatted CT images obtained in a plane perpendicular to the anterior aspect of the estimated acoustic axis are more accurate than traditional coronal CT images for measuring nasal valve angles.40 Spreader grafts and suture techniques, splay grafts, alar batten grafts, lateral crural extension grafts, and lateral alar suspension can be used to correct this deformity.13,42

Nasal valve collapse. Coronal CT image shows stenosis of the right nasal valve (arrow). The left nasal valve remains patent.
Conclusions
A wide variety of techniques and augmentation materials are used for cosmetic rhinoplasty. Familiarity with the expected alterations, and complications from rhinoplasty is essential for satisfactory interpretation of postoperative imaging.
Footnotes
Disclosures: Charles Schatz—UNRELATED: Expert Testimony: various attorneys, Comments: 2–3 times per year, no conflict of interest, Stock/Stock Options: unrelated investments/retirement plan.
Indicates open access to non-subscribers at www.ajnr.org
References
- © 2014 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.