
Abstract
BACKGROUND AND PURPOSE: The quantitative evaluation of orbital fat proliferation and edema and the assessment of extraocular muscles are useful for diagnosing and monitoring thyroid-associated orbitopathy. To evaluate therapy-induced quantitative changes in the orbital fat of patients with thyroid-associated orbitopathy, we performed volumetric and water fraction measurements by using T2-weighted FSE iterative decomposition of water and fat with echo asymmetry and least-squares estimation (FSE-IDEAL) imaging.
MATERIALS AND METHODS: Orbital FSE-IDEAL images of 30 volunteers were acquired twice within 1 week. Nine patients with thyroid-associated orbitopathy underwent FSE-IDEAL imaging before and after methylprednisolone pulse therapy, and the treatment results were assessed by using their pre- and post-methylprednisolone pulse therapy clinical activity scores. We performed volumetric and water fraction measurements of orbital fat by using FSE-IDEAL imaging and evaluated interscan differences in the volunteers. In patients with thyroid-associated orbitopathy, we compared pre- and posttherapy orbital fat measurements and assessed the correlation between the pretherapy values and clinical activity score improvement.
RESULTS: The reproducibility of results obtained by the quantitative evaluation of orbital fat in volunteers was acceptable. After methylprednisolone pulse therapy, the water fraction in the orbital fat of patients with thyroid-associated orbitopathy was significantly decreased (P < .001). There was a significant positive correlation between the pretherapy water fraction and clinical activity score improvement (right, r = 0.82; left, r = 0.79) and a significant negative correlation between the pretherapy volume and clinical activity score improvement (bilateral, r = −0.84).
CONCLUSIONS: Volumetric and water fraction measurements of orbital fat by using FSE-IDEAL imaging are feasible and useful for monitoring the effects of therapy and for predicting the response of patients with thyroid-associated orbitopathy to methylprednisolone pulse therapy.
ABBREVIATIONS:
- CAS
- clinical activity score
- FSE-IDEAL
- FSE iterative decomposition of water and fat with echo asymmetry and least-squares estimation
- MPPT
- methylprednisolone pulse therapy
- SI
- signal intensity
- TAO
- thyroid-associated orbitopathy
Thyroid-associated orbitopathy (TAO) is the most common extrathyroid manifestation of Graves disease. The enlargement of orbital fat and extraocular muscles in the relatively fixed volume space imposed by the bony orbit may produce proptosis, ocular motility loss, and decreased visual acuity.1 Histologic studies showed lymphocytic infiltration and edema due to the accumulation of hydrophilic, interstitial glycosaminoglycans in the orbital fat and extraocular muscles,2,3 attributable to antigenic cross-reactivity between thyroid proteins and orbital fibroblasts.4
The course of TAO can be divided into the active, regressing, and a burnt-out phase.5 Early active disease is treated with combined immunosuppression.6,7 The identification of patients who stand to benefit from this therapy is important but clinically difficult, despite the availability of activity scoring systems. Consequently, objective methods are needed.
CT has been used to quantify the volume of extraocular muscles and orbital fat in TAO.8⇓⇓–11 However, ocular radiation exposure limits its clinical use. Because MR imaging without ionizing radiation yields orbital images with excellent soft-tissue contrast in any plane, it has been used for evaluating TAO.12⇓⇓–15
The quantitative evaluation of the orbital fat volume on T1-weighted images was reported useful for assessing the severity of TAO and for monitoring the treatment response.12,16 Recently, Higashiyama et al17 demonstrated that after methylprednisolone pulse therapy (MPPT), the orbital fat volume was unchanged, while the total volume of extraocular muscles was decreased on T2-weighted images. However, in our search of the literature, we found no reports on quantitative changes in orbital fat edema after MPPT or orbital irradiation. Consequently, the correlation between the volume and edema of orbital fat and the treatment response of patients with TAO remains to be elucidated.
FSE iterative decomposition of water and fat with echo asymmetry and least-squares estimation (FSE-IDEAL), a novel 3-point Dixon method, is useful for separating the fat signal from the water signal18,19 but has not been used to quantify the orbital structures in TAO. To evaluate the feasibility of FSE-IDEAL imaging for the precise quantitative evaluation of orbital fat, we subjected healthy volunteers to 2 FSE-IDEAL imaging studies performed during 1 week. We measured the volume and the water fraction of their orbital fat and ascertained the reproducibility of the measurement results. We also acquired FSE-IDEAL images in patients with TAO to assess MPPT-induced changes in the volume and water fraction of their orbital fat and evaluated the correlation between the quantitative values of orbital fat and the improvement in their symptoms.
Materials and Methods
Subjects
This prospective study was approved by the Ethics Committee of Hiroshima University. Informed consent was obtained from all participants before entry into the study.
We recruited 30 healthy volunteers (15 men, 15 women; median age, 29 ± 7.6 years). They underwent orbital FSE-IDEAL imaging twice within 1 week to evaluate the reproducibility of the water fraction and the volume measurements of the orbital fat.
We also recruited 16 patients older than 20 years of age who had a clinical diagnosis of TAO between December 2013 and November 2015. The recorded activity of their TAO was based on their clinical activity score (CAS), including pain, eyelid erythema or edema, conjunctival hyperemia and chemosis, and a swollen caruncle.20 All 16 patients underwent orbital FSE-IDEAL imaging. Two of them underwent local injection of triamcinolone acetonide into the orbit, and 5 of them followed a conservative wait-and-see approach because their TAO was slight and the risk of MPPT would exceed the benefit. Consequently, the 9 patients (2 men, 7 women; median age, 57 ± 12.5 years; 18 eyes) who received MPPT (500 mg of methylprednisolone administered intravenously once a day for 3 consecutive days) were included in this study and underwent FSE-IDEAL imaging again 1.6 ± 0.7 months thereafter. Re-evaluation of the TAO activity was based on the latest CAS obtained around the time of the second MR imaging study (the interval, 1–15 days; median, 6.5 days).
MR Imaging
All images were acquired on a 3T scanner (Signa Excite HD 3.0; GE Healthcare, Milwaukee, Wisconsin; gradient strength, 40 mT/m; slew rate, 150 T/m/s) by using an 8-channel phased array brain coil. We optimized the T2-weighted FSE-IDEAL sequence (TR/TE, 6000/100 ms; flip angle, 90°; image matrix, 288 × 160; FOV, 160 × 160 mm; section thickness/gap, 2/0 mm; asymmetric echo shifts, −π/6, π/2, 7π/6; number of acquisitions, 3; number of sections, 32; scan time, 2 minutes 42 seconds) and obtained orbital water and fat images for all subjects.
Orbital Fat Water Fraction and Volume Measurements
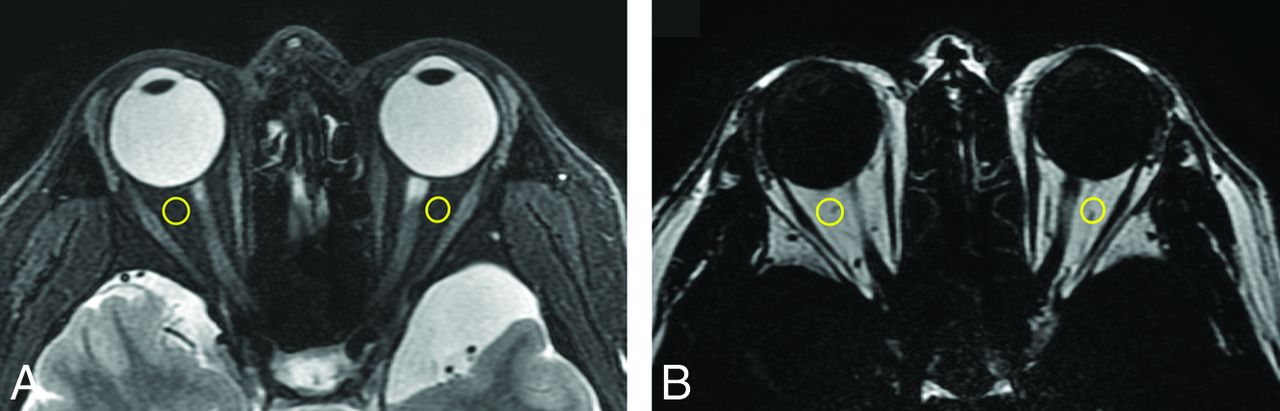
We placed an ROI in the orbital fat on FSE-IDEAL images of water and fat and measured the average signal intensity (SI) in the ROIs. Next, we defined and calculated the water fraction of the orbital fat as [SI Water / (SI Water + SI Fat)] to assess the orbital fat edema on the basis of the fat fraction (SI Fat / [SI Water + SI Fat]),18 defined to quantify fatty infiltration (Fig 1). The orbital fat volume of both eyes was measured on a workstation (Virtual Place Raijin; AZE Ltd, Tokyo, Japan). We first separated fat tissue from other structures by using the threshold value, recorded as the mean value between the average SI plus the SD of the ROI in the internal rectus muscle and the average SI minus the SD of the ROI in the orbital fat, considering some dispersion of signal intensities in the ROIs. Then we manually removed the fatty marrow of the orbital bone and outer fat; the orbital fat volume was automatically measured on the workstation (Fig 2).

Axial water (A) and fat (B) images of a healthy volunteer. The ROIs are encircled in yellow.

Axial fat image (A) of a healthy volunteer. The selected orbital fat is light green. We separated fat tissue by using an adequate signal-intensity threshold and manually removed extraorbital fat. In this volunteer, the internal rectus muscle showed an average SI of 207 and an SD of 112, whereas the orbital fat showed an average SI of 1636 and an SD of 88. Therefore the threshold value was [(207 + 112) + (1636 − 88) / 2 = 933]. Using FSE-IDEAL images, we then produced 3D reconstruction images of the bilateral orbital fat (B) and measured the orbital fat volume on a workstation.
Statistical Analyses
All statistical analyses were performed with commercially available software (XLSTAT, version 2015.6.01.244, Addinsoft; https://www.xlstat.com/en/company/about-us) and Excel 2010 (Microsoft, Redmond, Washington).
We used Bland-Altman analysis and the Pearson correlation coefficient to evaluate interscan differences in the volunteers and used the mean value of the water fraction and the volume of the bilateral orbit in our analyses.
In patients with TAO, we performed paired-sample t tests to compare the water fraction and the volume of orbital fat before and after MPPT. The right and left orbits were examined separately because patients with unilateral TAO manifested unilateral excess fat exophthalmos.10 To ascertain that the values obtained before and after treatment were significantly different, we applied the 2-sample t test to compare the therapy-induced changes with the values obtained in the volunteers. We defined the therapeutic effect of MPPT as the following formula: [CAS Improvement Ratio = (Pretherapy CAS − Posttherapy CAS) / Pretherapy CAS)] and determined the correlation between the measured values before MPPT and the CAS improvement ratio with the Pearson correlation coefficient test. Differences of P < .05 were considered statistically significant.
Results
Volunteers
The difference in the water fraction and the volume of orbital fat on the first and second scans was 1.1% ± 11.9% and 0.5% ± 3.6%, respectively. Bland-Altman analysis of the measurement results showed that their reproducibility was adequate (water fraction: r = 0.71, bias = −0.002; 95% CI bias, −0.012–0.007; 95% CI, −0.052–0.047; volume: r = 0.99, bias = −0.066; 95% CI bias, −0.235–0.102; 95% CI, −0.951–0.819) (Fig 3).

Bland-Altman analysis confirming the interscan reproducibility of the water fraction (A) and the volume of orbital fat (B) on FSE-IDEAL images of the volunteers.
Patients
The clinical characteristics of the 9 patients with TAO are summarized in the Table. After MPPT, the water fraction in the orbital fat on both sides was significantly decreased (right, 12.4% ± 3.8%, P < .001; left, 13.6% ± 6.5%, P < .001; Fig 4A). The treatment-induced reduction in the water fraction was significantly larger than the interscan difference observed in the volunteers (right, P = .002; left, P = .001). There was no significant difference in the orbital fat volume pre- and posttreatment (right, 2.0% ± 7.8%, P = .37; left, 1.9% ± 3.8%, P = .17, Fig 4B).
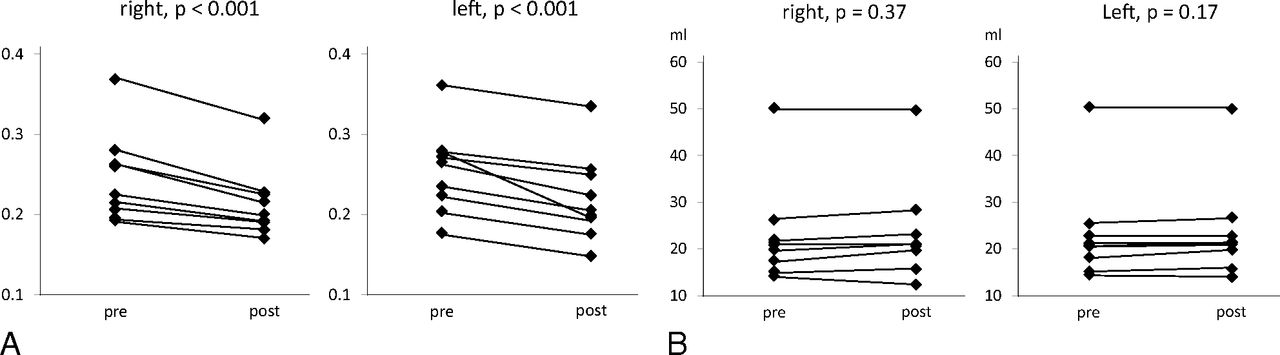
Comparison of the pre- and posttreatment water fraction (A) and the volume of orbital fat (B) in patients with TAO. Methylprednisolone pulse therapy significantly decreased the water fraction. The volume was unchanged.
Patient profiles
The pre- and posttreatment CAS fell by 3 points in 2 patients, by 2 points in 1 patient, and by 1 point in 3 patients. In the other 3, there was no change. The positive correlation between the pretreatment water fraction and the CAS improvement rate (right, r = 0.82, P = .007; left, r = 0.79, P = .012) showed that the higher the pretreatment water fraction, the greater was the posttreatment CAS improvement. On the other hand, there was a negative correlation between the fat volume and CAS improvement (right, r = −0.84, P = .005; left, r = −0.84, P = .005), indicating that the larger the pretreatment orbital fat volume, the lower the posttreatment CAS improvement rate.
Discussion
To the best of our knowledge, this is the first quantitative evaluation of orbital fat by using FSE-IDEAL imaging. We document an MPPT-induced reduction in the water fraction of orbital fat in patients with TAO and report the positive correlation between the pretreatment water fraction and the CAS improvement rate and the negative correlation between the pretreatment orbital fat volume and the CAS improvement rate.
We used FSE-IDEAL imaging to acquire axial images of the bilateral orbits and measured the water fraction and the volume of orbital fat in healthy volunteers and patients with TAO. Although many images contained motion artifacts due to voluntary and involuntary eye movements, it was possible to differentiate the SI of orbital fat and other intraorbital structures by applying an adequate threshold in the orbital fat volumetry. To measure the water fraction in orbital fat, we placed ROIs on the intraorbital fat; measurement of the SI was not hampered by motion artifacts. The reproducibility of water fraction and fat volume measurements on all iteratively acquired FSE-IDEAL images was sufficient.
Others12,21 used a 1.5T MR imaging scanner and a receiver surface coil to measure orbital fat volumes. Although surface coils can yield orbital images with high spatial resolution, the signal strength decreases as the distance from the coil increases. Our use of a 3T MR imaging scanner and an 8-channel brain coil resulted in orbital images with a high enough signal-to-noise ratio for the estimation of the orbital fat volume and the water fraction.
Orbital images with high spatial and temporal resolution and fewer motion artifacts due to eye movement can be acquired on multidetector row CT scanners.11 However, the low soft-tissue contrast on multidetector row CT images makes it difficult to separate out orbital fat. In addition, ocular radiation exposure is a serious concern. Therefore, MR imaging with high soft-tissue contrast is safer for orbital imaging.
We found that MPPT reduced the water fraction in the orbital fat of patients with TAO, possibly because it decreased the severity of edema. Earlier studies7,22⇓⇓–25 reported that the SI of extraocular muscles on short τ inversion recovery sequences correlated well with the disease activity assessed with clinical methods. The correlation was maintained as disease activity changed. Although the reversibility of the relaxation time in muscles with prolonged T2 values was explained as a therapy-induced decrease in the water content,8 treatment-induced changes in orbital fat have not been documented.
Like Higashiyama et al,17 we detected no significant difference in the pre- and posttreatment orbital fat volume. Others26⇓–28 found no difference in the degree of exophthalmos, which is related to an increase in orbital fat, in patients with TAO who had undergone MPPT. Expansion of the adipose tissue volume is elicited by glycosaminoglycan-related edema and the emergence of a population of newly differentiated fat cells in these tissues.29 Although MPPT can reduce orbital fat edema, the increase in the number of fat cells may persist after therapy.
In Japan, MPPT is generally applied in patients with TAO with low CAS scores because the Japanese patients with TAO often have orbital inflammation despite low CAS scores.30 We found that the higher the pretreatment water fraction, the greater the posttreatment decrease in the CAS, despite the low pretreatment CAS scores of our study patients. An increase in the water fraction is indicative of an increase in the tissue water content and may reflect acute inflammatory changes. Earlier studies on extraocular muscles found a correlation between the SI increase on pretreatment STIR images and a good therapeutic response31⇓–33 and between prolonged pretreatment T2 values and a good response to systemic corticosteroids or orbital radiation therapy.33 These findings indicate that treatment at an early and immunologically active stage of orbitopathy is important.11,34,35 Our quantitative MR imaging study by using the FSE-IDEAL sequence showed that MPPT was useful in patients with TAO whose orbital fat contained an elevated water fraction. On the other hand, the larger the pretreatment orbital fat volume, the lower the posttreatment CAS improvement rate. Because a longer duration of TAO is associated with a larger orbital fat mass and fibrosis,36 we think that a response to steroids is less likely when the disease is in its late, inactive stage with more fibrosis.33,34
Our study has several limitations. The number of patients with TAO who underwent MPPT was small, and the lack of age-matched controls limits the comparison between patients with TAO and healthy individuals. In addition, we used the T2-weighted FSE-IDEAL sequence provided by GE Healthcare. It is a novel, 3-point Dixon method that applies iterative algorithms and the region-growing technique to estimate local field inhomogeneities.37⇓–39 Application of the 3-point Dixon method developed by different vendors may result in significantly different measurement results with respect to the water fraction of orbital fat. In addition, the demarcation between orbital and upper or lower eyelid fat is ambiguous, and this feature may introduce some interobserver variability in the orbital fat volume. Last, the correct cutoff value for the water fraction and the volume of the orbital fat between patients with TAO and their controls remains to be determined.
Conclusions
The estimation of the water fraction and the volume of orbital fat on FSE-IDEAL images is feasible, and the reproducibility of these measurements is adequate. FSE-IDEAL imaging is useful for monitoring the effects of therapy and for predicting the response of patients with TAO to methylprednisolone pulse therapy.
Footnotes
Disclosures: Kazuo Awai—UNRELATED: Consultancy: GE Healthcare; Grants/Grants Pending: Toshiba Medical Systems,* Hitachi Medical Corporation,* Bayer Yakuhin,* Eizai,* Daiichi Sankyo,* Comments: research grants. *Money paid to the institution.
References
- Received January 28, 2016.
- Accepted after revision May 8, 2016.
- © 2016 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.