
Abstract
SUMMARY: Variations in cerebral venous development can influence the ability to regulate drainage. In cerebral sinovenous thrombosis, these variations can be associated with elevated intracranial pressure. We present a series of pediatric patients with unilateral cerebral sinovenous thrombosis and investigate whether the contralateral venous sinus size increases the risk of developing elevated intracranial pressure. Patients diagnosed with a unilateral cerebral sinovenous thrombosis were identified by querying our institutional radiology data base. The difference in the occurrence of elevated intracranial pressure in patients with cerebral sinovenous thrombosis with and without hypoplastic venous sinuses was studied. Twelve cases of unilateral cerebral sinovenous thrombosis met the inclusion criteria and had sufficient images. Six patients had hypoplastic contralateral venous sinuses. The presence of hypoplastic contralateral venous sinus in the setting of thrombosis of a dominant sinus was associated with elevation of intracranial pressure (83% versus 0%, P = .015). Patients with cerebral sinovenous thrombosis and contralateral hypoplastic venous sinuses are at higher risk of developing elevated ICP and may benefit from screening with an ophthalmologic examination.
ABBREVIATIONS:
- CSVT
- cerebral sinovenous thrombosis
- ICP
- intracranial pressure
Cerebral sinovenous thrombosis (CSVT) affects 0.34–0.67 per 100,000 children annually.1 Mortality rates are 3%–12%,1 and neurologic sequelae can be seen in 22%–50% of survivors.2 The etiology is multifactorial and frequently includes acute provoking illnesses such as head and neck infections, dehydration, central venous lines, chronic medical conditions, prothrombotic states, and head trauma.1 The clinical presentation of pediatric CSVT is highly variable and includes headache, papilledema, seizures, and focal neurologic deficits.3 Diagnostic evaluation of pediatric CSVT almost invariably includes brain imaging with CT, possibly along with CTV or MR imaging with MRV.
Anatomic variations in cerebral venous development exist, which may influence the ability to appropriately regulate venous drainage from the head and subsequently increase the risk of developing elevated intracranial pressure (ICP), especially in patients with CSVT. Recognizing these anatomic variations may be important when determining treatment and monitoring protocols for children with CSVT.3 We present a series of pediatric patients with unilateral CSVT involving the transverse/sigmoid sinuses and jugular vein and the influence of an anatomic variation (ie, the structure of the unaffected contralateral venous sinus) on the elevation of intracranial pressure and clinical outcome.
Materials and Methods
Our institutional radiology data base was queried from 2010 to 2015 by using the search terms “venous sinus thrombus,” “venous thrombosis,” and “venous thrombus.” All reports of cranial imaging positive for one of these terms were reviewed. Reports with a unilateral transverse and/or sigmoid sinus thrombus were included. One hundred one patients were identified. Infants younger than 28 days, patients with a Glasgow Coma Scale score of <10, and fetuses were excluded. Additionally, patients with other potential causes of increased ICP such as intracranial mass lesions or hemorrhage with mass effect were excluded. Twelve patients were identified for this study. Clinical and radiologic data were extracted from the electronic health record to investigate basic demographic data, location of the CSVT, and size of the affected side in proportion to the unaffected side as well as the presence of elevated ICP. Outcomes were determined from clinic notes and imaging performed 3–6 months after hospitalization.
For each patient, the cross-sectional area of both transverse sinuses was measured on sagittal images in a plane 1.5 cm lateral to the confluence of the sinuses. This distance was chosen because the transverse sinus is most nearly perpendicular to the sagittal plane in this location. An ROI was drawn around each sinus on sagittal postcontrast echo-spoiled gradient-echo images when available. When no contrast-enhanced MR imaging was available, measurements were performed on unenhanced echo-spoiled gradient-echo images or CTV images if no MR imaging was performed (Figs 1 and 2).

Method for measuring sinus cross-sectional area. Patient 8 is shown. A, Sagittal postcontrast echo-spoiled gradient-echo image of the left transverse sinus. An orange outline encloses an area of 51.3 mm2. B, The right transverse sinus cross-sectional area is 30.8 mm2. C, Coronal reformat of a postcontrast spoiled gradient-echo image. Arrow demonstrates a filling defect in the proximal left sigmoid sinus, consistent with thrombus. D, MIP image of a sagittal Inhance MRV (GE Healthcare, Milwaukee, Wisconsin). Arrow shows lack of flow in the left sigmoid sinus. The ratio of the nonthrombosed-to-thrombosed-side cross-sectional area is 0.60.
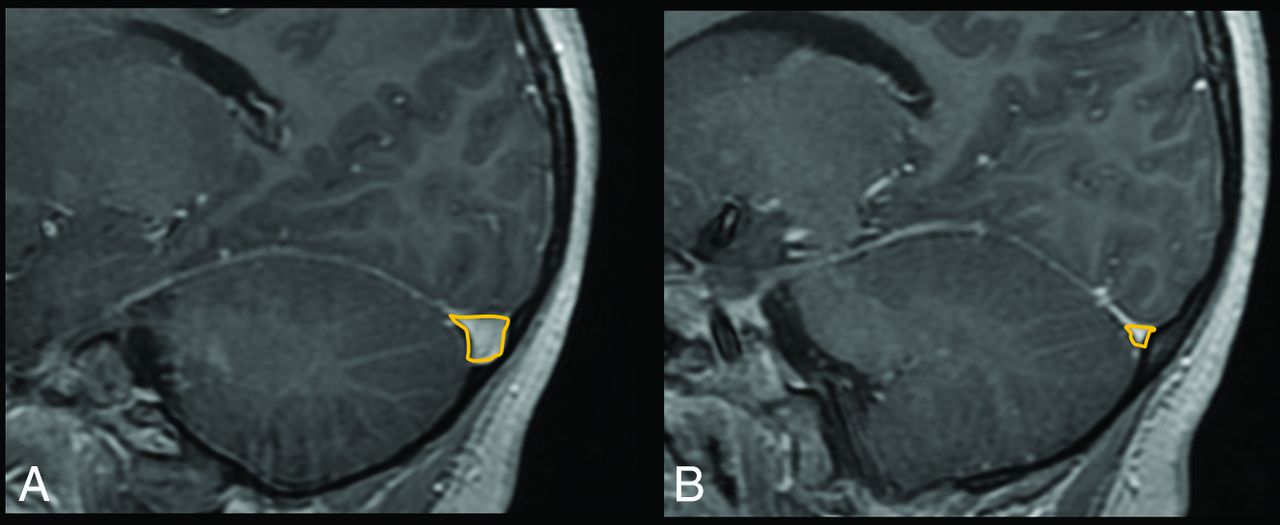
Measurements in a patient with hypoplastic right transverse sinus (patient 2). A, The left cross-sectional area is 61.1 mm2. B, The right sinus area is 6.2 mm2. The ratio is 0.10.
We defined hypoplasia of the transverse sinus when the cross-sectional area of one sinus was <50% of the area of the contralateral side. Elevated ICP was defined as the presence of symptoms such as headache, vomiting, or diplopia associated with clinical signs of elevation of ICP such as sixth cranial nerve palsy or encephalopathy. Papilledema confirmed on ophthalmologic assessment was used as our noninvasive criterion standard to diagnose elevation of ICP. Several patients had headache. While headache can be a symptom of ICP, other confounding causes of headache such as trauma and mastoiditis were present in much of our patient cohort. Therefore, headache in isolation was not considered sufficient to diagnose elevated ICP.
The difference in the occurrence of elevated ICP in patients with and without hypoplastic draining sinuses was obtained by using the Fisher exact test. Statistical analysis was performed by using STATA/IC 13.1 (Stata Corp, College Station, Texas).
Results
The initial search identified 101 patients. Twelve patients with unilateral CSVT met our inclusion criteria, of whom 6 had a hypoplastic contralateral venous draining sinus and 6 did not. Basic demographic data and clinical characteristics, imaging findings, and location of the CSVT as well as the presence of elevated ICP with associated symptoms can be found in the On-line Table.
The 12 consecutive pediatric patients with unilateral CSVT were analyzed. This cohort included patients 2 months to 16 years of age who presented at our institution between 2011 and 2014. The causes of CSVT were otogenic in 50%, traumatic in 42%, and associated with hypercoagulability in 8%. All except 2 patients were additionally followed as outpatients to assess their response to therapy and outcome.
Of the 6 patients with hypoplastic contralateral draining sinuses, all had signs and symptoms of elevated ICP (vomiting, encephalopathy, diplopia, or sixth cranial nerve palsy). All 6 were formally assessed for the presence of papilledema by the ophthalmology department. Five of 6 patients had elevated ICP confirmed by papilledema. The sixth patient did not have papilledema and was not considered to have elevated ICP in our analysis.
Of the 6 patients with normal contralateral venous sinuses, several had headaches on presentation but none had any other signs or symptoms of elevated ICP. One had undergone a formal ophthalmologic evaluation in which papilledema was ruled out. The presence of a hypoplastic contralateral venous sinus in the setting of thrombosis of a dominant sinus was highly associated with elevation of ICP (83% versus 0%, P = .015).
Discussion
The aim of this study was to report 6 pediatric patients with unilateral CSVT with contralateral hypoplastic venous sinuses whose course was complicated by increased ICP and development of papilledema. We compared this cohort with 6 patients with unilateral CSVT and normal contralateral venous sinuses who did not have elevated ICP. There is sparse literature on the implications of venous drainage variants in CSVT. According to the International Pediatric Stroke Study1 41% of children with CSVT had an acute illness or acute head/neck disorder identified; these findings made these conditions the primary cause of CSVT in otherwise healthy children. The diagnosis of CSVT in a child can be elusive: Most children either present with vague signs and symptoms or the CSVT is found incidentally as part of a diagnostic evaluation for an associated condition (eg, mastoiditis). Treatment usually includes parenteral antibiotics for infectious causes and anticoagulation4; however, there is no established consensus regarding systemic thrombolysis5 or surgical options such as mastoidectomy, endovascular thrombectomy, or internal jugular vein ligation,6 especially with a hypoplastic contralateral venous draining sinus.
Time-of-flight MRV is often used to evaluate the intracranial dural sinuses and confirm or exclude CSVT.7 Variations in the normal anatomy of venous sinuses not only make the diagnosis of CSVT more difficult but also imply a different prognosis and could justify a more aggressive treatment approach. Alper et al7 reported that in healthy adults, symmetric sinuses were seen in only 31%, while aplasia of the left sinus was seen in 20%; hypoplasia of the left sinus, in 39%; hypoplasia of the right sinus, in 6%; and aplasia of the right sinus, in 4%. Widjaja and Griffiths8 reported that in healthy children, variations are also common and include 1 transverse sinus being absent or hypoplastic in 52% of cases in their cohort, with or without the presence of an occipital sinus as an alternative drainage system. Leach et al9 reported asymmetric transverse sinuses in up to 49% of cases. Consistent with these reports, in our cohort, the right transverse sinus was the dominant sinus in 5 of 6 cases. It is plausible that if the dominant venous sinus is occluded due to a thrombus, the contralateral side will not drain sufficiently and there will be an increased predisposition to the development of increased ICP.
Csákányi et al6 reported a case series of 8 patients with otogenic CSVT in whom various treatment approaches were used, including internal jugular vein ligation, anticoagulation, and thrombectomy. Of this cohort, 3 patients had hypoplasia of the left venous draining sinus by CT and MR imaging. Two of these 3 had complications secondary to long-standing ICP, including permanent visual impairment and prolonged sixth cranial nerve palsy. Of the remaining 5 patients with symmetric venous draining sinus, all did well, though 2 underwent steroid therapy due to progression of papilledema and 1 had mild headaches. Of the 8 patients in this series, 6 underwent anticoagulation for a variable number of months. Of the 2 patients who did not undergo anticoagulation, 1 had hypoplasia of the left venous sinus, and this patient underwent an internal jugular vein ligation and thrombectomy and mastoidectomy.
In our cohort of 12 patients, 9 were initially started on anticoagulation. All 6 patients with contralateral hypoplasia of venous draining sinus were started on anticoagulation, and 4/6 (66%) had a good outcome with no remaining symptoms and minimal complications (On-line Table). One developed persistently elevated ICP and required optic nerve fenestration for deteriorating vision. One patient was lost to follow-up.
Four of the 6 patients without contralateral hypoplasia had no persistent symptoms attributable to their CSVT, and the other 2 were lost to follow-up. Three of these patients underwent anticoagulation, and no associated complications were reported.
The onset of signs and symptoms of CSVT are often insidious, and though vomiting, lethargy, and headache are commonly seen in children with severe otogenic infections, focal neurologic deficits such as diplopia due to a sixth cranial nerve palsy or papilledema warrant brain imaging. Of the 12 patients with unilateral CSVT, 6 underwent dilated ophthalmologic evaluation during their hospitalization, which confirmed the presence of papilledema in 5, all of whom had contralateral hypoplasia of the venous draining sinus. In all patients with CSVT, especially in those with a hypoplastic contralateral venous sinus, an ophthalmologic evaluation as an indirect measure of elevated ICP is essential. In CSVT and venous backpressure, parenchymal injury can occur secondary to vasogenic and cytotoxic edema and possible hemorrhagic venous infarction, which can cause substantial morbidity and mortality. The post-thrombotic complications, such as the development of pseudotumor cerebri and papilledema, can cause long-term morbidity as well.3
The authors recognize that a limiting factor of this study is the small sample size, including a solely pediatric cohort. We support the call for larger studies including adult and pediatric populations with unilateral CSVT and contralateral venous draining sinus hypoplasia. The inclusion of both adult and pediatric patients might elucidate differences in the incidence of elevated ICP, treatment tendencies, and complications.
Conclusions
There are significant variations in venous sinus anatomy in about 50% of healthy children, with one side being hypoplastic to various degrees. We report 5 patients with unilateral CSVT associated with a hypoplastic contralateral venous draining sinus that developed raised ICP and papilledema and compare them with 6 patients with normal contralateral venous sinuses without elevation of ICP. Although unilateral hypoplastic venous draining sinus is a common incidental and benign variant, in CSVT of the dominant draining side, it can pose a considerable problem, leading to increased ICP and substantial morbidity. Children with unilateral CSVT and contralateral venous hypoplasia should be evaluated and followed closely for development of elevated ICP. Early aggressive medical and surgical therapy to eradicate the underlying infection in cases of otogenic CSVT, in combination with systemic anticoagulation to prevent thrombus extension and promote recanalization, can lead to favorable outcomes with minimal adverse events.
Footnotes
Disclosures: Robert Avery—UNRELATED: Grants/Grants Pending: National Institutes of Health K23 award (Topic: Optical Imaging in Children with Tumors of the Visual Pathway).
References
- Received March 28, 2016.
- Accepted after revision June 13, 2016.
- © 2016 by American Journal of Neuroradiology





{kind=link}
{kind=link}