
Abstract
BACKGROUND AND PURPOSE: Combined transarterial balloon-assisted endovascular embolization with double-lumen balloon microcatheters and concomitant transvenous balloon protection was described as a promising treatment technique for dural arteriovenous fistulae of the transverse and sigmoid sinus. The purpose of this study was to evaluate the technical efficacy and safety of this combined treatment technique.
MATERIALS AND METHODS: Nine consecutive patients presenting with dural arteriovenous fistulas of the transverse and sigmoid sinuses underwent combined transarterial and transvenous balloon-assisted endovascular embolization. Prospectively collected data were reviewed to assess the technical success rate, complication rate, and clinical outcome.
RESULTS: Six patients presented with clinically symptomatic Borden type I, and 3 patients, with Borden type II dural arteriovenous fistulas of the transverse and sigmoid sinuses (3 men, 6 women; mean age, 50.4 years). Transarterial embolization was performed with a double-lumen balloon with Onyx and concomitant transvenous sinus protection with a dedicated venous remodeling balloon. Complete angiographic occlusion at the latest follow-up (mean, 4.8 months) was achieved in 6 patients, and near-complete occlusion, in 2 patients. Clinical cure or remission of symptoms was obtained in 6 and 2 patients, respectively. One patient with a residual fistula underwent further treatment in which the dural arteriovenous fistula was cured by sinus occlusion. Complete occlusion of the dural arteriovenous fistula was visible on the follow-up angiography after final treatment in 8 patients. One patient refused follow-up angiography but was free of symptoms. There were no immediate or delayed postinterventional complications.
CONCLUSIONS: Transarterial balloon-assisted embolization of dural arteriovenous fistulas of the transverse and sigmoid sinuses with combined transvenous balloon protection is safe and offers a high rate of complete dural arteriovenous fistula occlusion and remission of clinical symptoms.
ABBREVIATION:
- dAVF
- dural arteriovenous fistula
During the past few decades, endovascular embolization has become the first-line treatment for a wide range of dural arteriovenous fistulas (dAVFs). Several transarterial and transvenous endovascular approaches have been advocated. Preliminary studies on the use of double-lumen balloon microcatheters for transarterial embolization of dAVFs with Onyx (Covidien, Irvine, California) have shown encouraging results. These studies have reported high occlusion rates, reduction of reflux into the feeding artery, a reduced quantity of injected Onyx and peri-interventional time, and low complication rates.1⇓⇓⇓⇓⇓⇓⇓–9 In addition, transvenous balloon-assisted sinus protection during transarterial embolization has been reported to be another useful adjunct to the endovascular treatment of dAVFs.10⇓–12 Transvenous balloon protection of the recipient sinus has mainly been associated with a reduction in inadvertent occlusion of the lumen of a functioning sinus, preservation of venous patency, facilitation of occlusion of abnormal arteriovenous connections within the sinus wall and separate venous channels, and increased penetration of embolic material by retrograde reflux into other dural feeders of the fistula network. Techniques aiming to preserve the underlying sinus may have lower complication rates than sinus-occluding embolization techniques, in which the recipient venous sinus has to be sacrificed.13 Therefore, transarterial balloon-assisted embolization with a concomitant transvenous balloon protection technique theoretically has the advantages of both techniques combined; this combination leads to increased occlusion and reduced complication rates.
The purpose of this study was to report the angiographic and clinical outcomes of patients with dAVFs of the transverse and sigmoid sinuses treated with a combined approach of transarterial balloon-assisted endovascular embolization and double-lumen balloon microcatheters with concomitant transvenous balloon protection.
Materials and Methods
Between August 2015 and September 2016, nine consecutive patients presented at our institution with symptomatic dAVFs of the transverse and sigmoid sinuses and were treated by combined transarterial and transvenous balloon-assisted endovascular embolization. Clinical and angiographic data were collected in a clinical data base and retrospectively analyzed.
Clinical data, including age, sex, clinical presentation, and clinical follow-up, were recorded. Angiographic data, including location and type of fistula (according to the Borden and Cognard classifications); feeding arteries; the angiographic outcome immediately after the treatment and during the follow-up angiography (at 3–6 months); and treatment-related data on arterial access, embolic agent, and technical and other related complications, were collected. Clinical deterioration, stroke, intracranial hemorrhage, and cranial nerve palsy were considered treatment-related complications. A technical complication was defined as any technical problem with the material used or any medical problem occurring during the intervention, including vessel perforation, inadvertent embolization of nontarget vessels, and failure to complete the treatment.
In patients who had Borden type I dAVFs, endovascular treatment was offered after reaching interdisciplinary consensus if intolerable clinical symptoms were present and if patients were actively asking for treatment.
Angiographic and Clinical Analysis
The imaging material was analyzed in detail by 2 experienced neuroradiologists (E.P. and P.M., with 8 and 12 years of experience, respectively), one of whom had no involvement in the treatment. Angiographic outcome was descriptively defined as complete occlusion if no residual fistula was visible; as near-complete occlusion with minimal residual fistula, if there was a 90%–99% occlusion rate; and as residual fistula, if an occlusion rate of <90% was achieved. To determine the clinical course, we asked patients before and immediately after the treatment, as well as during the follow-up examination (3–6 months), about the subjective improvement or deterioration of their symptoms, especially the intensity of the tinnitus. The outcome was categorized as better, equal to, and worse than before treatment. Clinical cure was defined as complete absence of previous symptoms.
Endovascular Technique
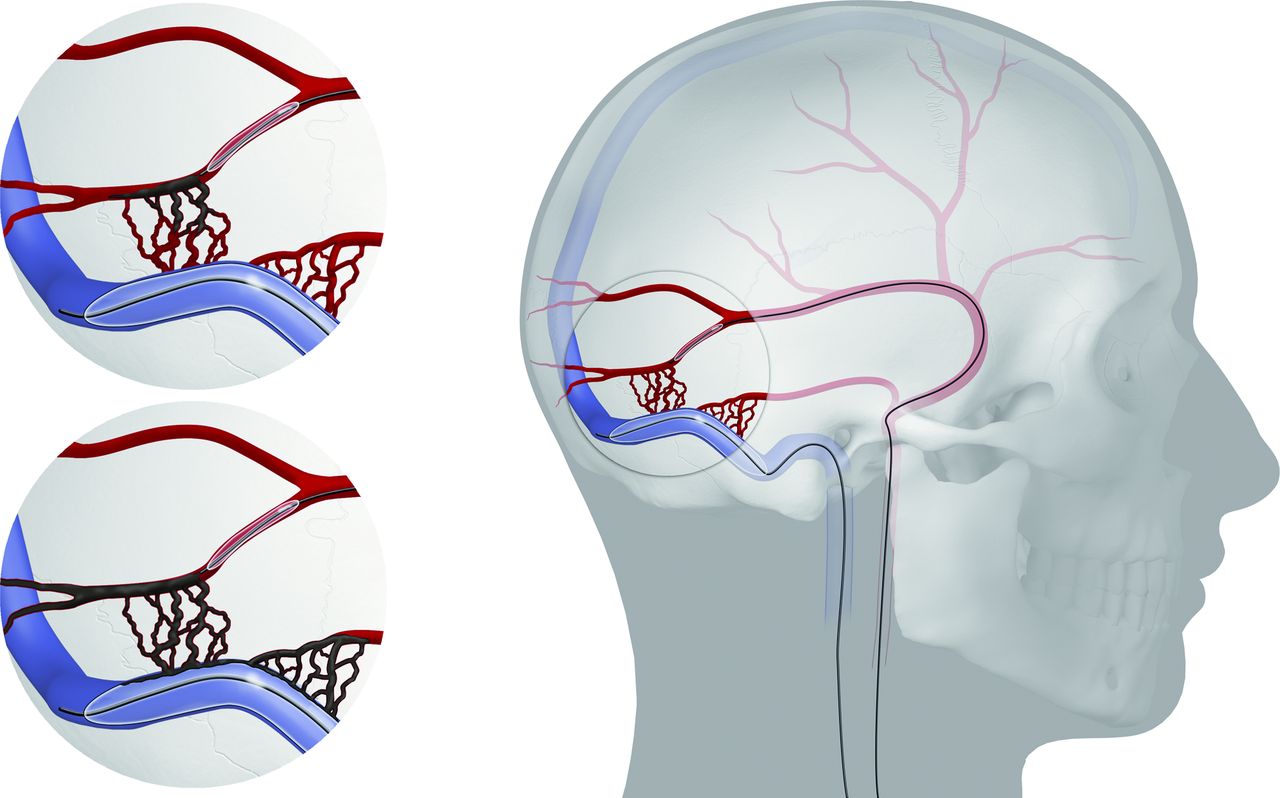
All endovascular interventions were performed by the same trained neuroradiologists (P.M., J.G.) with the patient under general anesthesia using a biplane neuroangiography suite (Artis zee; Siemens, Erlangen, Germany). After puncture of the left femoral vein and right femoral artery, an 8F guiding catheter was placed in the internal jugular vein and the external carotid artery on the side of the fistula (Guider Softip; Boston Scientific, Fremont, California). Transarterial navigation into the most promising arterial feeder was performed with a double-lumen dimethyl-sulfoxide–resistant balloon microcatheter (4 × 10 mm, Scepter C; MicroVention, Tustin, California) over a 0.014-inch microwire (SilverSpeed-14; Covidien). A distal position at the site of the fistula or close to the fistula could be achieved in all cases. Nimodipine (2 mg) was added to the continuous flushing line (1000 mL of saline) to facilitate distal navigation and to avoid or minimize mechanically induced vasospasm. Subsequently, via the transvenous route, a dedicated compliant dimethyl-sulfoxide–resistant venous remodeling balloon (8 × 80 mm, Copernic RC; Balt Extrusion, Montmorency, France) was navigated into the affected sinus covering the site of the fistula. After carefully inflating the transarterial double-lumen balloon, we performed microcatheter embolization with Onyx-18 and/or Onyx-20 under the roadmap technique (Fig 1). Simultaneously, the venous balloon was repeatedly temporarily inflated during transarterial Onyx injection for a maximum of 2–5 minutes. Inflation pressure was manually adapted to prevent Onyx migration into the main sinus lumen and to simultaneously achieve better penetration into the fistulous connections within and around the sinus wall (Fig 1).
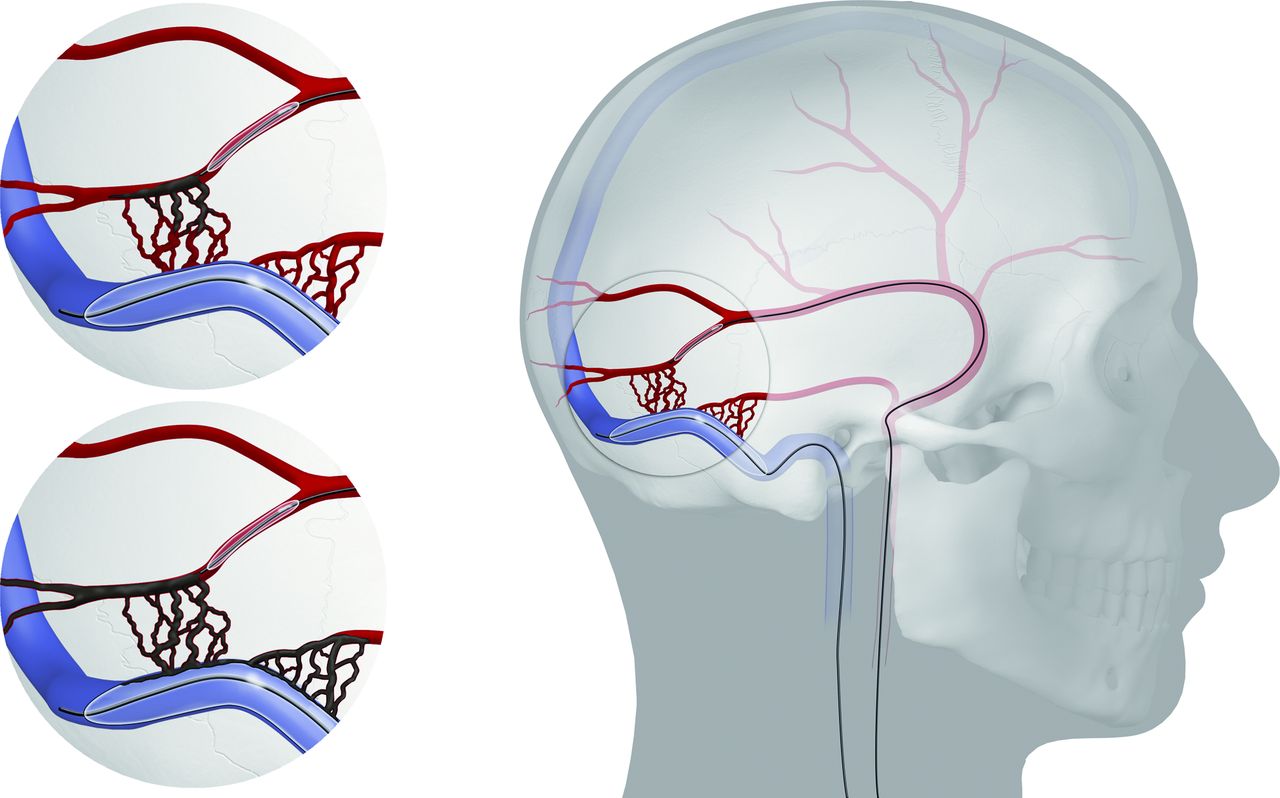
Demonstration of the technique combining transarterial balloon-assisted embolization and transvenous balloon protection in the endovascular treatment of dAVFs of the transverse and sigmoid sinuses. Onyx injection during inflation of the balloons with Onyx penetration throughout the feeding arteries and total occlusion of the fistula.
After termination of the liquid embolic injection, the transarterial and transvenous balloons were deflated and retrieved without any complications. A 4-vessel diagnostic angiography was performed at the end of every procedure to check for complete occlusion or residual fistula (Figs 2 and 3). Technical and procedural details are summarized in the On-line Table.

A 51-year-old man (patient 7) after 3 unsuccessful endovascular treatment attempts 10 years ago showing a progressive Borden I fistula on the right. A, Time-of-flight angiography. B, Right external carotid artery angiogram shows feeding arteries from the middle meningeal artery, occipital artery (black arrow), meningohypophyseal trunk (not visible), posterior auricular artery, artery of the falx cerebelli (not visible), subarcuate artery, and vertebral artery (not visible). C, Right external carotid artery angiogram after positioning of the venous balloon in the right transverse and sigmoid sinuses (8 × 80 mm, Copernic RC; white arrow). Middle meningeal artery (black arrow). D, Fluoroscopic image depicting the inflated venous balloon (black arrow), the arterial double-lumen balloon microcatheter in the middle meningeal artery, partially hidden behind Onyx (4 × 10 mm, Scepter C; white arrow), and the cast of Onyx-18. E, Right external carotid artery angiogram after embolization of the fistula with complete occlusion. F, Fluoroscopic image shows Onyx-18 distribution after complete occlusion of the dural fistula.

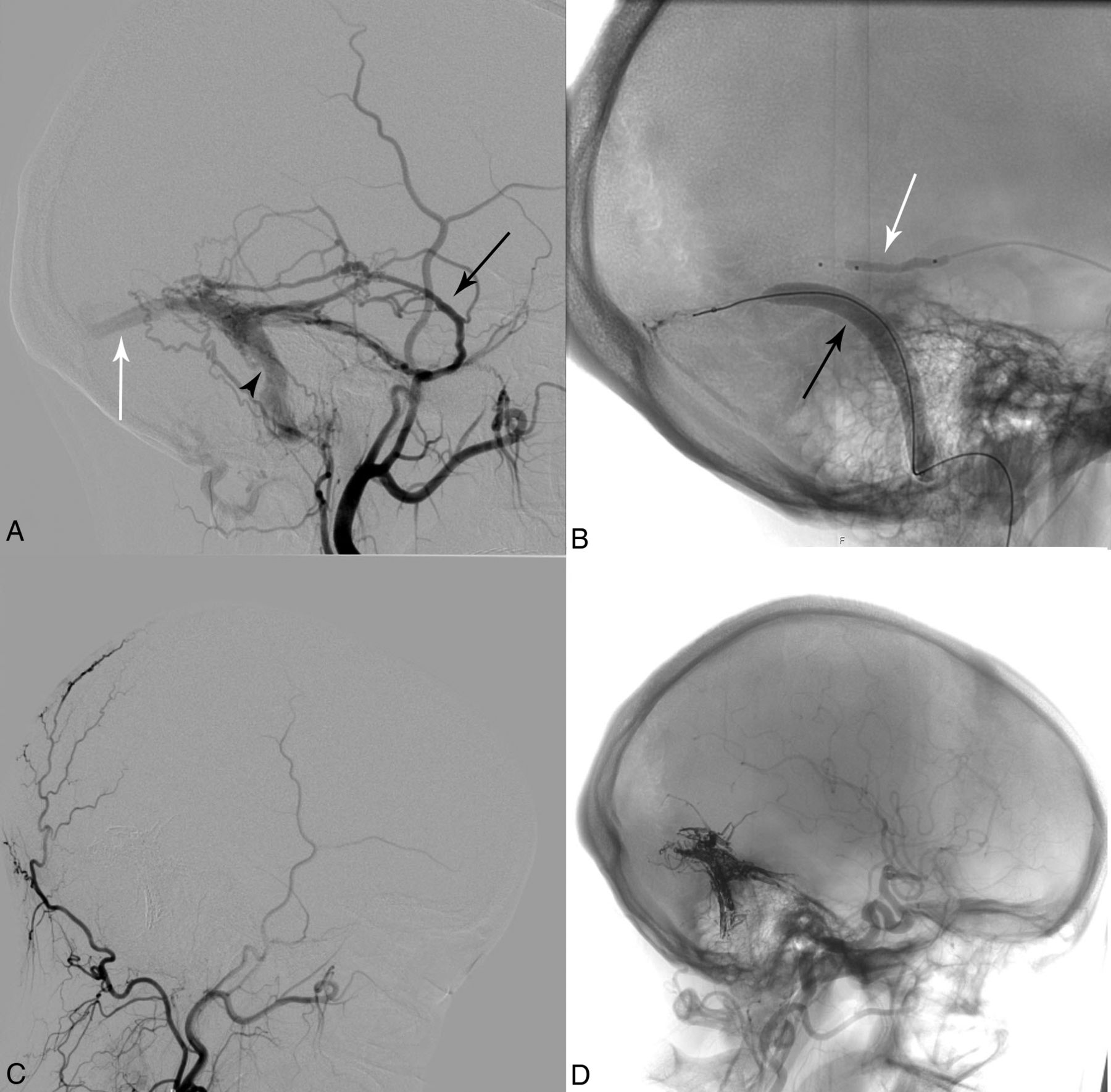
A 24-year-old woman (patient 1) with a Borden II fistula on the left. A, Baseline left external carotid artery angiogram with feeding arteries from the middle meningeal artery (black arrow), occipital artery, and meningohypophyseal trunk (not visible). Transverse sinus (white arrow); sigmoid sinus (black arrowhead). B, Fluoroscopic image showing an inflated venous balloon (8 × 80 mm Copernic RC; black arrow) and arterial double-lumen balloon catheter in the middle meningeal artery (4 × 10 mm, Scepter C; white arrow). C, Left external carotid artery angiogram (2-month follow-up) after embolization of the fistula showing complete occlusion. D, Fluoroscopic image depicting Onyx-18 distribution after complete occlusion of the dural fistula.
Results
Six patients presented with clinically symptomatic Borden type I; and 3, patients with Borden type II dAVFs of the transverse and sigmoid sinuses (3 cases of Cognard type I; 3 cases of Cognard type IIa; 1 case of Cognard type IIb; 2 cases of Cognard type IIa + b).14,15 Of these 9 patients, 3 were men and 6 were women. The mean age was 50.4 years (range, 24–66 years). Clinical symptoms at presentation were intolerable tinnitus in all 9 patients and additional headache in 3 patients. No patient had experienced dAVF-related hemorrhage. One patient (No. 7) presented with persistent intolerable tinnitus after 3 previous unsuccessful attempts at transarterial embolization, with residual fistula, while the other 8 patients presented with a newly diagnosed dAVF. Patient clinical characteristics are summarized in the On-line Table.
Overall, complete angiographic occlusion was achieved in 6 patients, and near-complete angiographic occlusion with minimal residual fistula, in 2 of the 9 patients after 1 embolization (88.9%), leading to clinical cure or remission of symptoms. In Borden type I fistulas with residual shunt, no transformation to a higher grade was noted postintervention, and all Borden type II fistulas with residual shunts were downgraded to Borden type I fistulas. Of the 6 patients with near-complete occlusion and minimal residual fistulas immediately after treatment, 5 patients showed complete clinical cure during follow-up of whom 4 patients showed a proven spontaneous complete occlusion of the fistula during follow-up imaging (1 patient with a residual fistula and residual tinnitus had a second treatment session, and the fistula was cured by sinus occlusion; 1 patient refused to undergo any follow-up imaging due to clinical cure). Eight patients underwent a single endovascular treatment session. Routine clinical or angiographic follow-up or both were performed after 2–6 months, and records were available for 8 of the 9 patients (mean follow-up, 4.8 months). Two patients refused to undergo the 6-month follow-up angiography due to clinical cure. There were no immediate or delayed permanent postinterventional complications.
Transarterial navigation of the balloon microcatheter to the target position in a main feeder close to the fistula point where Onyx injection was intended to start was possible in all 9 patients; this target was the middle meningeal artery. Embolization was performed from a single arterial feeder, and it was possible to place the venous remodeling balloon within the affected sinus segment in all patients. There were no technical difficulties or complications associated with balloon placement, inflation, deflation, or retrieval.
In 1 patient (No. 6) diagnosed with a Borden type II fistula, embolic material migrated into the proximal vein of Labbé despite venous balloon protection, most likely through a parallel dural channel not protected by the balloon. Consequently, the intervention was stopped prematurely to prevent further propagation of embolic material. No impairment of patency of the vein of Labbé was noted, and it was still contributing to the drainage of brain parenchyma. The patient had an uneventful clinical course, with no improvement of his initial intolerable tinnitus. Follow-up angiography demonstrated the residual Borden type I dAVF at the level of the distal sigmoid sinus. Progressive occlusion of the transverse and proximal sigmoid sinuses at the level of the previously embolized portion of the dAVF and at the level of the jugular bulb was noted. Because the distal sigmoid sinus was exclusively draining the fistula without any contribution of the cerebral veins, the residual dAVF was treated secondarily by transvenous sinus occlusion with coils and Onyx. Complete occlusion of the dAVF and complete remission of the tinnitus were achieved. Therefore, after the final treatment, all patients were free of symptoms, and 8 of 9 had an angiographic occlusion of the dAVF (1 patient with a minimal residual fistula refused to undergo any follow-up imaging).
Discussion
In our small series of patients with dAVFs, we achieved complete occlusion or reduction of flow to a minimal residual fistula in 88.9% of the cases after 1 embolization attempt, with complete improvement of the initial symptoms during follow-up. One patient with a residual fistula was treated again, which led to occlusion of the parent sinus followed by clinical cure. There were no immediate or delayed permanent postinterventional complications.
During the past few decades, endovascular embolization with liquid embolic material, particles, or coils has become the first-line treatment for a wide range of dAVFs. Several transarterial and transvenous endovascular approaches have been advocated. Recent technical improvements include the introduction of dimethyl-sulfoxide–compatible double-lumen balloon microcatheters for transarterial embolization and dedicated especially designed venous balloons for transvenous sinus protection. Combining the advantages of transarterial balloon-assisted embolization with transvenous balloon protection seems to be a promising treatment strategy. Formerly, use of the technique had only been reported in small case series as part of different endovascular treatment approaches for dAVFs.2,8,13
The introduction of dimethyl-sulfoxide–compatible double-lumen balloon microcatheters for transarterial embolization of dAVFs with Onyx has shown encouraging results in preliminary studies, with high occlusion and low complication rates.1⇓⇓⇓⇓⇓⇓⇓–9,16 In the largest study available, Kim et al5 compared the results of transarterial Onyx embolization for dAVFs using a double-lumen balloon with those obtained by using a nonballoon microcatheter. The use of a double-lumen balloon microcatheter led to an increased immediate complete occlusion rate, decreased procedure time, decreased Onyx injection time, and a decrease in the number of feeders requiring embolization compared with the group treated with a nonballoon microcatheter. The main advantages of double-lumen balloon-assisted embolization are immediate control of the antegrade flow of the embolic material without the need for proximal plug formation, more effective distal penetration into the fistula and possibly into the distal portion of other arterial feeders, and the prevention of reflux into adjacent arteries.5 The larger profile and greater stiffness of the balloon microcatheter compared with dedicated low-profile embolization microcatheters mean that a satisfactory distal injection position may not be reachable due to small vessel caliber or tortuosity.3 In our series, delivery of the balloon microcatheter was possible through the middle meningeal artery in all cases; this artery usually has a rather straight course, facilitating microcatheterization. The potential risk of vessel rupture as a result of overinflation of the balloon2 can be avoided by carefully inflating the balloon under fluoroscopic control.
Transvenous balloon protection during transarterial embolization was first proposed by Shi et al8 with a small compliant balloon originally designed for aneurysm remodeling. The introduction of a large dedicated dimethyl-sulfoxide–resistant single-lumen compliant balloon catheter for transvenous sinus occlusion (8 × 80 mm, Copernic RC) has facilitated this adjunctive technique and paved the way for its wider use. The advantages of transvenous balloon protection during simultaneous transarterial embolization include the prevention of inadvertent occlusion of the lumen of a functioning sinus required for cerebral venous drainage and propagation of embolic material into adjacent cortical or deep cerebral veins. Ertl et al13 recently conducted a retrospective comparison of sinus-preserving and sinus-occluding endovascular treatment techniques for low- and intermediate-grade dAVFs involving the transverse and sigmoid sinuses (Cognard type I–IIb). A higher rate of permanent fistula occlusion was achievable with sinus-occluding techniques than with the sinus-preserving technique (93% versus 71%), but this came at the cost of a higher complication rate (33% versus 0%). These results are in accordance with our findings using a combined transarterial and transvenous approach for sinus-preserving dAVF embolization, showing no permanent complications and a high rate of remission of clinical symptoms with a single treatment session. Two-thirds of our patient population presented with a low-grade dAVF with a known benign natural history and thus relative and no vital treatment indication, despite the disturbing tinnitus. Every treatment attempt should aim for the lowest risk of complications and the most favorable benefit-risk ratio.
Despite a small residual shunt in 5 patients, after the embolization session, all patients experienced remission of clinical symptoms with spontaneous complete occlusion in 4 patients during follow-up and subsequently complete clinical cure (1 patient refused the follow-up angiography due to clinical cure). Furthermore, transvenous balloon placement in the sinus was helpful to understand the vascular anatomy of the fistula network and its venous drainage during embolization. Parallel venous channels as recipients for the arterial shunt into the transverse/sigmoid sinus and multiple arteriovenous connections within the dural wall and not the sinus itself can be observed.17⇓–19 These venous recipient structures may be obscured and not distinctly identified during angiography and transarterial embolization. The use of transvenous balloon protection with inflation of the balloon within the main sinus lumen, covering the entire length of the diseased sinus, facilitates the identification and occlusion of these abnormal arteriovenous connections within the sinus wall and separates venous channels by enabling increased penetration of embolic material by retrograde reflux into other dural feeders of the fistula network. At the same time, the technique allows sinus patency control and provides continuous injection of liquid embolic material, minimizing the risk of leakage into the sinus.8,10⇓–12
Although no permanent clinical complications occurred in our series, inadvertent propagation of Onyx into the proximal vein of Labbé was noted despite balloon inflation inside the main sinus lumen in 1 patient (No. 6), most probably the result of retrograde leakage of liquid embolic material along a parallel channel. This finding emphasizes the necessity of monitoring and adjusting balloon pressure appropriately and carefully observing the Onyx penetration along the dural sinus. An inflation time of 2–5 minutes has been used with temporary deflation of the balloon during cessation of Onyx injection to avoid venous infarction due to prolonged transvenous balloon occlusion, especially in the dominant sinus or in those cases involving normal cortical veins.11
The limitations of our study include its retrospective nature, the small sample size, and, for some patients, the short follow-up period. However, the results were obtained in consecutive patients with a defined pathology who were treated with a standardized endovascular approach.
Conclusions
In our small series of patients with dAVFs of the transverse and sigmoid sinuses, we found no relevant adverse events and a high cure rate with a technique combining transarterial balloon-assisted embolization and transvenous balloon protection. Long-term follow-up and larger patient series are necessary to further assess its efficacy and durability.
Footnotes
Jan Gralla and Pasquale Mordasini contributed equally to the study.
Disclosures: Jan Gralla—UNRELATED: Consultancy: Medtronic and Penumbra, Comments: Global Principal Investigator of STAR and SWIFT-DIRECT (Medtronic), Clinical Events Committee member of the ProMISe Study (Penumbra)*; Grants/Grants Pending: Swiss National Foundation, Comments: research grant for MRI in stroke*. *Money paid to the institution.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received March 13, 2017.
- Accepted after revision June 1, 2017.
- © 2017 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- ihtObtura: A novel liquid embolic agent with post-embolization radiopacity loss, in endovascular treatment of brain arteriovenous malformations, dural arteriovenous fistulas, and tumors: CLARIDAD trial
- Balloon protection of the vein of Labbe during embolisation of a dural arteriovenous fistula
- Transarterial embolization of dural arteriovenous fistulas of the lateral sinuses with stent-assisted sinus protection
- Endovascular Management of Intracranial Dural Arteriovenous Fistulas: Transarterial Approach
- First clinical multicenter experience with the new Scepter Mini microballoon catheter
- Transarterial Treatment of Cranial Dural Arteriovenous Fistulas: The Role of Transarterial and Transvenous Balloon-Assisted Embolization
- The Influence of Angioarchitectural Features on the Success of Endovascular Embolization of Cranial Dural Arteriovenous Fistulas with Onyx
- Endovascular Treatment of Dural Arteriovenous Fistulas Using Transarterial Liquid Embolization in Combination with Transvenous Balloon-Assisted Protection of the Venous Sinus