
Abstract
BACKGROUND: Thrombectomy trials are often specifically interpreted as evidence for the effectiveness of stent retrievers. The effectiveness of other thrombectomy techniques such as aspiration thrombectomy should be validated through further investigation and review.
PURPOSE: To evaluate published treatment times and clinical outcomes in patients treated with aspiration thrombectomy or ADAPT (A Direct Aspiration, First Pass Technique) for acute ischemic stroke.
DATA SOURCES: A systematic literature review was performed following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. MEDLINE, Scopus, and the Cochrane trial register were searched on November 8, 2016.
STUDY SELECTION: Twenty studies (n = 1523 patients) were included in this review and meta-analysis. One of these studies was prospective, and the rest were retrospective.
DATA ANALYSIS: Meta-analysis was performed by using a random effects model. Data and publication bias were visualized with forest plots and funnel plots.
DATA SYNTHESIS: Five studies investigated aspiration thrombectomy only, and 16 studies investigated ADAPT. Of the 16 studies on ADAPT, the rate of successful recanalization (TICI 2b/3) was 89.3% (95% CI, 85.4%–92.3%). The proportion of patients with good clinical outcome (90-day mRS ≤2) was 52.7% (95% CI, 48.0%–57.4%).
LIMITATIONS: Studies on ADAPT were retrospective, and there was heterogeneity between studies for successful recanalization (P < .001) and good clinical outcome (P < .001). There was evidence of publication bias for recanalization rates (P = .01), but not for clinical outcomes (P = .42).
CONCLUSIONS: ADAPT and aspiration thrombectomy are effective approaches to thrombectomy, with high recanalization rates and excellent clinical outcomes reported in the literature. Aspiration thrombectomy is a promising neurointervention, but large prospective randomized studies are needed to validate its utility.
ABBREVIATION:
- ADAPT
- A Direct Aspiration, First Pass Technique
Endovascular therapy has recently been shown to be an effective intervention and is now the standard of care for acute ischemic stroke.1⇓⇓⇓–5 Broadly, there are 2 categories of techniques in endovascular treatment for stroke: 1) stent-based thrombectomy using retrievable stents with or without aspiration catheter and 2) aspiration thrombectomy using aspiration catheter alone. A Direct Aspiration, First Pass Technique (ADAPT) describes using aspiration thrombectomy as the first-line treatment with the possibility of adjuvant treatment if recanalization is not initially achieved. ADAPT is a commonly used thrombectomy technique among neurointerventionalists, but its effectiveness relative to stent-based thrombectomy has not been established.
Five randomized controlled clinical trials in 2015 (MR CLEAN, ESCAPE, REVASCAT, SWIFT PRIME, and EXTEND IA) demonstrated that thrombectomy is superior to intravenous alteplase for stroke caused by large vessel occlusions.1⇓⇓⇓–5 Thrombectomy was specifically limited to stent retrievers in some protocols and was the first-line treatment for most patients in these trials. These trials are often specifically interpreted as evidence for the effectiveness of stent retrievers. The effectiveness of other thrombectomy techniques such as aspiration thrombectomy should be validated through further investigation and review.
In this systematic review, we evaluated the effectiveness of aspiration alone and ADAPT and reviewed their advantages and disadvantages relative to stent-based thrombectomy. We also compared treatment times and clinical outcomes for patients treated with aspiration thrombectomy alone and patients who required further treatment with stent retriever.
Methods
Literature Search and Study Categorization
This review was conducted in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.6 A systematic review was performed on November 8, 2016 by using MEDLINE, Scopus, and the Cochrane trial register data bases. The search term was “(aspiration OR suction) AND stroke AND (thrombectomy OR endovascular OR neurointervention).” Duplicates were removed from records identified in the data base search. Articles were then screened based on title and abstract. The remaining papers underwent full-text review. Inclusion criteria were 1) the study must contain at least 20 patients treated with ADAPT or aspiration thrombectomy for acute ischemic stroke; 2) the study must include either a measure of treatment time or a measure of clinical outcome for patients treated with aspiration thrombectomy; and 3) the study must be written in English.
Aspiration thrombectomy and ADAPT are inconsistently defined in the literature. Terminology for aspiration thrombectomy includes thromboaspiration; forced arterial suction thrombectomy, or FAST; modified Penumbra System (Penumbra, Alameda, California); manual aspiration thrombectomy, or MAT; and ADAPT.7⇓⇓–10 Manual aspiration thrombectomy has variably been used to refer to stent-based thrombectomy under aspiration and to aspiration thrombectomy itself.9 ADAPT has a similar semantic fluidity, with some studies by using ADAPT and aspiration thrombectomy interchangeably. ADAPT has also been called sequential endovascular thrombectomy approach, or SETA; switching strategy for mechanical thrombectomy; and first-line aspiration.11
In this review, we define ADAPT as using aspiration thrombectomy on the first pass with the option of subsequent adjuvant treatment if recanalization is not achieved.12 We chose to define ADAPT in this way because allowing neurointerventionalists to switch to other thrombectomy methods after initial attempts at aspiration thrombectomy is a more clinically pragmatic approach.11 Furthermore, the ADAPT acronym explicitly specifies direct aspiration as a first pass and does not limit subsequent passes to aspiration.12
In contrast to “ADAPT” studies, we define “asp only” studies as ones that limit neurointervention to aspiration thrombectomy regardless of the initial ability to achieve recanalization. We make a distinction between “ADAPT-asp only” patients who received only aspiration under the ADAPT paradigm and “asp only” patients who were restricted to aspiration thrombectomy by treatment protocol. Patients treated with only aspiration under the ADAPT paradigm often achieved recanalization during initial passes with aspiration thrombectomy and did not require subsequent passes with stent retrievers. In contrast, “ADAPT-asp + adjuvant” patients often were not able to achieve recanalization with initial attempts at aspiration thrombectomy, and “asp only” patients continued with aspiration thrombectomy despite unsuccessful initial passes with aspiration thrombectomy. Patients who received only aspiration under the ADAPT paradigm might therefore represent less complicated cases, and we categorized them separately from patients restricted to an aspiration-only protocol.
Data Extraction
Demographic information, baseline characteristics, treatment, and clinical outcomes were extracted from studies that met the inclusion criteria. Demographic information included number of patients, age, and sex. Baseline characteristics include NIHSS at hospital admission and location of the occlusion. Treatment includes devices used, the proportion of patients who received IV-tPA before thrombectomy, onset-to-puncture times, puncture-to-recanalization times, proportion of patients treated with aspiration thrombectomy alone, and proportion of patients treated with stent retriever after attempt with aspiration thrombectomy (ADAPT). Clinical outcomes include TICI 2b/3 recanalization rate, rate of symptomatic intracerebral hemorrhage, rate of embolic occlusion in new territories, 90-day mRS, and 90-day mortality.
Statistical Analysis
Recanalization rates and clinical outcomes were assessed by meta-analysis. Cochran Q test and I2 test were used to detect heterogeneity. Significant heterogeneity was defined as either a Cochran Q greater than the χ2 critical value at 10% level of significance or an I2 value greater than 50%. A random effects model was used for meta-analysis. All statistical analyses were performed by using the R language for statistical programming (http://www.r-project.org/).
Results
Study Selection
The data base search yielded 708 studies from MEDLINE (270), Scopus (402), and Cochrane (36). Study selection is summarized in the flow diagram (Fig 1). Among these studies, the THRACE trial and the THERAPY trial were randomized controlled clinical trials with at least 20 patients treated with aspiration thrombectomy.13,14 The THRACE trial compared thrombectomy after intravenous alteplase with intravenous alteplase alone. Of 141 patients treated with thrombectomy, 23 (16%) were patients treated with aspiration.14 Outcome data specific to these 23 patients was not available, and this study was not included in this review. The THERAPY trial investigated whether aspiration thrombectomy after intravenous alteplase is superior to intravenous alteplase alone. The trial was terminated because of the loss of equipoise from the publication of MR CLEAN and the establishment of endovascular therapy with intravenous alteplase as the standard of care.13 The results of the trial are therefore underpowered, but are included in this meta-analysis. Ultimately, 20 studies comprising 1523 patients were selected for review (Table 1, On-line Tables 1 and 2).7⇓⇓⇓⇓⇓–13,15⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–27 Nineteen of these studies were retrospective, and 1 was prospective. Treatment times and clinical outcomes are summarized in Table 1.
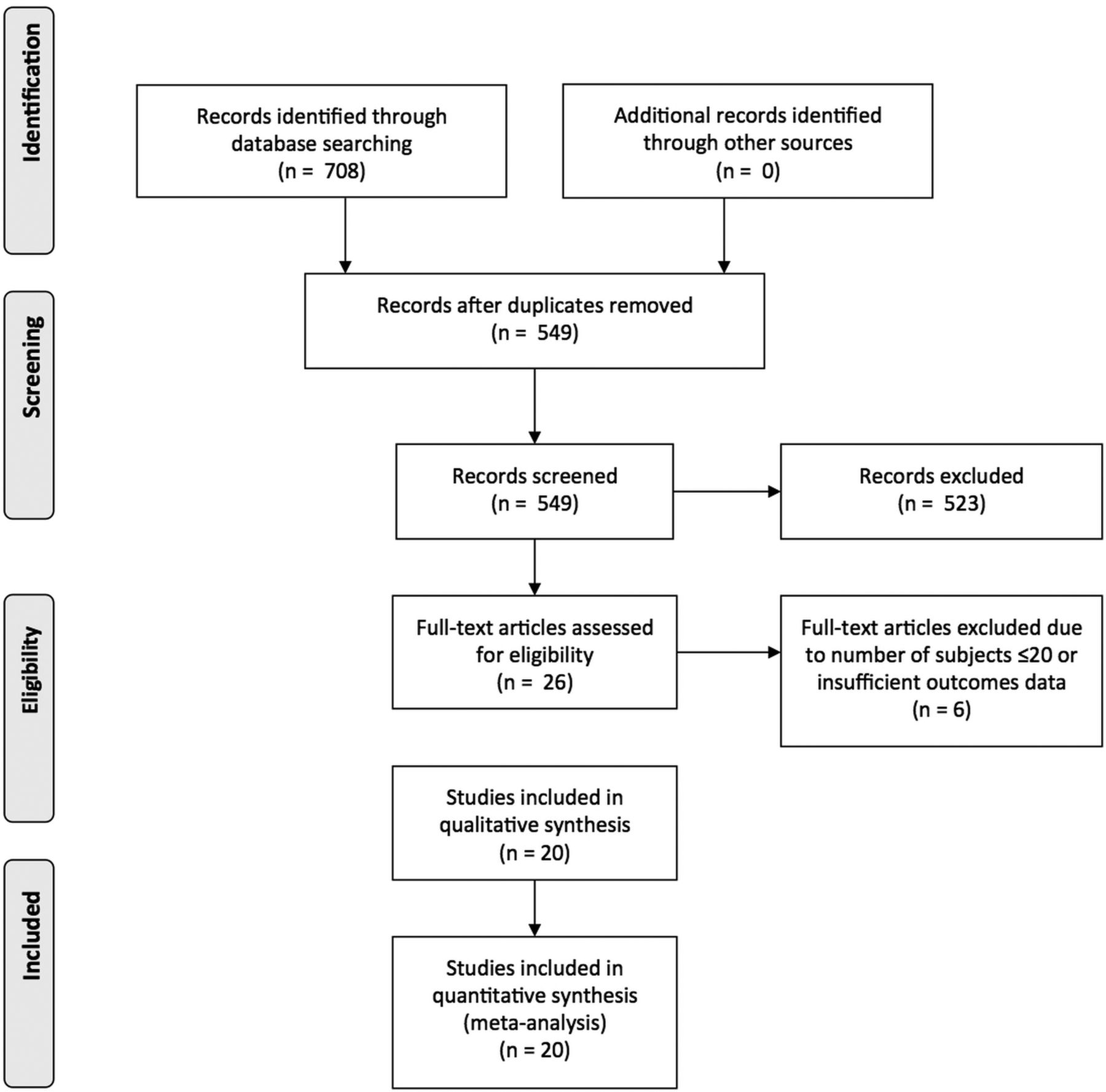
PRISMA flow diagram on study inclusion.
Treatment times and clinical outcomes by study
Of the 20 studies included in this review, 5 followed an aspiration-only approach to treatment and 16 used an ADAPT paradigm. One study included both an aspiration-only group and an ADAPT group.11 Four of the ADAPT studies included descriptive statistics for the subgroup of patients who were only treated with aspiration and the subgroup of patients with subsequent passes of adjuvant treatment after initial passes with aspiration thrombectomy (On-line Tables 3 and 4).18,21,23,26
ADAPT Meta-Analysis and Study Heterogeneity
A meta-analysis of 16 ADAPT studies was performed for rates of successful recanalization (TICI 2b/3) and good clinical outcome (90-day mRS ≤2). The TICI 2b/3 recanalization rate was 89.3% (95% CI, 85.4%–92.3%) (Fig 2). Among patients treated with ADAPT, 52.7% (95% CI, 48.0%–57.4%) had a good clinical outcome (Fig 3). Cochran Q test and I2 test suggest significant heterogeneity between studies for successful recanalization (Q = 54.5; df = 15; I2 = 72.5%; P < .001) and good clinical outcome (Q = 27.8; df = 12; I2 = 56.8%; P < .001). Tests for funnel plot asymmetry found evidence of publication bias for recanalization rates (P = .01), but not for clinical outcomes (P = .42) (On-line Figs 1 and 2).

Forest plot of TICI 2b/3 recanalization rates by study.

Forest plot of good outcomes (90-day mRS ≤90) by study.
Discussion
Endovascular treatment of acute ischemic stroke with large vessel occlusion more than doubles the odds of a good clinical outcome compared with medical treatment alone and is now considered the standard of care.28 Aspiration thrombectomy is a form of endovascular treatment that may have advantages over stent retrievers with respect to puncture-to-recanalization times, recanalization rates, cost-effectiveness, and clinical outcomes.15,18,29 In this literature review, we categorized studies involving treatment with aspiration thrombectomy into 3 categories: 1) patients treated under an aspiration-only paradigm, 2) patients treated under ADAPT who only received aspiration thrombectomy, and 3) patients treated under ADAPT.
Aspiration Thrombectomy
Comparatively few studies assess aspiration thrombectomy without adjuvant therapy, and 5 studies were included in this review. The THERAPY trial was a randomized controlled clinical trial comparing aspiration thrombectomy after intravenous alteplase to medical treatment with alteplase alone. Aspiration thrombectomy with the Penumbra System was the procedure specified in the study protocol; however, 13% of patients were nonetheless treated with a stent retriever. A Penumbra 3D separator was also used in 25% of patients. Although the trial was underpowered because of early termination from loss of equipoise, trends were seen in superior clinical outcomes for aspiration thrombectomy. Ninety-day mortality was 12% for aspiration thrombectomy and 23.9% for medical treatment (P = .18). In the per-protocol population, good clinical outcome as measured by ordinal mRS had a 2.2 odds ratio (P = .05) in favor of aspiration thrombectomy.13 An earlier retrospective study by Eom et al7 similarly found aspiration thrombectomy superior to intra-arterial fibrinolysis. Aspiration thrombectomy had faster procedure times as well as higher rates of recanalization and good clinical outcomes in this study on basilar artery occlusions.
In another retrospective study, Hwang et al8 found that aspiration thrombectomy for distal internal carotid occlusion strokes had superior recanalization rates and clinical outcomes compared with mechanical clot disruption. Patients treated with aspiration thrombectomy had a TICI 2b/3 recanalization rate of 64.7% (11/17) compared with 16.7% (1/6) for mechanical clot disruption (P = .04). Aspiration thrombectomy was also more likely to lead to good clinical outcome, with 45% (9/20) of patients having a 90-day mRS ≤2 compared with 16% (3/19) for mechanical clot disruption (P = .05). Park et al10 evaluated the effectiveness of aspiration thrombectomy for more distally located large vessel occlusions. Aspiration thrombectomy successfully recanalized 84% (27/32) of patients with M2 occlusions, resulting in a good clinical outcome (90-day mRS ≤2) for 78% (25/32) of patients.
Kang et al11 compared the aspiration-only paradigm with the ADAPT paradigm in a period-to-period analysis. There was a trend toward superior TICI 2b/3 recanalization rates for ADAPT over aspiration-only (P = .10), which became significant for difficult cases requiring at least 3 passes (P = .03). Overall, the aspiration-only paradigm may have superior clinical outcomes compared with intravenous medical management, intra-arterial fibrinolysis, and mechanical clot disruption. Aspiration only, however, may be inferior to the ADAPT paradigm.8,11,13
ADAPT–Aspiration Only
Among the 16 studies included in this review that used ADAPT, 4 provided descriptive statistics for the subgroup that received only aspiration thrombectomy. Patients who received only aspiration under the ADAPT paradigm had shorter puncture-to-recanalization times than patients who were also treated with stent retriever or other adjuvant therapies.18,21,23,26 This is expected because ADAPT calls for aspiration as a first attempt, so patients successfully treated with aspiration would have fewer passes and shorter treatment times than patients who had subsequent passes. The potential advantages of ADAPT may be especially realized in patients who are recanalized early through aspiration thrombectomy. In patients treated under ADAPT, 56%–91% were treated by aspiration alone.9,21
ADAPT
Comparisons of puncture-to-recanalization times, recanalization rates, and clinical outcomes between ADAPT and stent-based thrombectomy have been inconclusive and have had conflicting results.15,20,22,29 Kim et al20 found that ADAPT has longer puncture-to-recanalization times than stent-based thrombectomy for M2 occlusions. Turk et al29 reported the opposite and found faster treatment times for ADAPT, whereas Lapergue et al22 did not report a significant difference in treatment times despite patients treated under ADAPT having more passes overall. Both Turk et al29 and Lapergue et al22 reported higher recanalization rates for ADAPT; however, this did not translate to a significant difference in 90-day clinical outcome. In contrast, Delgado Almandoz et al15 reported no difference in treatment times despite more passes and no difference in recanalization, but found an advantage for ADAPT in clinical outcomes.
A meta-analysis of 16 studies was performed to assess rates of recanalization and good clinical outcome for ADAPT. The TICI 2b/3 recanalization rate was 89.3% (95% CI, 85.4%–92.3%) and the rate of 90-day mRS ≤2 was 52.7% (95% CI, 48.0%–57.4%). Goyal et al28 conducted a patient-level meta-analysis of MR CLEAN, ESCAPE, REVASCAT, SWIFT PRIME, and EXTEND IA. These 5 randomized clinical trials used predominantly stent-based thrombectomy for first-line neurointervention and had an overall recanalization rate of 70.5% (402/570) and good clinical outcome rate of 46.0% (291/633) (On-line Table 5). Although recanalization and good clinical outcome rates were lower for the stent retriever meta-analysis than the lower bound of the 95% CI for this ADAPT meta-analysis, different inclusion criteria between studies and significant heterogeneity in the ADAPT meta-analysis limit interpretation of the relative utility of these thrombectomy techniques.
ADAPT has furthermore been reported to result in fewer complications with intracerebral hemorrhage, fewer cases of subarachnoid hemorrhage, and shorter length-of-stay in an intensive care unit.15,29 These advantages have not been consistently found to be significant in the literature, and there does not appear to be a consensus on whether ADAPT offers any clinical advantages to stent-based thrombectomy with respect to complications.22,29 Unlike stent-based thrombectomy, however, patients with subcortical infarctions treated with ADAPT do not demonstrate an increase in hemorrhage, which may be because of aspiration thrombectomy having less of a shearing effect on vascular endothelium.16 Aspiration thrombectomy may therefore have a role in expanding inclusion criteria for endovascular stroke treatment.
Factors Affecting Success of Aspiration Thrombectomy
Choice of aspiration catheter may affect success with aspiration thrombectomy. As new aspiration catheters are introduced and neurointerventionalists become more experienced, success rates with aspiration thrombectomy are expected to improve.29 It is worth noting that treatment with aspiration alone does not necessarily translate to use of a single device. Jankowitz et al17 reported that a single aspiration catheter was able to achieve recanalization in 41% of patients, and an additional catheter was necessary in 18% of patients. Nonetheless, aspiration thrombectomy is more cost-effective and requires fewer resources than stent-based thrombectomy.29
The techniques used in aspiration thrombectomy and characteristics of large vessel occlusion may factor into relative success with aspiration thrombectomy and stent-based thrombectomy. Aspiration thrombectomy is particularly challenging with tortuosity, and a stent retriever may be the preferred method of treatment when the occlusion is located immediately distal to a severe acute angulation.20 Young age of the patient, however, has been found to be associated with successful revascularization when using aspiration thrombectomy.27 In Mascitelli et al,27 average age of the patient in cases with successful aspiration thrombectomy was 66.5 years, and average age of the patient in cases of aspiration failure was 74.1 years (P = .03).
Clot composition may influence the ease of thrombectomy, and it is possible certain types of clots are more amenable to different treatment modalities. Kang et al11 found that the ADAPT paradigm of switching to a stent retriever after initial failure with aspiration thrombectomy led to greater rates of recanalization than continued attempts with aspiration thrombectomy. Conversely, Kim et al30 used aspiration thrombectomy to successfully revascularize 83.3% of patients who were recalcitrant to initial passes with a stent retriever. Aspiration thrombectomy and stent-based thrombectomy may have unique roles in acute stroke neurointervention, and future studies may identify factors that predict favorable response to each endovascular treatment.
Limitations and Future Directions
Limitations of this study include heterogeneity in the studies that met inclusion criteria for meta-analyses as well as evidence of publication bias for recanalization rate. Furthermore, most of the studies included in this review used ADAPT as the treatment protocol. There is a paucity of literature directly comparing aspiration thrombectomy with stent-based thrombectomy. Nearly all studies, including all studies assessing ADAPT, were retrospective. The COMPASS trial and ASTER trial are 2 randomized controlled trials designed to assess the potential noninferiority of ADAPT compared with stent-based thrombectomy. One of these trials (ASTER) has finished recruitment and the other (COMPASS) is ongoing. The results from these trials will hopefully address a gap in the literature on the effectiveness of the ADAPT approach.
Conclusions
This systematic review confirms that ADAPT and aspiration thrombectomy are effective approaches to thrombectomy for acute ischemic stroke. Meta-analysis found ADAPT is associated with 89.3% of patients achieving TICI 2b/3 recanalization and 52.7% having a 90-day mRS ≤2. A limitation of this review is that there are few studies investigating aspiration thrombectomy without adjuvant therapy, and only retrospective studies of ADAPT were available for meta-analysis. Furthermore, the ADAPT meta-analyses have significant heterogeneity with evidence of publication bias in recanalization rates, which may limit interpretation of these results. Prospective studies are necessary to directly assess the utility of aspiration thrombectomy and ADAPT.
Footnotes
Disclosures: Johanna Fifi—UNRELATED: Consultancy: Penumbra, MicroVention; Grants/Grants Pending: Stryker; Payment for Lectures (including service on Speakers Bureaus): Penumbra. J,D. Mocco—UNRELATED: Consultancy: Rebound Medical, Endostream, Synchron, Cerebrotech, TSP, Pulsar; Grants/Grants Pending: Stryker Neurovascular, Penumbra, Medtronic, Microvention*; Stock/Stock Options: Blockade Medical, TSP, Cerebrotech; Other: Apama, The Stroke Project, Endostream, Synchron, Cerebrotech, NeurVana, NeuroTechnology Investors, Comments: investor/ownership. Reade De Leacy—UNRELATED: Consultancy: Medical Metrics, Dfine, Comments: spine interventional company. *Money paid to the institution.
References
- Received March 7, 2017.
- Accepted after revision May 24, 2017.
- © 2017 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Pretreatment and interventional parameters predict excellent recanalization of large vessel occlusion in patients with acute ischemic stroke
- Direct aspiration stroke thrombectomy: a comprehensive review
- Standard Diffusion-Weighted Imaging in the Brain Can Detect Cervical Internal Carotid Artery Dissections
- Need for rescue treatment and its implication: stent retriever versus contact aspiration thrombectomy