
Abstract
BACKROUND: The safety and efficacy of standard poststent angioplasty in patients undergoing carotid artery stent placement have not been well-established.
PURPOSE: We conducted a systematic review of the literature to evaluate the safety and efficacy of carotid artery stent placement and analyzed outcomes of standard-versus-selective poststent angioplasty.
DATA SOURCES: A systematic search of MEDLINE, EMBASE, Scopus, and the Web of Science was performed for studies published between January 2000 and January 2015.
STUDY SELECTION: We included studies with >30 patients describing standard or selective poststent angioplasty during carotid artery stent placement.
DATA ANALYSIS: A random-effects meta-analysis was used to pool the following outcomes: periprocedural stroke/TIA, procedure-related neurologic/cardiovascular morbidity/mortality, bradycardia/hypotension, long-term stroke at last follow-up, long-term primary patency, and technical success.
DATA SYNTHESIS: We included 87 studies with 19,684 patients with 20,378 carotid artery stenoses. There was no difference in clinical (P = .49) or angiographic outcomes (P = .93) in carotid artery stent placement treatment with selective or standard poststent balloon angioplasty. Both selective and standard poststent angioplasty groups had a very high technical success of >98% and a low procedure-related mortality of 0.9%. There were no significant differences between both groups in the incidence of restenosis (P = .93) or procedure-related complications (P = .37).
LIMITATIONS: No comparison to a patient group without poststent dilation could be performed.
CONCLUSIONS: Our meta-analysis demonstrated no significant difference in angiographic and clinical outcomes among series that performed standard poststent angioplasty and those that performed poststent angioplasty in only select patients.
ABBREVIATION:
- CAS
- carotid artery stent placement
Endovascular therapy of carotid artery disease has advanced during the past decade and is now considered a valuable treatment alternative to surgery in appropriately selected patients.1⇓⇓⇓–5 The indications for carotid endarterectomy were initially established in the North American Symptomatic Carotid Endarterectomy Trial6 in 1991, which expanded treatment indications to patients with symptomatic severe or moderate carotid stenoses. Formerly, patients who were not eligible for surgery were treated with percutaneous transluminal balloon angioplasty,7,8 first described by Kerber et al in 1980.9 Although procedure-related complication rates were similar/comparable for both treatment modalities,7,8,10 some potential drawbacks and specific problems occurred due to the endovascular approach, including luminal compromise from catheters and guidewires crossing the stenotic lesions and/or during balloon inflation (temporary carotid occlusion by a balloon and/or wire catheter), intraprocedural thromboembolic events, elastic vessel recoil, or intimal dissection.11 After the carotid artery stent placement technique was developed, stent-assisted balloon angioplasty showed better results in event-free survival and even lower repeat angioplasty rates.11 The primarily used balloon-expandable stents were increasingly replaced by self-expanding stents,11,12 exhibiting an intrinsic radial expansion force with memory on the stenotic vessel wall. Poststent balloon angioplasty may then be performed to closely appose the stent and intima and, moreover, to expand regions of residual stent narrowing.11
Supporters of standard poststent balloon angioplasty (per protocol) indicated that poststent ballooning decreased the incidence of restenosis by re-establishing the normal luminal diameter. However, numerous studies13⇓–15 have suggested that poststent balloon dilation increases the likelihood of postprocedural emboli. Moreover, poststent ballooning can increase the probability of reflex bradycardia and hypotension, which might be associated with higher rates of periprocedural and postprocedural complications.16⇓⇓–19
Some authors claim that poststent dilation should be performed on a selective, case-by-case basis to maximize patient benefits and limit complications. However, to the best of our knowledge, there is no evidence in the recently published literature supporting the superiority of either of these techniques. Standard poststent balloon angioplasty has become the standard of care in many vascular centers,20⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–35 and only some interventionalists19,36⇓⇓⇓⇓–41 prefer performing poststent angioplasty on a selective base. On the basis of the latter studies, standard poststent balloon angioplasty may be associated with additional risks in patients with acceptable angiographic results, without additional post–carotid artery stent placement (CAS) angioplasty.
To evaluate the safety and efficacy of standard poststent angioplasty versus selective poststent angioplasty, we conducted a systematic review and meta-analysis and analyzed outcomes by a series that performed standard poststent balloon angioplasty per protocol on all patients versus those that performed selective poststent balloon angioplasty on only a subset of patients.
Materials and Methods
Study Selection
A comprehensive review of the literature was performed by using the keywords “carotid stenosis,” “carotid artery disease,” “revascularization,” “carotid,” “stent,” “angioplasty,” and “endarterectomy” in both “AND” and “OR” combinations to search PubMed, Ovid MEDLINE, Ovid EMBASE, Scopus, and the Web of Science. Inclusion criteria were the following: English language; >30 patients; studies published between January 2000 and January 2015; studies that performed poststent angioplasty regardless of patient selection for this procedure; and studies with adequate data on periprocedural and postprocedural complications, outcome and technical success, and primary patency. The exclusion criteria were the following: case reports; in vitro, cadaveric or animal studies; studies with no poststent angioplasty; review articles, guidelines, and technical notes. In case of any inconsistencies or differences with regard to study inclusion/exclusion into the meta-analysis, the senior author decided on inclusion or exclusion (G.L.).
The electronic search was supplemented by contacting experts in the field and reviewing the bibliographies of included studies for relevant publications. Abstracts, methods, results, figures, and tables of full text for detailed review were searched by 2 independent reviewers (neurosurgeon O.P. and radiologist W.B.) for data on poststent balloon angioplasty selection, technical success, long-term primary patency, procedure-related morbidity and mortality, and possible selection-related complications such as periprocedural hypotension and bradycardia. The reference lists of retrieved articles were also screened for additional studies. Furthermore, in case of multiple publications from the same institution and/or the same authors, only the most recent and updated study was considered to avoid inclusion of overlapping patients.
Definition of Treatment Groups
The objective of this study was to determine whether there was any difference in angiographic and clinical outcomes among series in which standard poststent angioplasty was performed and those in which poststent angioplasty was performed in only select cases. Studies were categorized as either a “standard poststent balloon angioplasty” series or a “selective poststent balloon angioplasty” series. Standard poststent balloon angioplasty series were defined as those in which poststent angioplasty was reportedly performed in all patients, whereas selective poststent balloon angioplasty series were defined as those in which poststent balloon angioplasty was performed in select cases (ie, residual stenosis, poor wall apposition, and so forth).
Data Abstraction
For each study, we extracted the following descriptive clinical and anatomic information: patient demographics, initial clinical status, and the type of patient selection for the poststent balloon angioplasty (standard versus selective). We studied the following outcomes: periprocedural stroke rates with differentiation of minor and major stroke, periprocedural TIA, procedure-related neurologic or cardiovascular morbidity and mortality, periprocedural myocardial infarction, bradycardia and hypotension rates in all patients distinguishing between hemodynamic changes requiring intervention, long-term stroke rate at last follow-up, long-term primary patency, and technical success. Periprocedural complications were defined as those occurring within 30 days of the carotid artery stent placement.
Statistical Analysis
We estimated from each study the cumulative incidence (event rate) and 95% confidence interval for each outcome. Event rates for each intervention were pooled in the meta-analysis across studies by using the random-effects model.42 Consequently, there was no need for establishing a hierarchy of analyzed outcomes. Subgroup interactions were conducted by using an interaction test as described by Altman and Bland.43 For all outcomes, we quantified between-study heterogeneity by calculating the I2 statistics.44,45 Anticipating heterogeneity between studies, we chose this model a priori because it incorporates within-study variance and between-study variance. We were unable to test for publication bias due to the noncomparative nature of these studies.
Results
Literature Review
An initial comprehensive literature search yielded 1585 articles. Eighteen studies were removed as duplicates. On the initial abstract and title review, 1099 were excluded because they were deemed not relevant to the current study. Four hundred sixty-eight studies were reviewed in additional detail; 283 studies were irrelevant because they lacked information about the use of poststent balloon angioplasty and/or postprocedural outcome/complications of patients. Ninety-eight additional studies were excluded because they were either case reports or had too few patients. In total, 87 studies with 19,684 patients with 20,378 carotid artery stenoses were included. Series reporting standard poststent angioplasty included 16,983 procedures (83.3%), and series reporting selective poststent angioplasty included 3395 procedures (16.7%). Sixty included studies had ≥100 patients. Eleven studies were prospective, and 76 were retrospective. Data are summarized in On-line Table 1. Methodologic characteristics of included studies are listed in On-line Table 2. A flow diagram describing our literature search process is provided in Fig 1.
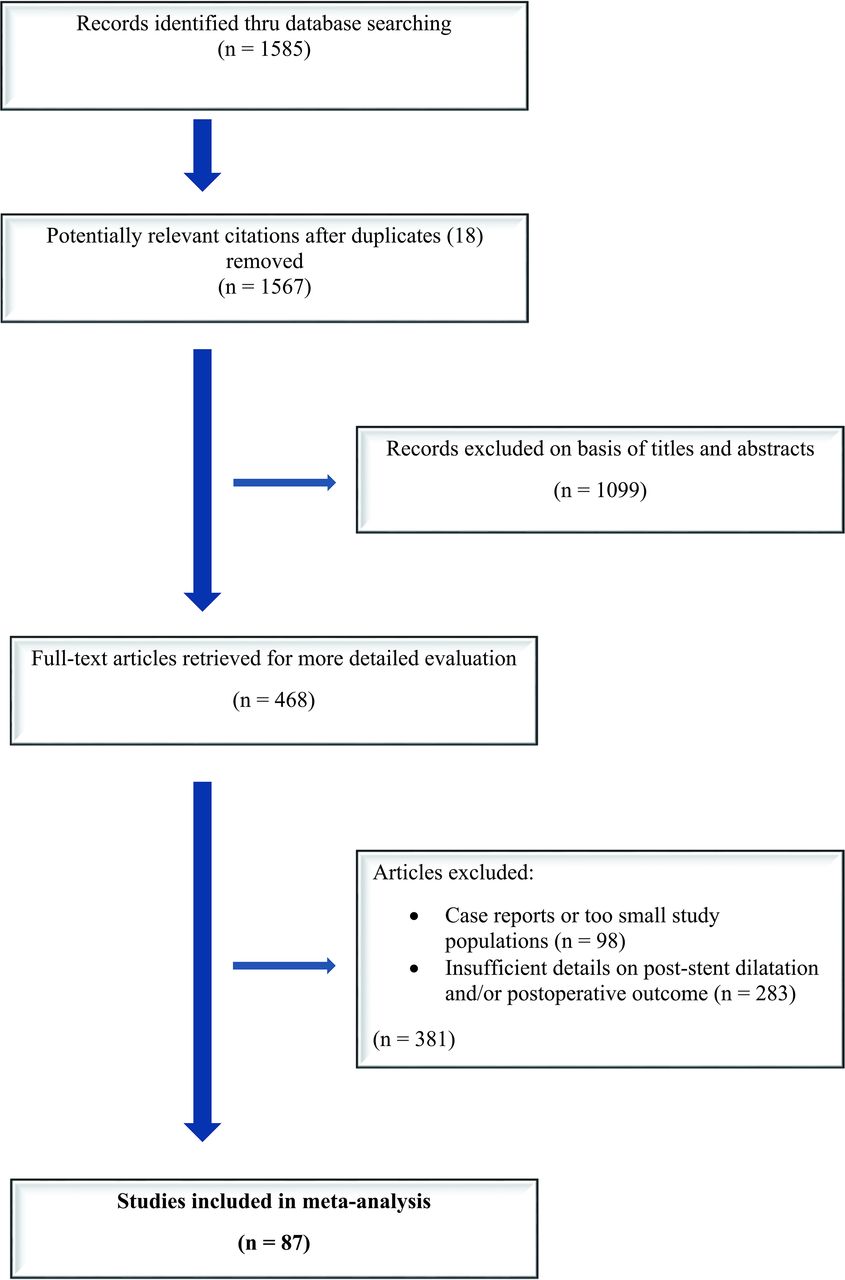
A flow diagram describing our comprehensive literature search.
Complication Rates by Type of Poststent Angioplasty
There were no statistically significant differences in any of the periprocedural and long-term complication rates by type of poststent angioplasty. Studies reporting selective poststent balloon angioplasty had similar rates of periprocedural stroke (2.3%; 95% CI, 1.8%–3.0%) compared with those reporting standard poststent balloon angioplasty (2.6%; 95% CI, 2.2%–3.1%) (P = .36). The same was true for long-term stroke rates (1.3% versus 1.6%, P = .49). Major stroke rates were similar in the selective poststent angioplasty group compared with the standard poststent angioplasty group (1.2% versus 1.0%, P = .44). There was no difference in minor stroke rates in the selective poststent angioplasty group (1.3% versus 1.7%, P = .19). There was no difference in periprocedural TIA rates either (1.7% versus 2.2%, P = .43). The periprocedural myocardial infarction rate was 0.6% (95% CI, 0.4%–1.1%) in the selective poststent angioplasty group versus 0.7% (95% CI, 0.5%–1.1%) in the standard poststent angioplasty group (P = .66). These data are summarized in On-line Table 3.
Periprocedural Hemodynamic Changes by Type of Poststent Angioplasty
Studies reporting selective poststent balloon angioplasty had significantly higher rates of bradycardia/hypotension (25.3%; 95% CI, 16.9%–36.3%) compared with those undergoing standard poststent angioplasty (13.3%; 95% CI, 8.0%–21.4%) (P = .04). The same was true for bradycardia/hypotension rates requiring interventions (18.7% versus 8.6%, P = .01). Data are summarized in On-line Table 3.
Angiographic Long-Term Results by Type of Poststent Angioplasty
There were no statistically significant differences in any of the long-term primary patency rates or technical success by type of poststent angioplasty. Studies reporting selective poststent angioplasty had similar long-term primary patency rates (94.3%; 95% CI, 90.7%–96.6%) compared with those undergoing standard poststent angioplasty (94.5%; 95% CI, 92.5%–95.9%) (P = .93). Technical success was 98.7% (95% CI, 97.1%–99.5%) in the selective poststent angioplasty group versus 99.0% (95% CI, 98.6%–99.3%) in the standard poststent angioplasty group (P = .61). These data are summarized in On-line Table 3.
Study Heterogeneity and Characteristics
Significant heterogeneity (I2 value > 50% and P value for the Cochrane Q test < .05) was noted in the analyses of 2 outcomes: bradycardia/hypotension and bradycardia/hypotension requiring intervention. Therefore, confidence in a pooled summary estimate for these 2 outcomes is limited. I2 values are summarized in On-line Table 3. Methodologic characteristics of included studies are listed in On-line Table 2.
Discussion
This systematic review and meta-analysis of 87 studies with 19,684 patients reporting either selective and standard poststent balloon angioplasty following carotid artery stent placement demonstrated no difference in clinical or angiographic outcomes in the CAS treatment with selective or standard poststent balloon angioplasty. In our study, we also found that both selective and standard poststent angioplasty groups had very high technical success rates of >98% and very low procedure-related mortality rates of 0.9%. Furthermore, there were no statistically significant differences between both groups in the incidence of restenosis or in procedure-related complication rates. Last, despite the selective poststent balloon angioplasty being associated with higher rates of periprocedural bradycardia/hypotension events, there was a very slight trend toward lower rates of periprocedural TIAs in these patients. These findings are important because they suggest that standard poststent angioplasty is not required during carotid stent placement. The similar rates of primary patency between groups suggest that the addition of standard poststent angioplasty does not provide any definite benefit.
Comparisons of clinical and angiographic outcomes between standard and selective poststent dilations in the literature are limited largely due to the small sizes of most case series. Numerous transcranial Doppler studies14,15,46 demonstrate the presence of emboli with each passage across a stenosis with a guidewire, embolic protection device, balloon, or stent, with the highest potential for embolization occurring during poststent dilation when the balloon pushes the stent struts against the atheromatous plaque. Ackerstaff et al47 reported in a series of 550 patients that multiple microemboli (>5 showers) at poststent angioplasty were independently associated with neurologic deficits. While our study found no statistically significant differences between the selective and the standard poststent angioplasty groups in terms of risk of stroke and TIA, the standard poststent angioplasty producing no benefit in primary patency suggests that this additional procedure may not always be necessary.
There has been considerable debate in the literature with regard to hemodynamic depression as a possible predictor of adverse events. Some studies16,17,19,48 suggested that hypotension may result in a greater incidence of periprocedural complications, and even death. To our knowledge, in the largest study to date of 103 patients evaluating the effect of poststent ballooning on hemodynamic stability during and after carotid stent placement, Qazi et al19 demonstrated that poststent balloon angioplasty was a significant predictor of hemodynamic depression (OR, 3.8; 95% CI, 1.3–11; P < .01) with increased risk of major adverse cardiovascular events. Gupta et al16 showed that patients with persistent hypotension are at a higher risk of developing an adverse clinical event such as stroke or death after CAS. On the other hand, our study found higher rates of bradycardia/hypotension in patients treated with selective poststent angioplasty compared with standard poststent angioplasty; however, there was no impact on procedure-related complications. The reasons behind this surprising finding in our study are not known. Presumably, patients who undergo selective post-CAS dilation are more likely to have rigid stenoses or insufficient alignment of the stent with the vessel wall compared with those undergoing standard post-CAS angioplasty. Consequently, selective post-CAS dilation is then performed in these cases. During this procedure, relevant hemodynamic events such as bradycardia and/or hypotension can occur, reflecting forced opening of the rigid stenosis.
Limitations
We acknowledge that our meta-analysis has several limitations. Studies reporting only carotid artery stent placement without subsequent angioplasty were excluded. With this design, no comparison with a group without poststent dilation could be performed. There was a paucity of studies comparing outcomes of patients who received no poststent angioplasty and those who did. Our results should not be interpreted as saying that poststent angioplasty is ineffective because it is likely useful on a case-by-case basis. Rather, our results should be interpreted to say that there is no difference in angiographic and clinical outcomes among patients undergoing standard poststent angioplasty and those undergoing selective poststent angioplasty.
Ecologic bias (eg, comparisons are made across studies and not within studies), the possibility of publication bias, and statistical heterogeneity are important limitations that affect inferences derived from this study. None of the included studies were randomized or included control groups. There was no detailed information regarding the indications for selective poststent angioplasty. Similarly, there was no information about residual stent narrowing before performing balloon angioplasty. However, given the contemporary and widely accepted literature evidence for treatment of carotid artery disease, all included studies most likely had similar strict indications for carotid artery stent placement.
Conclusions
This meta-analysis of >87 series reporting selective and standard poststent balloon angioplasty following carotid artery stent placement demonstrated that both standard and selective approaches were associated with low rates of procedure-related neurologic or cardiovascular morbidity and high rates of long-term primary patency of >94%. There were no statistically significant differences in clinical or angiographic outcomes between series reporting standard and selective poststent angioplasty. Comparative prospective studies are needed to confirm our findings.
Footnotes
Disclosures: Giuseppe Lanzino—UNRELATED: Consultancy: Covidien/Medtronic.* *Money paid to the institution.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
- 89.
- 90.
- 91.
- 92.
- 93.
- 94.
- 95.
- 96.
- 97.
- 98.
- 99.
- 100.
- 101.
- 102.
- 103.
- 104.
- 105.
- 106.
- 107.
- 108.
- 109.
- 110.
- 111.
- 112.
- Received August 29, 2016.
- Accepted after revision December 12, 2016.
- © 2017 by American Journal of Neuroradiology





{kind=link}