
Abstract
BACKGROUND AND PURPOSE: Spinal epidural meningioma is an uncommon tumor. This study aimed to analyze the imaging and pathologic characteristics of this rare tumor.
MATERIALS AND METHODS: Fourteen confirmed cases of epidural meningioma were retrospectively reviewed, and imaging characteristics and pathologic findings were analyzed to identify the typical features.
RESULTS: The mean age of the patients (4 men, 10 women) was 44.9 years. Twelve tumors were in the cervical spinal canal, and 2, in the thoracic spinal canal. There were 9 en plaque meningiomas, 4 dumbbell-shaped meningiomas, and 1 fusiform/ovoid meningioma. The epidural meningiomas extended over 2–5 spinal segments (mean, 3.2 spinal segments). A soft epidural mass was seen in 12/14 (86%) patients. Dural calcification was seen in 8/14 (57%) tumors. Tumor caused intervertebral foramen enlargement in 10/14 (71%) patients and adhered to the nerve roots in 11/14 (79%) patients. Intradural invasion was seen in 8/14 (57%) patients. The dural tail sign was present in 13/14 (93%) tumors on contrast-enhanced T1WI. Regarding pathologic type, 10 of 14 (71%) were psammomatous, 2 of 14 (14%) were meningothelial, 1 of 14 (7%) was angiomatous, and 1 of 14 (7%) was transitional. During follow-up (mean follow-up, 73.4 months; range, 4–192 months), 7 patients had recurrence. Recurrences were between 4 and 192 months after the operation.
CONCLUSIONS: Epidural meningioma has 3 different growth patterns. Dural thickening, calcification, invasion, and epidural mass formation are characteristic features of epidural meningioma. Regular follow-up imaging is required to detect recurrence.
Meningiomas are the second most common intraspinal tumors after schwannomas and account for approximately 25% of all intraspinal tumors. Meningiomas may be intradural or epidural. Most are intradural, and the most common presentation is an intradural meningioma in the thoracic spinal canal of a middle-aged woman. Epidural meningiomas are rare and account for only 3%–21% of meningiomas.1,2 Only 39 epidural meningiomas (10 in male patients and 29 in female patients) have been reported in the literature from 1963 to 2013.3⇓⇓⇓⇓⇓⇓⇓⇓–12 The age of the patients ranged from 13 to 74 years (mean, 41.24 ± 17 years). Of the 39 tumors, 21 were in the cervical spinal canal; 14, in the thoracic spinal canal; 3, in the cervicothoracic spinal canal; and 1, in the lumbar spinal canal. The cases reported until now showed a female predilection and susceptibility of the patients in their fourth decade of life. Epidural meningiomas may be en plaque, dumbbell-shaped, or ovoid.1,13 There are distinct differences in biologic behavior between epidural and intradural meningiomas. Because of its aggressive behavior, epidural meningioma may easily be mistaken for a malignant spinal tumor on preoperative imaging studies; postoperative recurrence is also not rare. Accurate diagnosis is therefore of great importance. Epidural meningiomas have some distinctive imaging features. The aim of this study was to identify the characteristic imaging findings of epidural meningioma.
Materials and Methods
Patients
From 2006 to 2015, fourteen patients were diagnosed with epidural meningioma at our institution. Three patients had postoperative recurrence. All patients underwent CT and MR imaging. The final diagnosis was based on intraoperative confirmation of an extradural tumor and postoperative pathologic diagnosis of meningioma. Intradural meningiomas invading or extending into the epidural space were excluded. Clinical information, including age at presentation, sex, history, duration of signs and symptoms, imaging findings, and follow-up data were collected from the case records and retrospectively reviewed.
Imaging Protocol
CT examinations were performed with a multidetector CT system (LightSpeed 64; GE Healthcare, Milwaukee, Wisconsin) with intravenous administration of contrast material (80 mL injected at a rate of 3 mL/s). Tube voltage of 120 kV and tube current of 250 mA were used. The acquisition section thickness was 0.625 mm. For image reconstruction, a standard method was selected. All datasets were reconstructed with an effective section thickness of 3 mm. The exposure time was 800 ms.
MR imaging was performed with a 3T scanner (Magnetom Tim Trio; Siemens, Erlangen, Germany) with the patient in a supine position. MR phased array spine coils and related scanning techniques were applied. The standardized protocol included sagittal T1-weighted FSE imaging (TR/TE, 618/11 ms; FOV, 280 × 100 mm) and sagittal (TR/TE, 2852/96 ms; FOV, 190 × 180 mm) and axial (TR/TE, 2720/88 ms; FOV, 190 × 180 mm) T2WI. Sagittal proton-density imaging (TR/TE, 2800 /34 ms; FOV, 250 × 280 mm) was also performed. The same section thickness (3 mm) and section gap (0.3 mm) were used in all procedures. All patients also underwent axial, sagittal, and coronal gadolinium-enhanced (0.2 mmol/kg; injection rate, 2 mL/s) T1-weighted fat-saturated (3D volumetric interpolated breath-hold examination) imaging (TR/TE, 700/11 ms; FOV, 280 × 100 mm; section thickness, 3 mm; section gap, 0.3 mm).
Image Analysis
Two radiologists specializing in spinal diseases reviewed all images on a PACS workstation. Abnormalities were identified and characterized by consensus. They assessed the following features: tumor location, morphology, and growth patterns; signal intensity on T1- and T2-weighted images (hypointense, isointense, or hyperintense relative to the normal spinal cord); and pattern and degree of enhancement. Bony erosion and calcification were evaluated on CT.
Pathologic Examination
All 14 patients underwent complete or partial resection of the tumor. Pathologic review was performed on hematoxylin-eosin–stained tissue from all cases.
Results
Clinical Findings
The 14 patients included 4 men and 10 women (mean age, 44.9 years; age range, 20–76 years). The presenting symptoms were bilateral lower limb numbness (6 patients), bilateral lower limb numbness plus upper limb weakness (4 patients), bilateral lower limb numbness plus upper limb pain and numbness (3 patients), and cervical mass (1 patient). Symptom duration ranged from 3 months to 10 years.
CT Findings
Table 1 lists the location, morphology, and growth patterns of the 14 tumors. The tumor was in the cervical spinal canal in 12/14 (86%) patients and in the thoracic spinal canal in 2/14 (14%) patients. Regarding shape, 4/14 (29%) tumors were dumbbell, 9/14 (64%) were en plaque, and 1/14 (7%) was oval/fusiform. Six en plaque and 2 dumbbell-shaped tumors showed flaky dura calcification on CT (Figs 1A, -B and 2A); thus, calcification was present in 57% (8/14) of patients. In 10/14 (71%) patients, the tumor extended through the intervertebral foramen to the outer part of the spinal canal, causing enlargement of the foramen. In 5/14 (36%) patients, tumors in the cervical spine compressed adjacent bone, leading to bone erosion; however, there was no bone destruction. Table 2 lists the CT findings.
Location, shape, and calcification of epidural meningioma
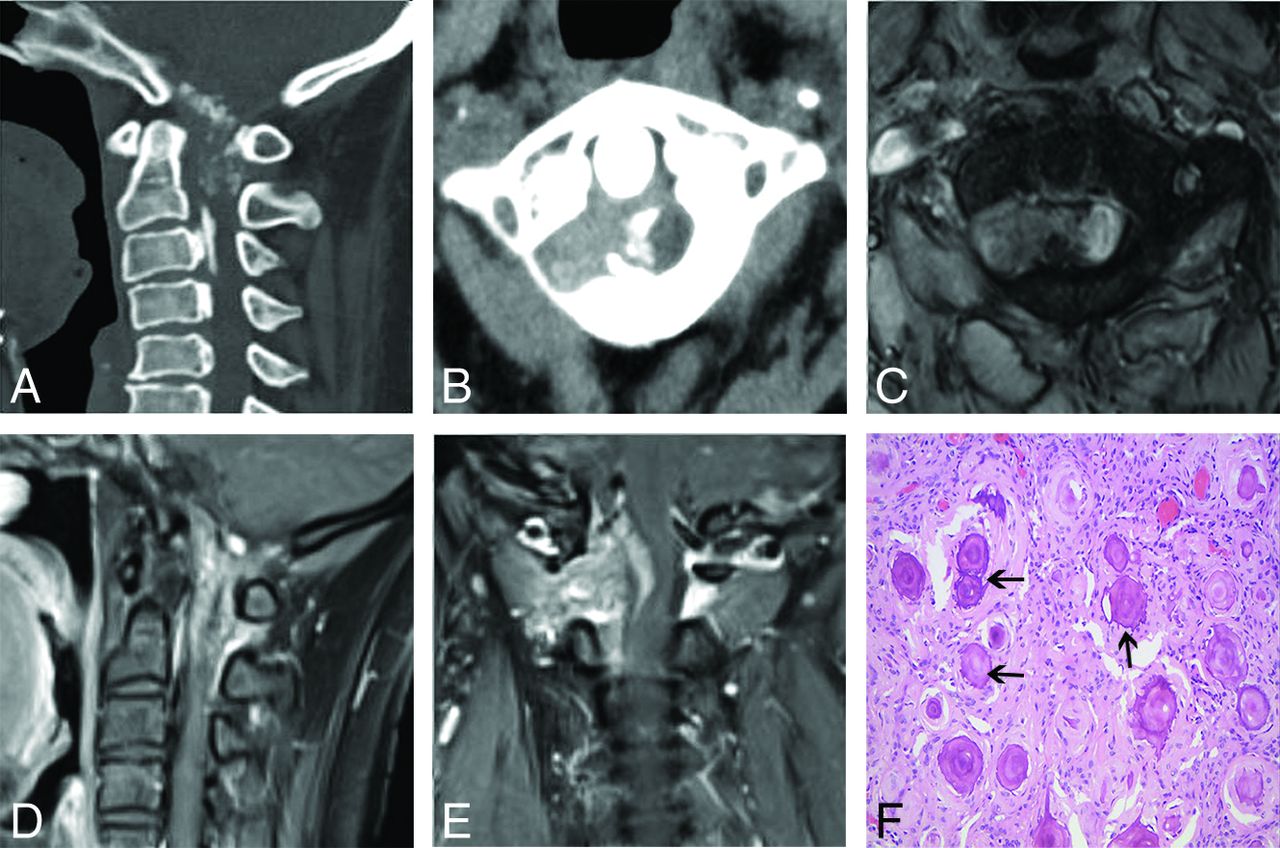
A dumbbell-shaped epidural psammomatous meningioma in 43-year-old woman at C1–2. Sagittal CT image (A) reveals the dura from the occiput to C2 thickened with patchy calcification. The ossification of the posterior longitudinal ligament is seen in the C2–3 segment. Axial CT image (B) shows a high-intensity epidural mass formed at C1–2 with adjacent bone thinned. Axial T2-weighted image (C) shows that the soft mass has low signal intensity compared with that of the spinal cord. Postcontrast T1-weighted sagittal (D) image demonstrates a diffusely enhancing dorsal and ventral dura extending over 2 vertebral segments. Postcontrast T1-weighted coronal image (E) shows an epidural mass with moderate enhancement and C1–2 intervertebral foramen enlargement. The spinal cord was markedly displaced, and intradural invasion can be seen. F, Photomicrograph of the epidural component shows a psammomatous meningioma characterized by the presence of psammoma bodies (arrows). H&E, original magnification, ×200.

En plaque epidural psammomatous meningioma in a 48-year-old woman at C2–4. Sagittal CT image (A) reveals the dural calcification at the C2–4 spinal segments. Sagittal T2-weighted image (B) shows that the epidural lesion is isointense. Axial T2WI (C) shows that epidural soft mass encircles spinal cord as a half ring. Axial postcontrast T1-weighted image (D) shows that the homogeneously enhanced epidural mass encircling the spinal cord from the ventral and dorsal sides. Sagittal postcontrast T1-weighted image (E) shows homogeneous enhancement of the ventral and dorsal dura, and the dural tail sign can be seen. Coronal postcontrast image (F) shows homogeneous enhancement of the epidural mass that compresses the spinal cord. G, Photomicrograph of a psammomatous meningioma is characterized by the presence of psammoma bodies (arrow). There are meningothelial cells (long arrow) and a small number of fibrous components. H&E, original magnification, ×200.
Imaging and pathologic findings
MR Imaging Findings
Table 2 lists the MR imaging findings. There were 9 en plaque meningiomas with a sheet-like or collar-like appearance on sagittal images. In these cases, the mean thickness of the dura was 4.56 mm, and the mean length of the thickened dura was 54 mm. En plaque epidural meningiomas extended along the dorsal and/or ventral dura, and 7/9 (78%) presented a half-ring appearance on axial MR images (Figs 1C and 2B, -C).
The epidural meningiomas in this study extended over 2–5 spinal segments (mean, 3.2 spinal segments). A soft epidural mass was seen in 12/14 (86%) patients, including 7 patients with en plaque, 4 with dumbbell-shaped, and 1 with fusiform epidural meningiomas (Fig 3A–C). Meningiomas caused spinal canal narrowing in 12/14 (86%) patients, with 9 en plaque meningiomas with even narrowing, 4 dumbbell-shaped, and 1 fusiform with lateralized narrowing. Spinal compression was seen in 12/14 (86%) patients. The epidural meningiomas in this study tended to adhere to the dura; only 2 tumors did not show that adhesion. In 11/14 (79%) patients, the tumors adhered to the nerve roots, leading to difficulty in separating the nerve from tumor during the operation. Intradural invasion was seen in 8/14 (57%) patients.

Fusiform epidural angiomatous meningioma in a 59-year-old woman at T4–6. Sagittal T1-weighted MR image (A) shows the epidural mass with signal intensity like that of the spinal cord. The subarachnoid space is obliterated at the level of the mass. Sagittal T2-weighted MR image (B) shows that the mass has heterogeneous signal intensity and the spinal cord is compressed with edema. Sagittal T1-weighted postcontrast image (C) reveals homogeneous enhancement of the extradural meningioma, and the dural tail sign can be seen. Photomicrograph shows that this tumor is composed of islands of meningothelial cells with many vascular vessels (thin arrows, D). H&E, original magnification, ×200.
On T1WI, epidural meningiomas were isointense (8/14, 57%) or hypointense (6/14, 43%) relative to the normal spinal cord. On T2WI, hypointense signal was seen in 7/14 (50%) patients; isointense signal, in 5/14 (36%) patients; and heterogeneous signal, in 2/14 (14%) patients. The tumors showed moderate (5/14, 36%) or marked (9/14, 64%) enhancement on postcontrast scans (Figs 1D, -E and 2D, -F). On contrast-enhanced T1WI, the dural tail sign was present in 13/14 (93%) tumors.
Pathologic Characteristics and CT/MR Imaging Findings
On gross examination, the tumors were red (11 tumors) or gray–white (3 tumors). On pathologic examination, 10/14 (71%) tumors were diagnosed as psammomatous and 2/14 (14%), as meningothelial meningiomas. Under light microscope, the tumor was composed of fibroblast-like cells; calcified psammomatous bodies were visible in 8/14 (57%) tumors (Figs 1F and 2G). These findings were consistent with their imaging manifestations, namely hypointensity on T1- and T2-weighted images and strip or flaky calcification on CT. One tumor was diagnosed as angiomatous, and one, as a transitional meningioma. The angiomatous meningioma was composed of numerous blood vessels with focal meningioma morphology (Fig 3D), while the transitional type was composed of characteristic uniform tumor cells. These findings were consistent with the heterogeneous signal on T2WI. All the above-mentioned tumor types are benign and are classified as World Health Organization grade I meningiomas.
Treatment and Follow-Up
Complete and subtotal resection of the tumor was achieved in 3/14 (21%) and 11/14 (79%) patients, respectively. The mean follow-up was 73.4 months (range, 4–192 months). Thirteen cases were followed up with MR imaging. Recurrence was identified in 7 patients, 3 patients did not have recurrence, and 3 patients who had subtotal resection did not show any progression of the tumor during the follow-up period (Table 3).
Treatment and follow-up results
Discussion
Epidural meningioma is a rare type that may originate from arachnoid cells on the nerve roots outside the dural sac,14 arachnoid cells located outside the dural sac,15 or the periosteum of the vertebra.16 The imaging features, biologic behavior, and prognosis of epidural meningiomas differ from those of intradural meningiomas. This study aimed to identify the characteristic features of epidural meningiomas.
Among the 14 patients with epidural meningiomas in the current study, the male/female ratio was 4:10 and the mean age was 44.9 years; this sex distribution and age are consistent with those in previous reports.10,17 In terms of tumor location, 12 tumors in this series were in the cervical spinal canal and 2 were in the thoracic spinal canal. This location is contrary to the findings of Frank et al,18 who reported that the thoracic spine is the typical location of epidural meningioma. However, like us, Wu et al19 also found the cervical spine to be the most common site of these tumors. In contrast, intradural meningiomas are typically located in the thoracic spinal canal.
Epidural meningiomas may be en plaque, dumbbell-shaped, or fusiform/ovoid. In the current study, 9 epidural meningiomas appeared as en plaque on the sagittal view; the ratio of en plaque to dumbbell-shaped and fusiform tumors was 9:4:1. In en plaque meningiomas, thickened dorsal and ventral dura encircled the spinal cord, forming a C-shape or half ring on the axial MR images. This sign was seen in 78% of our patients and, according to the literature, is common in en plaque meningiomas.8 Epidural meningioma may extend through the intervertebral foramen to the outer part of the spinal canal. This feature was seen in 10/14 (71%) tumors in the present study. The imaging appearance is like that of a neurogenic tumor. Intervertebral foraminal widening is mainly due to epidural growth pattern, and epidural meningioma is different from its intradural counterpart. Some investigators have suggested that there is proximity to the nerve root or intervertebral foraminal widening, mainly due to presence of arachnoid villi at the nerve root.20 Enlargement of the intervertebral foramen can be used to differentiate intradural meningioma and schwannoma,20 but it is difficult to distinguish epidural meningioma from schwannoma with this sign. Another characteristic of epidural meningiomas is calcification, which is uncommon in spinal intradural meningiomas. Radiologically visible calcification has been described in only 1%–4.6% of all spinal meningiomas.2 In this study, flaky calcification was observed in 8 epidural meningiomas (6 en plaque and 2 dumbbell-shaped). Calcification was mainly due to psammoma bodies, and it was present in 8 of the 10 psammomatous meningiomas. Epidural meningiomas may have different shapes and may be of different pathologic types, but all except 2 epidural meningiomas showed isointensity or hypointensity on T2WI, mainly due to the presence of calcification, psammomatous bodies, and interstitial collagen fibers, which tend to decrease the signal intensity. Epidural meningiomas commonly show moderate or marked enhancement, reflecting the good epidural blood supply.
The dural tail sign is commonly seen in meningiomas. It manifests as linear thickening and contrast enhancement of the meninges adjacent to the meningioma. In the current study, 13 (93%) meningiomas showed the dural tail sign on contrast-enhanced T1-weighted images. Wu et al19 described the dural tail sign in 75% of extradural en plaque meningiomas in their series of 12 patients. We found the dural tail sign to be common in epidural meningiomas. The dural tail sign is said to be present in 50%–60% of intradural meningiomas.20 Although this sign favors the diagnosis of extradural meningioma, it is not specific for this tumor and is also seen in other lesions such as metastases and lymphoma.
Epidural spinal meningiomas show more aggressive behavior than intradural meningiomas.21 Most epidural meningiomas, especially the en plaque type, often adhere to the dura. They show an epidural growth pattern and often display intradural invasion; consequently, the tumor boundary may not be clearly defined as in intradural meningiomas. In this study, only 2/14 (14%) tumors had clear boundaries. Epidural meningiomas can grow through the intervertebral foramen and involve an adjacent nerve root. In this series, 8 tumors showed intradural invasion on MR imaging and 11 tumors demonstrated adhesions to nerve roots during an operation. Tuli et al22 were the first to report invasion of nerve roots by epidural meningioma in a pathologic specimen. This behavior makes complete tumor removal difficult, and in our series, complete resection was achieved in only 3 of the 14 patients.
Postoperative recurrence of epidural meningioma is not rare. Rutherford et al23 reported 1 patient who had 2 recurrences. One of the 6 patients reported by Yao et al3 had a recurrence 6 years after surgery. In the current study, 7 of the 14 patients had postoperative recurrence between 5 and 192 months after the operation. Of these 7 cases, 1 was an infiltrated meningothelial-type meningioma; the risk of recurrence was high because this large-sized tumor had invaded adjacent muscles and complete resection was impossible. In the other 6 patients, the recurrences were due to close adherence of tumor to the dura or nerve roots, which made complete resection difficult to perform. In this study, the longest interval between the operation and recurrence was 192 months, which shows that long-term follow-up is particularly important in these patients. Many investigators have suggested that calcification of meningiomas is associated with tumor recurrence. In the present series, 5 of the 7 patients with recurrences had dural calcification; such calcification adds to the difficulty of complete removal of the tumor.24
Depending on the imaging findings and the shape of the epidural meningioma, the differential diagnosis could include spinal lymphoma, neurogenic tumor, angiolipoma, metastatic tumor, and ossification of ligament. En plaque epidural meningioma shows the same growth pattern and signal as a lymphoma. However, lymphomas are mostly observed on the ventral side of the dura and are characterized by formation of a paravertebral soft-tissue mass and infiltration of adjacent bone.25 Epidural meningiomas rarely destroy adjacent bone; they mostly cause bone compression and erosion.7 In this study, 5 patients had bone compression and reactive osteosclerosis, features that are more likely to be seen with benign tumors. Dumbbell-shaped epidural meningiomas should be differentiated from neurogenic tumor. Neurogenic tumors rarely show calcification, whereas punctuate calcification is common in epidural meningiomas. In addition, neurogenic tumors show heterogeneous enhancement, whereas meningiomas are characterized by homogeneous contrast enhancement.20 Fusiform meningioma needs to be differentiated from metastatic tumor and angiolipoma. A metastatic tumor is often accompanied by adjacent bone destruction and paravertebral involvement.26 An angiolipoma is hyperintense on T2WI, whereas most meningiomas are iso- or hypointense. The dural tail sign is also useful for identification of a meningioma. Ossification of the posterior longitudinal ligaments could be confused with an epidural meningioma; however, the former condition is not accompanied by dura thickening or enhancement.
Our study had several limitations. First, this was a retrospective study without a control group. Second, the number of patients was small; however, epidural meningioma is an uncommon entity, and ours is one of the largest studies to date. Third, T2-weighted gradient-echo images were not acquired; this acquisition would have been useful for differentiating these tumors from schwannomas.27 Fourth, intradural invasion was not confirmed pathologically. Finally, long-term clinical and MR imaging follow-up was not performed for all patients.
Conclusions
In this study, epidural meningioma was most common in middle-aged women. The cervical spinal canal was the most common location of the tumor. Tumor shape was en plaque, dumbbell, or ovoid/fusiform. Enlargement of the intervertebral foramen, adhesion to or infiltration of adjacent nerve roots, and intradural extension were common. CT revealed linear or flaky calcification in the dura mater. Epidural meningioma had isointense or hypointense signal on T2WI. The dural tail sign was common on postcontrast MR imaging. The psammomatous tumor was the most common pathologic type in this sample. Complete removal of tumor can be difficult because of encirclement and infiltration of the dura or an adjacent nerve root. Long-term follow-up is necessary to detect recurrence.
References
- Received May 24, 2017.
- Accepted after revision July 29, 2017.
- © 2018 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.