
We read with great interest the article recently published in the American Journal of Neuroradiology by Barreras et al1 entitled, “Analysis of 30 Spinal Angiograms Falsely Reported as Normal in 18 Patients with Subsequently Documented Spinal Vascular Malformations.” This very valuable article for the interventional neuroradiology and neurosurgical communities presents the causes of false-negative digital subtraction angiography findings for the depiction of spinal dural arteriovenous fistulas (SDAVFs). The authors found that the most frequent reason for missing a SDAVF on spinal DSA (sDSA) was misinterpretation of abnormal findings documented on the DSA (55.6%), followed by nonexploration of the ROI (29.6%), and, finally, inadequate opacification of the artery supplying the fistula (nonselective injection) (14.8%).
We congratulate the authors for their effort in seeking the reasons for false-negative DSA findings in the diagnosis of SDAVF and for emphasizing the need for a rigorous protocol for spinal DSA. While spinal DSA is the criterion standard examination for the diagnosis of SDAVF,2 it remains an operator-dependent examination, which can lead to false-negative results in a substantial number of cases due to potentially avoidable operator-related misinterpretations. Missing a SDAVF on DSA has a great impact on a patient's outcome because it may delay the treatment, thus reducing the chance of recovery.
In addition to the recommendations suggested by the authors (adoption of rigorous technical and training standards and second opinion reviews), we would like to share our experience and insist on the need for full spinal DSA, which includes systematically (from top to bottom and bilaterally) the following: costocervical trunks, vertebral arteries, intercostal arteries, lumbar arteries, medial sacral artery, iliolumbar arteries, and lateral sacral arteries (superior and inferior). We insist that all these arteries must be catheterized as selectively as possible. For instance, for the lateral sacral arteries, the catheterization of the internal iliac artery is not sufficient because proximal injection may lead to poor opacification of the lateral sacral arteries (Fig 1). In the article of Barreras et al,1 most of the missed fistulas (52.9%) were at or below the L4 level, which confirms the need for a complete spinal DSA, including the lower spinal supplies.

A 56-year-old man presenting with a progressive paraparesis lasting for a few months. Spinal cord MR imaging, sagittal T2-weighted imaging (A), and contrast-enhanced T1WI (B) demonstrate T2 hyperintensity involving the thoracolumbar spinal cord and the conus medullaris (A, white arrows), which may be suggestive of a SDAVF. However, no perimedullary vein enhancement on contrast-enhanced T1WI is seen (B). A first digital subtraction angiography was performed with a negative result for SDAVF (not shown). However, the internal iliac arteries were not catheterized during this first spinal DSA. A second sDSA was performed 3 months after the first one (C). The right internal iliac artery was catheterized, but too proximally. The sDSA findings were interpreted as normal. A second look revealed a possible fistula fed by the right superior lateral sacral artery (LSA) (C, arrow). D and E, Right internal iliac artery DSA in an anteroposterior projection. D, Early phase. E, Late phase, large FOV. The tip of the catheter is located close to the origin of the right LSA. The presence of a SDAVF is confirmed, fed by the right superior LSA (D, white arrow). The shunt point is located along the right S1 nerve root (asterisk) with low-flow ascending venous drainage (D and E, black arrows). Note the pre-anastomosis between a branch of the LSA (D, black arrowhead) and the medial sacral artery (D, white arrowheads).
Additionally, a cervical myelopathy may be observed in the case of an intracranial AVF with perimedullary venous drainage.3 Thus, a cerebral DSA with internal and external carotid artery catheterization and opacification should be performed secondarily in case of a negative sDSA finding.
In most cases of missed SDAVFs in the article of Barreras et al,1 the fistula was documented on the DSA but misinterpreted. Some conditions may enhance the quality of the images acquired during the sDSA, such as the intravenous injection of hyoscine or glucagon to reduce peristalsis-related artifacts or performing the sDSA with the patient under general anesthesia with provoked apnea during the runs to reduce the patient's motion artifacts.
A peculiar anatomic variation may also be responsible for a false-negative sDSA performed for SDAVF: a separate origin of the dorsospinal branch from the segmental artery on the aorta.4 Indeed, the dorsospinal branch (which usually gives rise to the radiculomeningeal branches) may not arise from the segmental artery but instead originate from the aorta. This anatomic variation can be suspected when no physiologic blush of the vertebral body is seen during the selective injection of the segmental artery (because the branches feeding the ipsilateral hemivertebral body are supplied by the dorsospinal trunk).
Furthermore, the catheterization of the origin of the segmental artery may be responsible for vasospasm. In case of a low-flow fistula, this spasm may reduce the flow toward the fistula, which could be responsible for the nonvisualization of the SDAVF.
Moreover, we stress that metachronous double dural AVFs,5 even if rare, may be observed. Thus, clinical recurrence after SDAVF treatment with negative sDSA findings at the SDAVF site should suggest performing a complete sDSA, looking for a second fistula.
Finally, the authors do not mention the potential of noninvasive/semi-invasive techniques such as time-resolved MR angiography6 or intra-aortic CT angiography (IA-CTA).7 These techniques potentially provide an overall examination of the whole spinal cord supply in a single acquisition. They may be valuable in patients with atheromatous vessels with stenosis at the origin of the intercostal/lumbar arteries, leading to difficult stable catheterization and thus to poor vessel opacification (Fig 2). However, while time-resolved MRA is sensitive for the depiction of SDAVFs (sensitivity as high as 81%6), the spatial resolution of this examination is limited and the precise location of the shunt point cannot be evaluated on time-resolved MRA in some cases.8 Concerning IA-CTA, despite its potential for the depiction of SDAVFs (sensitivity of 90%7) and the valuable information it provides regarding the location of the shunt point and its relationship with the bone landmarks, this examination may also provide false-negative results, mainly for SDAVFs supplied by branches from the internal iliac arteries, due to the incomplete opacification of the latter vessels by the contrast material injected directly in the aorta (Fig 1).
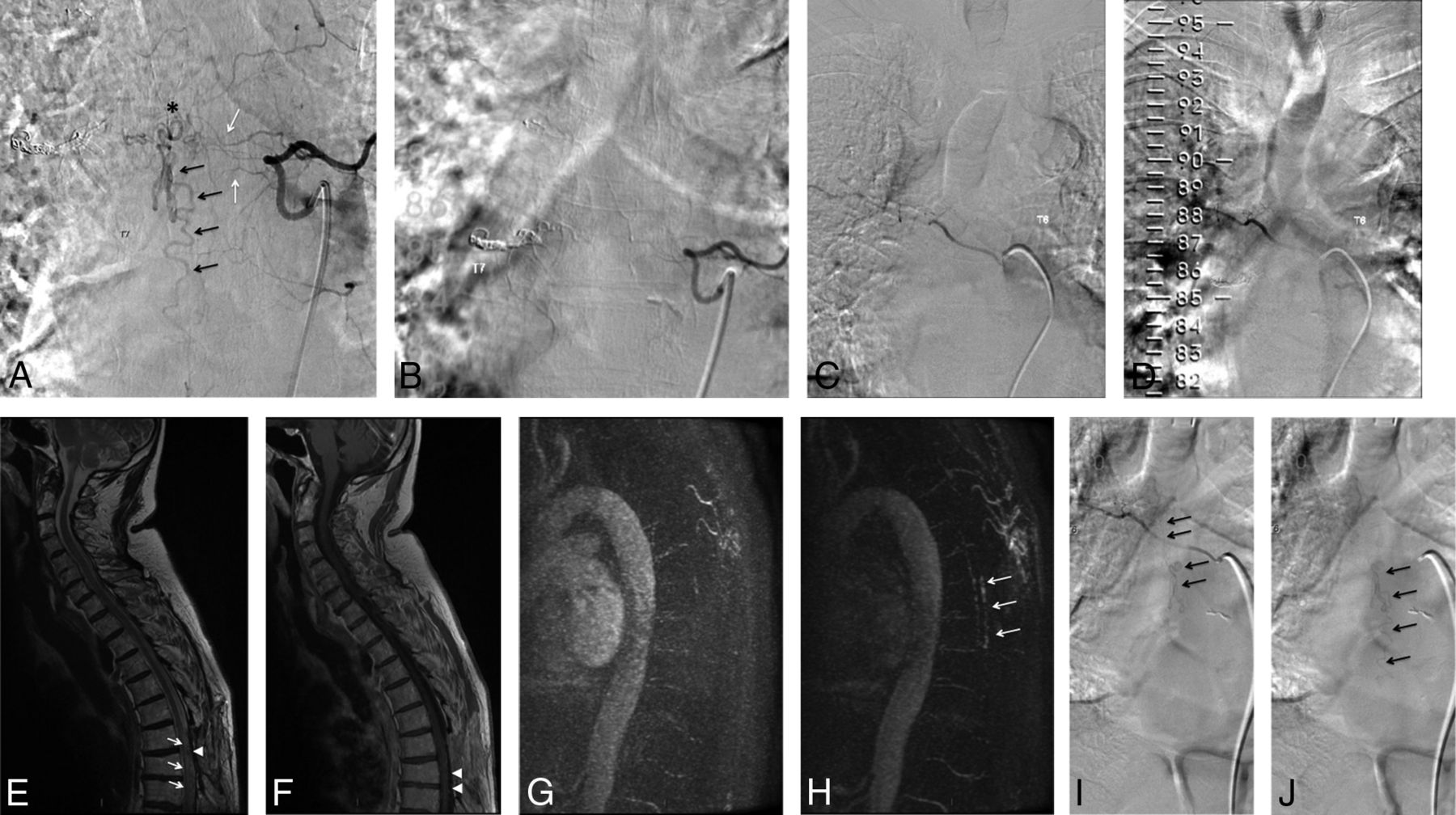
A 76-year-old man who had a previous embolization with coils and Onyx (Covidien, Irvine, California) for a right T7 SDAVF. Recurrence of the clinical symptoms (gait disturbance) was observed >1 year after the endovascular treatment. The spinal cord MR imaging (not shown) was suggestive of a recurrence of the fistula. An sDSA was performed (A) and confirmed the recurrence of the fistula (asterisk indicates the shunt point; black arrows, descending venous drainage), which was fed by the contralateral intercostal artery (left T7) via the retrocorporeal network (A, white arrows). The patient was referred for surgery for the treatment of this recurrence. After surgical treatment, the patient experienced a slight clinical worsening (ataxia). Within the 2 months after the surgical treatment, the patient continued to experience gradual clinical worsening (worsening of the ataxia with walking being impossible). A full sDSA was scheduled to rule out a recurrence of the SDAVF. The selective injection of the left T7 intercostal artery showed no residual fistula (B). The right T6 intercostal artery could not be catheterized selectively due to ostium stenosis, and the injection was performed in front of the origin of the intercostal artery (C, early phase; D, late phase). The sDSA findings were thus interpreted as normal. A spinal cord MR imaging was performed the day after the sDSA (E, sagittal T2WI; F, sagittal contrast-enhanced T1WI) and showed postoperative changes associated with spinal cord hyperintensity, suggestive of venous edema (E, white arrows). Equivocal posterior perimedullary serpiginous T2 hypointensities (E, arrowhead) presenting a doubtful enhancement were also seen (F, arrowheads), possibly corresponding to perimedullary vein dilations. Time-resolved MR angiography (Time Resolved Imaging of Contrast Kinetics, TRICKS; GE Healthcare, Milwaukee, Wisconsin), sagittal acquisition (G, early phase; H, late phase). Abnormal early perimedullary vein enhancement was seen (H, white arrows) at the midthoracic level, suggestive of sAVF recurrence (On-line Video). A new sDSA was performed with the patient under general anesthesia. Selective catheterization of the right T6 intercostal artery (I, early phase; J, late phase) confirmed the recurrence of the spinal DAVF with early opacification of dilated perimedullary veins (I and J, black arrows).
In conclusion, interventional neuroradiologists and neurologists should keep in mind that a single negative spinal DSA finding is not enough to rule out a spinal vascular malformation and therefore should be repeated with enhanced acquisition protocol if the clinical presentation is strongly suggestive of a SDAVF.
Footnotes
Disclosures: Frédéric Clarençon—UNRELATED: Payment for Lectures Including Service on Speakers Bureaus: Balt Extrusion, Medtronic. David Grabli—UNRELATED: Board Membership: AbbVie, Zambon; Employment: Assistance Publique-Hôpitaux de Paris; Grants/Grants Pending: Assistance Publique-Hôpitaux de Paris, Institut National de la Santé et de la Recherche Medicable, France Parkinson*; Payment for Lectures Including Service on Speakers Bureaus: Novartis, Merz, Pharma AbbVie, Teva; Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: AbbVie, Merz Pharma. Nader-Antoine Sourour—UNRELATED: Consultancy: Medtronic, MicroVention; Stock/Stock Options: Medina. *Money paid to the institution.
References
- © 2018 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.