
Abstract
BACKGROUND AND PURPOSE: Percutaneous radiofrequency ablation combined with vertebral augmentation has emerged as a minimally invasive treatment for patients with vertebral metastases who do not respond to or have contraindications to radiation therapy. The prevalence of posterior vertebral body metastases presents access and treatment challenges in the unique anatomy of the spine. The purpose of this study was to evaluate the safety and efficacy of simultaneous bipedicular radiofrequency ablation using articulating bipolar electrodes combined with vertebral augmentation for local tumor control of spinal metastases.
MATERIALS AND METHODS: Imaging-guided simultaneous bipedicular radiofrequency ablation combined with vertebral augmentation was performed in 27 patients (33 tumors) with vertebral metastases selected following multidisciplinary consultations, to achieve local tumor control in this retrospective study. Tumor characteristics, procedural details, and complications were documented. Pre- and postprocedural cross-sectional imaging was evaluated to assess local tumor control rates.
RESULTS: Thirty-three tumors were successfully ablated in 27 patients. Posterior vertebral body or pedicle involvement or both were present in 94% (31/33) of cases. Sixty-seven percent (22/33) of the tumors involved ≥75% of the vertebral body volume. Posttreatment imaging was available for 79% (26/33) of the treated tumors. Local tumor control was achieved in 96% (25/26) of tumors median imaging follow up of 16 weeks. No complications were reported, and no patients had clinical evidence of metastatic spinal cord compression at the treated levels.
CONCLUSIONS: Simultaneous bipedicular radiofrequency ablation combined with vertebral augmentation is safe and effective for local tumor control of vertebral metastases. Articulating bipolar electrodes enable the placement and proximity necessary for optimal confluence of the ablation zones. Local tumor control may lead to more durable pain palliation, prevent disease progression, and reduce skeletal-related events of the spine.
ABBREVIATIONS:
- RF
- radiofrequency
- RFA
- radiofrequency ablation
Approximately 1.7 million patients are diagnosed with cancer in the United States annually, most of whom will develop metastases that in 40% of cases will involve the spine.1,2
The vertebral column is the most common site of osseous metastasis as a result of vascular red marrow in adult vertebrae and communication of valveless vertebral venous plexuses with deep torso veins.3 Approximately 90% of symptomatic patients with vertebral metastases present with pain due to pathologic fracture, biochemical stimulation of endosteal nociceptors, osteoclast-mediated osseous destruction, and spinal cord or nerve root compression, which occur in 10%–20% of patients and are most often due to tumor involvement of the posterior vertebral body.4,5 Pain and neurologic deficits associated with vertebral metastases often lead to impaired mobility, deficient functional independence, and overall diminished quality of life.6 Management of metastatic spine disease requires multidisciplinary input.7
Radiation therapy is the current standard of care for local control and pain palliation of vertebral metastases, but when used alone, it has important limitations. First, certain tumor histologies respond less favorably to radiation therapy, such as sarcoma, renal cell carcinoma, non-small cell lung cancer, and melanoma.8 Second, radiation therapy of vertebral metastases is limited by the cumulative tolerance of the spinal cord, which often precludes retreatment of recurrent tumor or progressive tumor at adjacent vertebrae.9 Last, radiation therapy excludes patients from certain systemic chemotherapy clinical trials. Surgery (including stabilization, corpectomy, and gross tumor resection) is often of limited benefit in the management of spinal metastases due to its morbidity and patients' often poor functional statuses and short expected life span, and is typically considered for patients with neurologic compromise or spinal instability.
During the past few years, investigators have exploited minimally invasive percutaneous thermal ablation technologies, often combined with vertebral augmentation, for pain palliation and local tumor control of vertebral metastases. These may be performed in an outpatient setting with the patient under conscious sedation with short recovery and no compromise of adjuvant radiation or chemotherapy.10⇓⇓⇓⇓⇓–16 Percutaneous thermal ablation for vertebral metastases is performed to achieve pain palliation, local tumor control, or both (often with vertebral augmentation for fracture stabilization or prevention) in patients who have not responded to or have contraindications to radiation therapy.
There has been a recent paradigm shift in stereotactic spine radiosurgery for management of vertebral metastases with specific consensus recommendations by the International Spine Radiosurgery Consortium for the definition of clinical target volume versus gross tumor volume to account for microscopic tumor spread and marginal radiation therapy failures.17 The consensus recommendations define clinical target volume (to be treated by stereotactic spine radiosurgery) to include gross tumor volume plus surrounding abnormal bone marrow signal intensity on MR imaging to account for microscopic tumor invasion and adjacent normal osseous expansion to account for subclinical tumor spread in the marrow space.17 For example, tumor involving the posterior vertebral body would involve treating the entire vertebral body and both pedicles (Fig 1).
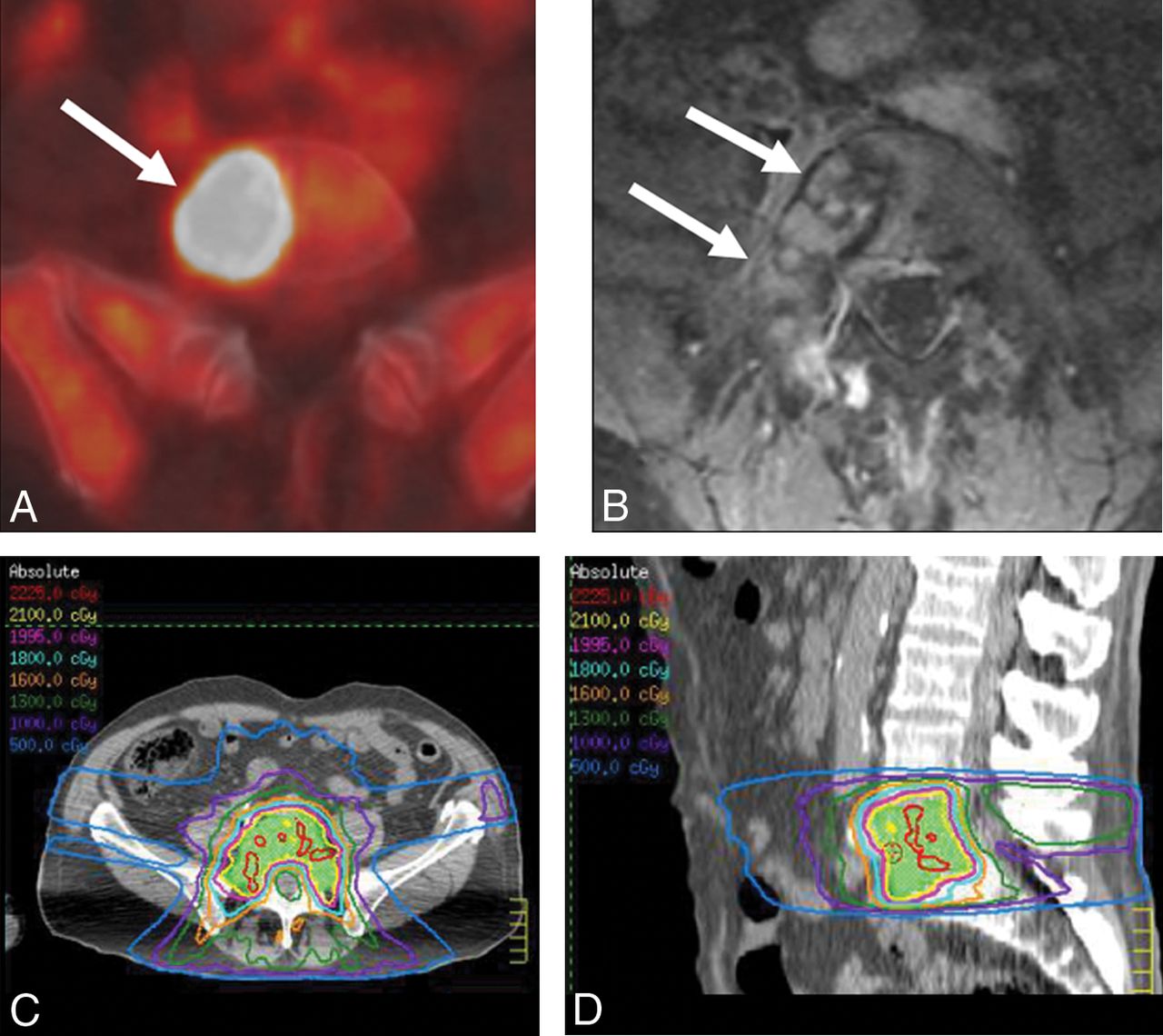
A 63-year-old man with chest wall melanoma and painful L5 metastasis. Axial FDG-PET/CT (A) and axial T1-weighted fat-saturated contrast-enhanced MR imaging (B) show hypermetabolic bone marrow replacing lesion in the L5 vertebral body extending to the right pedicle (A and B, arrows). Axial (C) and sagittal (D) stereotactic body radiation therapy planning CT images show stereotactic body radiation therapy contours with clinical target volume including the entire vertebral body and pedicles.
Simultaneous bipedicular radiofrequency ablation (RFA) is a novel technique that efficiently generates 2 confluent, coalescent, and overlapping ablation zones in close proximity that minimize the convective cooling effect (heat sink) and subsequently decrease the power required to conduct heat through tissue, decreasing the risk of thermal injury and minimizing charring and impedance-related issues. This technique may result in a more thorough ablation of the vertebral body and pedicles and supports the stereotactic spine radiosurgery paradigm to treat the entire vertebral body volume and pedicles (clinical target volume) for improved local tumor control rates and more durable pain palliation (Figs 1 and 2). However, the combination of transpedicular access being the safest approach to the vertebral body and the high prevalence of posterior vertebral body metastases (>95% of cases)18 makes minimally invasive access and treatment challenging.

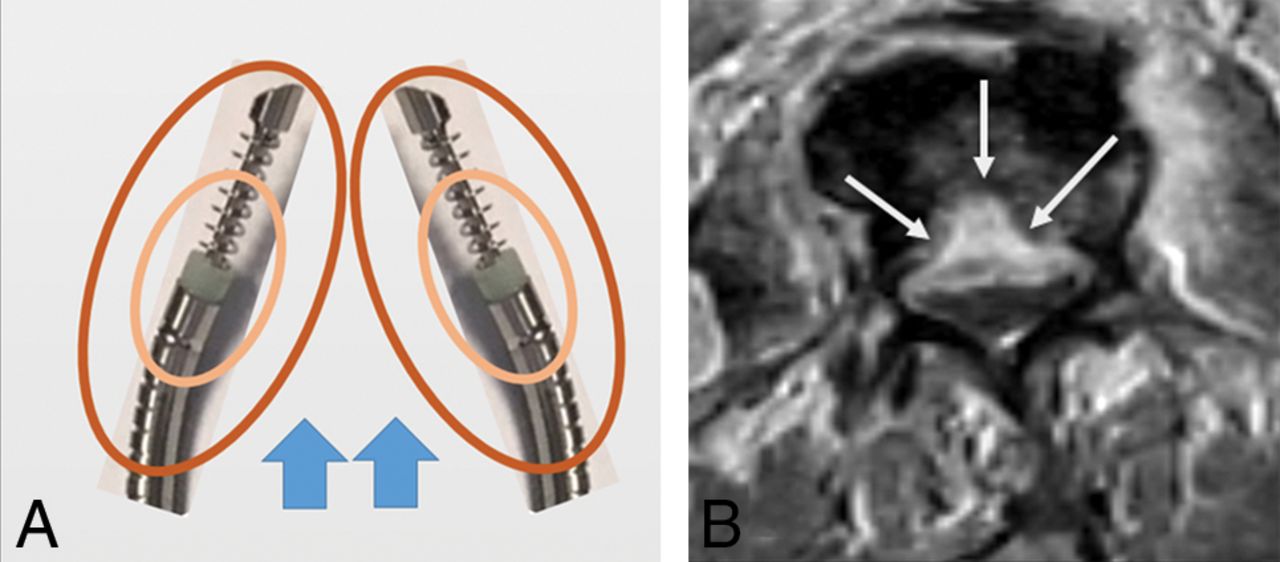
Illustration of simultaneous bipedicular RF ablation (A) depicts individual zones of resistive and conductive heating (central and peripheral ovoids, respectively) around 2 adjacent RF electrodes, resulting in a diminished convective cooling effect (ie, heat sink due to blood and CSF flow) (A, arrows). Adjacent areas of thermal spread result in reduction in the power required to conduct heat in tissue, decreased risk of thermal injury, and impedance-related issues. Axial T1-weighted fat-saturated contrast-enhanced MR imaging (B) following bilateral RF ablation using 2 straight electrodes shows ablation failure along the posterior third vertebral body centrally due to lack of confluent ablation zones (B, arrows).
The purpose of this study was to evaluate the safety and efficacy of simultaneous bipedicular RFA using a navigational bipolar electrode system combined with vertebral augmentation for local tumor control of vertebral metastases.
Materials and Methods
Institutional review board approval was obtained to retrospectively review the institutional data base for all patients who underwent simultaneous bipedicular RFA and vertebral augmentation of vertebral metastases between May 2016 and July 2017 at a National Cancer Institute–designated Cancer Center.
Informed consent was waived for this retrospective study. Recorded data included patient demographics, primary tumor histology, vertebrae treated, and whether the lesion had been previously treated with radiation therapy. Available preprocedural cross-sectional imaging of each treated vertebra was reviewed to determine whether the tumor involved the posterior vertebral body and/or pedicles, had involved the posterior vertebral body cortex, and/or was associated with a pathologic vertebral fracture.
Procedural notes were reviewed to determine the total conscious sedation time and total ablation time for each radiofrequency (RF) electrode at each vertebral level. Procedural complications were documented according to the Society of Interventional Radiology classification.19 Patients were clinically evaluated 2 hours after each procedure for evidence of acute complications, such as hematoma formation or neurologic injury, with routine follow-up by telephone 1 day, 1 week, and 1 month following the procedure. The duration of imaging follow-up was recorded for all patients, and electronic medical records were reviewed for possible delayed complications, such as infection.
Patient Selection for Radiofrequency Ablation and Vertebral Augmentation
Patients were selected for RFA and vertebral augmentation by a multidisciplinary team of radiation and medical oncologists, interventional radiologists, and spine surgeons. Treatments were performed to achieve local tumor control and, in most cases, pain palliation. Patients selected for RFA treatment were either unable to undergo radiation therapy or had radiographic evidence of tumor progression at other sites of disease previously treated with radiation therapy. Exclusion criteria for RFA and vertebral augmentation included entirely osteoblastic metastases, the presence of pathologic compression fracture with spinal instability, or metastases causing spinal cord compression.
Radiofrequency Ablation and Vertebral Augmentation Procedure
Written informed consent was obtained before all procedures. All procedures were performed using fluoroscopic guidance with patients under conscious sedation. Conscious sedation was decreased from moderate-to-mild sedation during the ablation portion of the procedure so that the patient could provide active biofeedback to prevent thermal nerve and or spinal cord injury. The vertebral body was accessed from a bipedicular approach with 10-ga introducer working cannulas, and a navigational osteotome was used to create channels in the marrow space along the planned placements of the ablation electrodes.
The ablation electrodes were then placed through both introducer cannulas and articulated until the tips were 5–10 mm apart as seen on the anteroposterior fluoroscopic images (approximately 1 width of the spinous process) (Fig 3). The first ablation was performed anteriorly, and the electrodes were then retracted and articulated within the posterior third of the vertebral body re-establishing the 5- to 10-mm tip distance, to treat the posterior vertebral body and pedicles. In each case, the goal was to generate confluent, coalescent, and overlapping ablation zones to encompass the entire vertebral body (and pedicles) to treat the clinical target volume in alignment with the International Spine Radiosurgery Consortium consensus recommendations.17
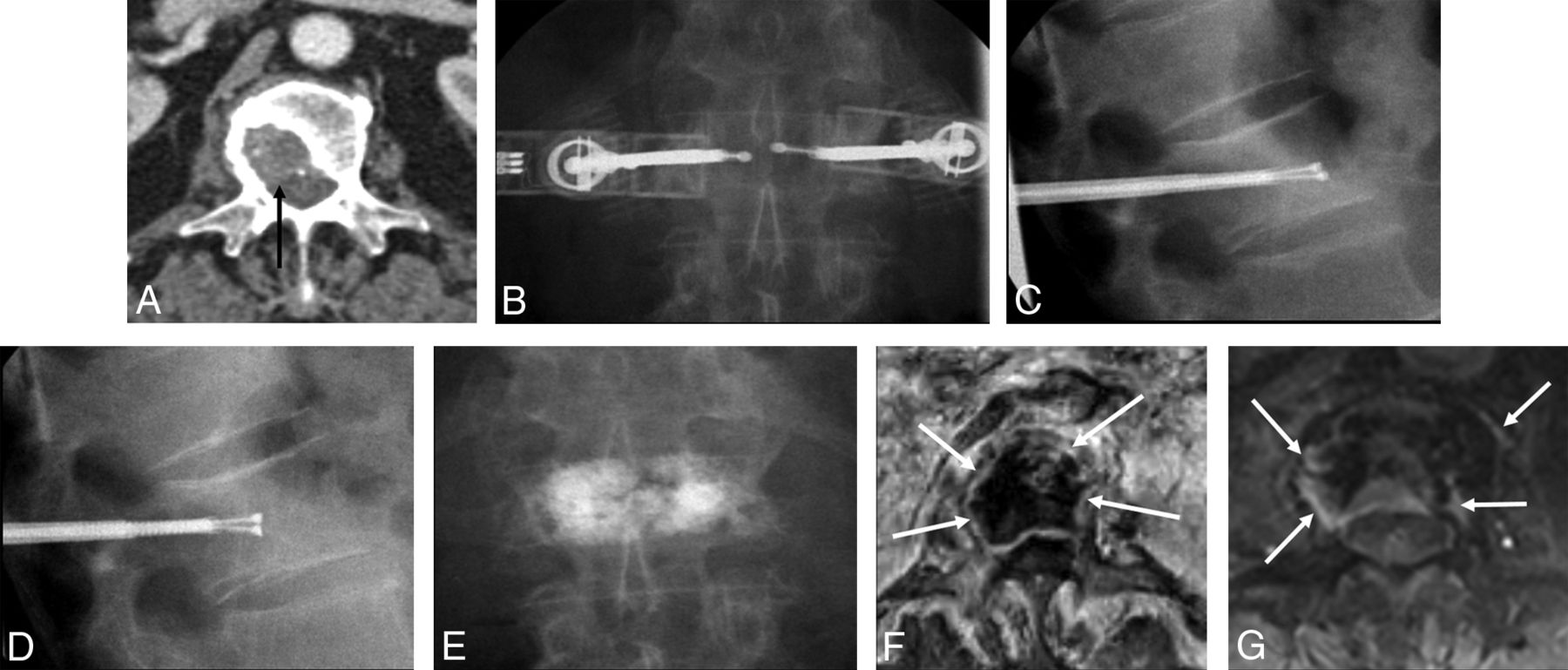
An 86-year-old man with metastatic melanoma and a painful L1 lesion. Axial contrast-enhanced CT (A) shows a destructive osteolytic mass within the vertebral body with partial disruption of the posterior wall and a small component extending to the anterior central canal (A, arrow). An anteroposterior fluoroscopic image during simultaneous bipedicular RF ablation (B) shows medial articulation of electrode tips, which are 5–10 mm apart (the width of the spinous process as a landmark). Lateral fluoroscopic images (C–E) show ablation of the anterior vertebral body first (C), followed by ablation of the posterior vertebral body and pedicles (D), and vertebral augmentation (E). Axial T1-weighted fat-saturated contrast-enhanced MR images obtained 2 weeks (F) and 52 weeks (G) following treatment show local tumor control with granulation tissues along the periphery of ablation zone (F and G, arrows).
Simultaneous bipedicular RF ablations were performed with the STAR Tumor Ablation System (Merit Medical Systems, South Jordan, Utah) consisting of the 10/15 STAR ablation electrode and the MetaSTAR generator. The ablation device is a navigational bipolar electrode with an articulating distal segment that can be curved in various projections providing optimal lesion access and electrode proximity, both essential for accessing and ablating tumor in the posterior central vertebral body.12,16 The electrode contains 2 active thermocouples embedded along its shaft 10 and 15 mm from the center of the ablation zone. These permit real-time monitoring of the temperatures at the periphery of the developing ablation zone, allowing accurate, intraprocedural assessment of the ablation zone size and providing passive thermal protection, which is especially important when treating the posterior vertebral body and pedicles. Based on the manufacturer's thermal distribution curves, the dimensions of the ellipsoid ablation volume are 20 × 15 × 15 mm when the thermocouple located 10 mm from the center of the ablation zone (distal thermocouple) reaches 50°C and 30 × 20 × 20 mm when the thermocouple located 15 mm from the center of the ablation zone (proximal thermocouple) reaches 50°C. The radiofrequency energy automatically stops when the proximal thermocouple registers 50°C, which is a valuable safety feature. Each individual ablation was performed until the proximal thermocouple registered 50°C, at which point the ablation was considered technically successful. The MetaSTAR generator provides 3-, 5-, 7.5-, and 10-W power settings, which allow slow ramping of temperatures and ablation size, improving efficacy and reducing undesired heat dispersion and impedance issues. Ablation is initiated at the 3-W setting until the temperatures registered at the thermocouples' plateau. The power is then sequentially increased using an identical strategy until the desired ablation volume is achieved. The generator displays ablation time, impedance, and the 2-thermocouple temperature readings, which allows precise real-time monitoring of the ablation zone geometry.
Vertebral augmentation was performed using the StabiliT Vertebral Augmentation System (Merit Medical Systems). In all cases, cement was injected through the same working cannulae used for ablation.
Local Control Assessment and Analysis
All available postprocedural cross-sectional imaging was reviewed to determine the ablation extent, degree of local tumor control, possible complications, and evidence of systemic disease progression.16,20 Local control failure was determined in accordance with previously established guidelines following thermal ablation of spinal metastases.16,20
Results
All RF ablation procedures were performed via a bipedicular approach as preoperatively planned and were technically successful. Thirty-three spinal metastases (in 27 patients, 17 men and 10 women; age range, 23–86 years) treated with simultaneous bipedicular RFA and vertebral augmentation were included in the study. Radiation-resistant histologies composed 70% (23/33) of treated tumors, including non-small cell lung cancer (30.3%, 10/33), sarcoma (18.2%, 6/33), renal cell carcinoma (12.1%, 4/33), and melanoma (9.1%, 3/33). Other histologies included multiple myeloma (6.1%, 2/33), epithelioid hemangioendothelioma (6.1%, 2/33), hepatocellular carcinoma (3%, 1/33), head and neck squamous cell carcinoma (3%, 1/33), breast adenocarcinoma (3%, 1/33), bladder carcinoma (3%, 1/33), prostate adenocarcinoma (3%, 1/33), and germ cell tumor (3%, 1/33). Thirty-six percent (12/33) of tumors involved thoracic vertebrae, 61% (20/33) involved lumbar vertebrae, and 3% (1/33) involved sacral vertebrae. Posterior vertebral body and/or pedicle involvement was present in 94% (31/33) of cases. Three percent (1/33) of tumors exclusively involved the pedicles. Sixty-seven percent (22/33) of tumors involved ≥75% of the vertebral body volume. Twenty-four percent (8/33) of lesions in 7 patients were treated with spinal radiation therapy before RFA.
The mean total ablation time per RF electrode was 18.3 minutes (range, 9.9–29.3 minutes). The mean total conscious sedation time was 102.6 ± 25.8 minutes (range, 55–168 minutes). According to the Society of Interventional Radiology classification, there were no acute or delayed procedure-related complications.
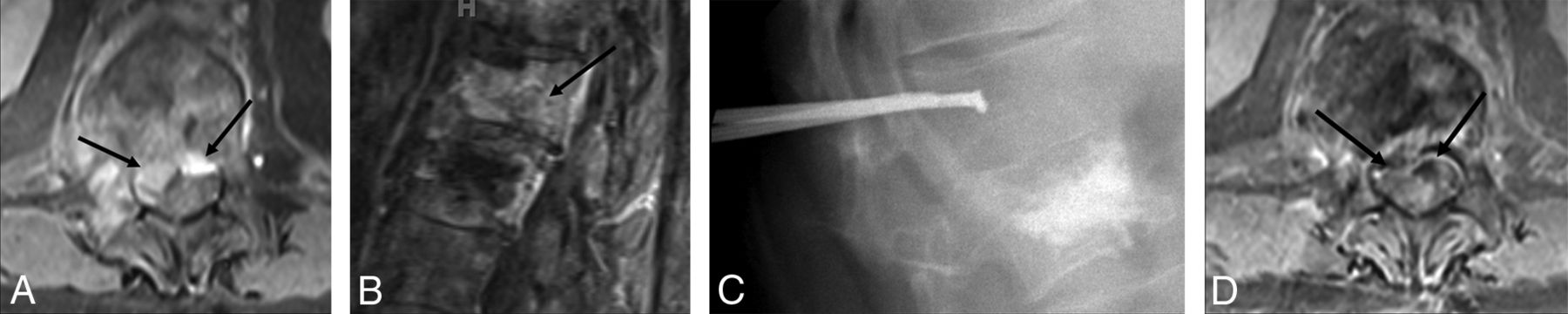
Follow-up imaging was available for 79% (26/33) of tumors in 23 of 27 patients and included MR imaging in 42% (14/33), CT in 52% (17/33), and PET/CT in 15% (5/33) of tumors. Follow-up imaging demonstrated local tumor control for 96% (25/26) of lesions (22 of 23 patients) with no evidence of residual or recurrent tumor during the median imaging follow-up of 16 weeks (range, 1–57 weeks; interquartile range, 29.5 weeks) (Fig 3). The patient thought to have progression had slightly more epidural tumor from the preoperative to the initial postoperative CT scan; however, it did not progress and remained unchanged at the 52-week follow-up in the setting of metastatic disease progression. Retraction of the epidural component of the tumor was identified in 3 lesions (Fig 4). On the basis of follow-up imaging, systemic metastatic disease progression was identified in 77% (17/22) of patients with local tumor control. Eight patients eventually died due to other causes, without symptoms of metastatic spinal cord compression, and 2 patients entered hospice care due to progression of visceral or intracranial metastatic disease.

A 70-year-old man with thigh metastatic undifferentiated pleomorphic sarcoma and a painful T12 lesion. Axial and sagittal T1-weighted fat-saturated contrast-enhanced MR images (A and B, respectively) show bone marrow replacing lesion in the T12 vertebral body with posterior wall destruction, epidural extension of tumor, and thecal sac compression (A and B, arrows). Note the previously treated L1 lesion (B). Lateral fluoroscopic image during simultaneous bipedicular RF ablation (C) shows aggressive ablation of the posterior vertebral body and pedicles. Axial T1-weighted fat-saturated contrast-enhanced MR image (D) obtained 30 weeks following treatment shows local tumor control with no evidence of recurrence and retraction of epidural component (D, arrows).
Discussion
In the present study, simultaneous bipedicular RFA and vertebral augmentation achieved a radiographic local tumor control rate of 96% (25/26 tumors), with a median follow-up of 16 weeks with no immediate or delayed complications. Systemic metastatic disease progression was identified in 77% (17/22) of patients with local tumor control. These results support the clinical value of a novel percutaneous thermal ablation approach for management of vertebral metastatic disease that adapts consensus recommendations by the International Spine Radiosurgery Consortium to treat clinical target volumes (entire vertebral body and pedicles if there is posterior vertebral body involvement), to account for microscopic tumor spread and marginal treatment failures for improved local tumor control rates.17
Although radiation therapy is the standard of care for palliation and local control of osseous metastases, simultaneous bipedicular RFA and vertebral augmentation may be a robust and safe alternative for patients who cannot be offered or cannot tolerate radiation therapy or have radiation-resistant tumors.
Simultaneous bipedicular RFA performed with an articulating device that permits optimal electrode placement has several important advantages: First, it effectively generates confluent and coalescent ablation zones at any given time to encompass as much vertebral volume as possible. This ablation zone is characterized by 2 regions of resistive and conductive heating in close proximity with the consequent reduction of the convective cooling effect (heat sink) (Fig 2).
Second, it minimizes the risk of undesired thermal injury by decreasing the power required to conduct heat through tissue via reduction of the temperature difference between regions of resistive heating and adjacent tissue, thus decreasing the distance that heat must be conducted. Consequently, there is less undesired heat propagation beyond the margins of ablation zones to generate the same ablation geometry compared with single-electrode RFA. This setup affords implementation of a low-power wattage protocol (with gradual increase in power), which also results in a decreased incidence of increased impedance, subsequently improving efficiency. Third, simultaneous ablation results in time savings and efficient treatment. In addition, the use of a bipolar navigational RF electrode system provides optimal tumor access, particularly within the posterior central vertebral body where access may be challenging using straight electrodes.12,16 Finally, in cases of challenging pedicle anatomy, the articulation can help anchor the electrode in position. This constellation of advantages is particularly important for treatment of tumors in the posterior vertebral body, which is involved in >95% of vertebral metastases.18 In these cases, aggressive ablation may be challenging due to proximity to the central canal and nerve roots and the associated risk of thermal injury, which increases the possibility of tumor recurrence and inadequate ablation. Similarly, based on dosimetry, the efficacy of radiation therapy declines with decreasing distance between the tumor and the spinal cord because of the risk of radiation-induced myelopathy.9
In a retrospective single-center study, Wallace et al10 used combination RFA and vertebral augmentation for the management of spinal metastases and reported local tumor control rates of 74% and 70% at 6-month and 1-year follow-up time points. The authors reported that in 89% (8/9 cases) of cases in which radiographic local tumor control was not achieved, residual or recurrent tumor was present in the posterior vertebral body or epidural space.10 A combination of radiation therapy and RFA has been used for improved local control rates of vertebral metastases.21 In a retrospective single-center study, Greenwood et al21 reported a local tumor control rate of 92% (12/13 tumors) at 3-month follow-up despite systemic metastatic disease progression. In the present study, 94% (31/33) of tumors involved the posterior vertebral body and/or the pedicles, and a local tumor control rate of 96% (25/26 tumors) was achieved. The safety of the procedure was supported by a lack of complications based on the Society of Interventional Radiology guidelines. Specifically, there were no thermal nerve or spinal cord injuries.
It is our practice to ablate as much vertebral body volume as possible plus the pedicles to account for microscopic tumor invasion and subclinical tumor spread in marrow space for improved local tumor control.17 We perform spinal RFA with patients under conscious sedation, in part, to allow patients to express new radicular pain indicating impending spinal nerve or potential spinal cord injury. In such cases, ablation is immediately terminated to avoid thermal nerve injury. Active thermal protective techniques including perineural and epidural injections of carbon dioxide and/or 5% dextrose in water are then attempted. If these are unsuccessful, the result is often less thorough tumor ablation. Of note, these active thermoprotective techniques were not necessary in this group of patients, and it is theorized that this feature may be, in part, due to the ability to use lower wattages, 5W and 3W, when ablating posteriorly near the spinal canal and neuroforamina. The difficulty in achieving maximum benefit of simultaneous bipedicular ablation includes the requirement for optimal positioning of dual RF electrodes, which may be difficult due to operator inexperience, challenging anatomy, and /or suboptimal imaging guidance.
The limitations of the present study include the single-arm nature of the analysis with no control group, the retrospective methodology, the relatively small number of treated tumors, and the lack of standard follow-up imaging protocol.
Conclusions
The results of this single-center retrospective study suggest that simultaneous bipedicular RF ablation using bipolar, articulating electrodes and the generation of confluent, coalescent, and overlapping vertebral body ablations, combined with vertebral augmentation, is safe and effective for local tumor control of vertebral metastases. The goal of treating the clinical target volume (the entire vertebral body and pedicles) in those with posterior vertebral body and pedicle lesions and achieving local tumor control may lead to more durable pain palliation, prevent disease progression, and reduce spinal skeletal related events.
Footnotes
Disclosures: Travis J. Hillen—UNRELATED: Other: helped with cadaver lab training course sponsored by DFine. Jack W. Jennings—RELATED: Consulting Fee or Honorarium: Merit Medical, Comments: ablation training labs and a few talks at national/international meetings regarding spine ablation; UNRELATED: Board Membership: Medtronic, Merit Interventional Oncology Advisory Boards, Comments: They have only met 1 time for each; Consultancy: Bard, BTG, Comments: BTG was for Principal Investigator fees.
References
- Received May 7, 2018.
- Accepted after revision June 18, 2018.
- © 2018 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}