
Abstract
BACKGROUND AND PURPOSE: Flow disruption with the Woven EndoBridge is increasingly used for the treatment of intracranial aneurysms. We examined factors leading to aneurysm occlusion and Woven EndoBridge shape change during a midterm follow-up.
MATERIALS AND METHODS: Patients with a minimum 12-month angiographic follow-up were included. Through a univariate and multivariate analysis, independent predictors of adequate occlusion (Raymond-Roy 1/Raymond-Roy 2) and Woven EndoBridge shape change (decrease of the height of the device) were assessed.
RESULTS: Eighty-six patients/aneurysms were included. The aneurysm mean size was 5.5 mm (range, 3–11.5 mm). The most common locations were the MCA (43/86 = 50%), basilar tip (13/86 = 15.1%), and anterior communicating artery (12/86 = 14%). Twenty-one patients (21/86 = 24%) had acute SAH. Immediate and long-term Raymond-Roy 1/Raymond-Roy 2 occlusion rates were 49% (42/86) and 80% (68/86), respectively. Woven EndoBridge shape change was detected among 22% (19/86) of cases. At binary logistic regression, wide ostium (≥4 mm) (OR = 0.2; 95% CI, 0.01–1; P = .04) and regular aneurysm morphology (OR = 5.9; 95% CI, 1.4–24; P = .01) were independent factors of incomplete and adequate aneurysm occlusion, respectively. In addition, irregular morphology (OR = 5.4; 95%CI, 1.4–19; P = .01) and a wide ostium (OR = 9.8; 95% CI, 1.6–60; P = .03) significantly increased the probability of the Woven EndoBridge shape change. Decrease of the Woven EndoBridge height was more common among incompletely occluded aneurysms (6/12 = 50% versus 13/74 = 17.5%), but it was not an independent prognosticator of occlusion at the multivariate model.
CONCLUSIONS: The likelihood of good occlusion was 5 times lower in the presence of a wide ostium, whereas aneurysms with regular morphology were 6 times more likely to be occluded. Woven EndoBridge shape modification was strongly influenced by the aneurysm shape and ostium size, and it was not independently associated with the angiographic occlusion.
ABBREVIATIONS:
- AcomA
- anterior communicating artery
- BT
- basilar tip
- RR
- Raymond-Roy
The efficacy and safety of the Woven EndoBridge device (WEB; Sequent Medical, Aliso Viejo, California) have been largely evaluated by several multicentric trials.1 Treatment with the WEB resulted in approximately 80% of complete/near-complete occlusion in many published series.1⇓–3 However, as reported in some recent studies,2,4 aneurysm recurrence and WEB compaction may occur in nearly 8% and 40% of patients, respectively. Despite the increased operator experience and the better patient selection, factors leading to aneurysm occlusion, recanalization, or WEB shape modification are not fully understood. Very few studies explored patient and aneurysm characteristics potentially associated with the angiographic results after WEB implantation. Our study aimed to investigate independent predictors of adequate aneurysm occlusion and WEB shape modification among 86 patients/aneurysms available during midterm angiographic follow-up.
MATERIALS AND METHODS
Patient Selection
Our hospital institutional review board approved this retrospective study. A prospectively maintained data base of WEBs (2014–2019) was retrospectively reviewed by 2, and in case of inconsistency, by 3 investigators independently. We included patients with aneurysms (unruptured or ruptured) treated with the WEB and available at midterm angiographic follow-up (at least 12 months). To assess factors associated with midterm aneurysm occlusion, we excluded patients with a radiologic follow-up of <12 months. Recanalized aneurysms for which the WEB was used as retreatment strategy were excluded. Indications for treatment were made by multidisciplinary consensus (vascular neurosurgeons, interventional neuroradiologists).
Indications for WEB
The selection of aneurysms treated with the WEB was performed by interventional neuroradiologists according to aneurysm characteristics and available sizes of the device. The main indications for WEB treatment were the following: 1) unruptured and ruptured wide-ostium aneurysms difficult to treat with simple coiling; 2) aneurysms located at bifurcation points not amenable to treatment with coiling or balloon-assisted coiling and where a flow diverter may lead to the risk of covering bifurcation branches or perforators. In addition, due to the progressive enlargement of WEB indications5 and on the basis of our own positive results, some small-neck or small-sized aneurysms were treated with the WEB.
Antiplatelet Therapy
For unruptured aneurysms, patients were premedicated with dual antiplatelet therapy in case of a strategy shift to stent-assisted technique (aspirin, 75 mg, and clopidogrel, 75 mg, starting 5 days before treatment). Daily aspirin administration was continued for 1 month. In case of additional stent placement, the dual antiplatelet therapy was maintained for 3 months, and on the basis of the clinical and radiologic evaluation, the patients were switched to aspirin. The VerifyNow P2Y12 assay (Accumetrics, San Diego, California) was used to test the platelet inhibition (P2Y12 reaction unit). Concurrent with the procedure, intravenous heparinization was performed (activated clotting time of >250 seconds).
For ruptured aneurysms, apart from heparin in the pressure bags for flushing (1000 IU/L), no antiplatelet therapy was used. In case of stent placement, an intravenous bolus of abciximab (0.125 mg/kg) was administered before stent deployment, and standard dual antiplatelet therapy was started the day after.
Description of Technique
With the patient under general anesthesia, via a transfemoral approach, access to the aneurysm was obtained in a triaxial fashion. Through a long femoral sheath, a 6F guiding catheter was advanced into the carotid artery. The WEB was delivered under roadmap guidance through the dedicated VIA microcatheter (Sequent Medical). Most of the implanted WEBs were single-layer (SL): accordingly, we included only SL devices. VasoCT (Philips Healthcare, Best, the Netherlands) with diluted iodinated contrast medium was used to assess WEB apposition.
Selection of WEB Size
Size selection derived from the measurements of the aneurysm on 3D rotational angiography (width and height of the dome outside of additional blebs and daughter aneurysms). In general, on the basis of the rule of the manufacturer, the device was chosen adding 1 mm to the average width (to ensure good wall apposition) and subtracting 1 mm from the average height of the aneurysm (to adjust for the longitudinal increase caused by the horizontal compression).6 Starting in 2017, WEB devices were selected using a computer-based-simulation modeling tool (Sim&Size software; Sim&Cure; Grabels, France).
Imaging Assessment
Anatomic and angiographic results were independently evaluated by 2 interventional neuroradiologists not directly involved in patient treatment. A senior interventional neuroradiologist solved discrepancies.
Aneurysm occlusion and WEB shape modification were evaluated on the DSA performed at least at 12-month follow-up. The aneurysm occlusion rate was defined on the basis of the Raymond-Roy (RR) classification: complete occlusion (class 1), residual ostium (class 2), and residual aneurysm (class 3).7
After WEB deployment, the size of the device was evaluated as “adequate” or “undersized.” There were no cases of oversized devices resulting in WEB protrusion over the ostium. A detailed definition of undersized and adequately sized devices is reported in the On-line Appendix.
Aneurysm shape was dichotomized into regular (when the surface was smooth and regular in the 3D angiography) and irregular (in case of blebs or multilobular shape).
WEB shape change (also called “compaction”) was defined as a decrease in the height of the device or a deepening of the proximal and distal concave recesses during follow-up:8 It was analyzed on nonsubtracted images. Methods to evaluate WEB changes are reported in the On-line Appendix.
Statistical Analysis
Categoric data were described by frequency, whereas quantitative data, by means and SDs. We assessed the following: 1) long-term angiographic aneurysm occlusion (“adequate occlusion” [RR 1/RR 2] versus “incomplete occlusion”[RR 3]); and 2) WEB shape modification (yes versus no) during midterm follow-up. A χ2 test was used to evaluate qualitative factors: vascular risk factors, location, ruptured status, bifurcation point versus sidewall, aneurysm shape, wide ostium (≥4 versus <4 mm), vessel coming from the aneurysm, additional stent placement, WEB shape modification, immediate aneurysm occlusion, and correctly sized versus undersized devices. The t test (2-tailed) was applied to assess quantitative factors (age, aneurysm dome size, dome/ostium ratio, aspect ratio). The independent variables significantly associated (P ≤ .1 in the univariate analysis) with adequate occlusion or WEB shape modifications were analyzed together in a binary logistic regression to assess the independent contribution of each factor. The results of the regression model were calculated with the Wald test and expressed using a P value and related odds ratio. All statistical analyses, descriptive and inferential, were performed with SPSS, Version 24 (IBM, Armonk, New York).
RESULTS
Baseline Population and Aneurysm Characteristics
In the 5-year period, 130 consecutive aneurysms/patients were treated with the WEB (detailed data in On-line Table 1). We extracted 86 patients (58 women, 28 men; mean age, 61 years; range, 35–76 years) available at midterm angiographic follow-up. Twenty-one patients (24%) were treated in the setting of acute SAH. The mean aneurysm dome size was 5.5 ± 1.9 mm; range, 3–11.5 mm), and the most common location was the MCA bifurcation (43/86 = 50%), followed by the basilar tip (BT) (13/86 = 15%) and the anterior communicating artery (AcomA) (12/86 = 13.9%).
Treatment Characteristics and Technical Results
The WEB-SL was used in all cases (On-line Table 2). The WEB-SL and WEB-Single-Layer Sphere (SLS) were used in 90.6% (78/86) and 8.4% (8/86) of patients, respectively. Additional stent placement was performed in 13 cases (13/86 = 15%).
Successful WEB deployment was achieved in all cases. The mean intervention and fluoroscopy times were 66 ± 17 minutes (range, 50–103 minutes) and 30 ± 12 minutes (range, 18–60 minutes), respectively.
Angiographic Outcome of Aneurysms
The mean angiographic follow-up was 17 ± 11.5 months; range, 12–32 months) (On-line Table 2). Immediately after treatment, RR 1/RR 2 occlusion was 48.8% (42/86). At 12-month follow-up, 49/86 (57%) and 19/86 (22%) aneurysms presented with complete occlusion and ostium remnants, respectively. The proportion of RR 1 and RR 2 occlusion was close to 49% and 33% at the 24-month follow-up (60 patients available), respectively. Overall, 51/86 (59%) WEBs were defined as adequately sized, whereas 35/86 (41%) were classified as undersized devices.
WEB shape change was detected among 22% of cases (19/86): 7% (6/86), 15% (13/86), and 0% (0/60) at 6-, 12-, and 24-month follow-up, respectively. Retreatment with additional stent and coiling was required in 11/86 recanalized aneurysms (13%).
Predictors of Adequate Occlusion and WEB Shape Change
Significant predictors of occlusion and WEB shape change at univariate analysis were further analyzed in multivariable logistic regression (On-line Tables 3 and 4). Regular shape (OR = 5.9; 95% CI, 1.4–24; P = .01) was an independent predictor of good occlusion, whereas a wide ostium (OR = 0.2; 95% CI, 0.01–1; P = .04) was an independent factor in incomplete occlusion.
Irregular shape (OR = 5.4; 95% CI, 1.4–19; P = .01) and a wide ostium (OR = 9.8; 95% CI, 1.6–60; P = .03) independently influenced the likelihood of WEB shape change at follow-up. Higher aneurysm dome size (continuous variable) showed a trend toward greater WEB shape modification (OR = 1.39; 95% CI, 0.9–1.6; P = .06).
DISCUSSION
Predictors of Angiographic Occlusion
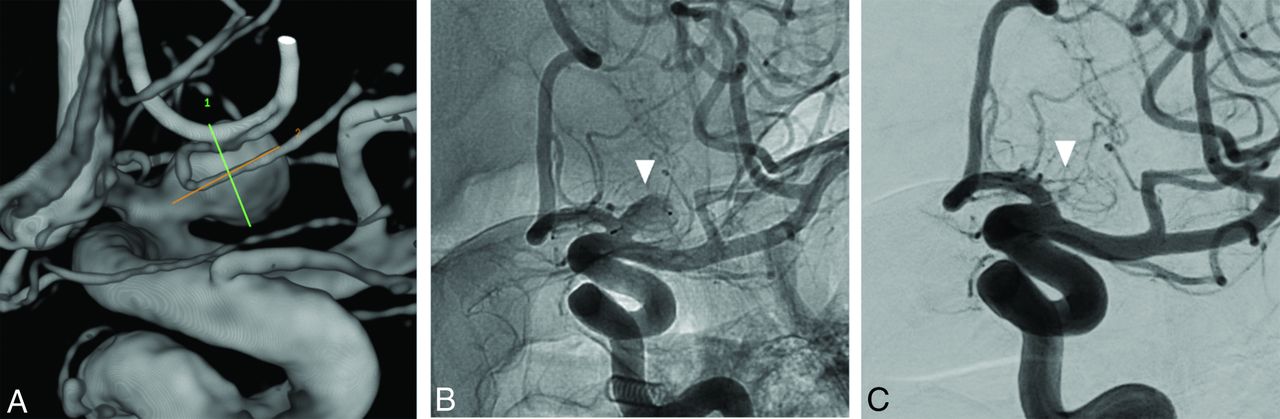
Consistent with the literature of WEB devices reporting 80% adequate occlusion at 1 year,3,9 in our series, RR 1/RR 2 occlusion was 79% and 81% after 12- and 24-month DSA follow-up. Kabbasch et al,10 evaluating a series of 98 aneurysms treated with the WEB, reported dome size, intra-aneurysmal thrombosis, and additional coiling as factors associated with lower occlusion at 6-month follow-up. Another recent series of 24 aneurysms reported that ostium size and dome-to-ostium ratio were significantly related to the angiographic results after WEB treatment.2 To our knowledge, there are no studies investigating independent predictors of occlusion after treatment with WEB devices. In our series of 86 patients, eliminating the influence of potential confounders using the regression model showed that ostium diameter and aneurysm shape were the only independent predictors of occlusion. Among the subgroup of adequately occluded aneurysms, 60% had a diameter of the ostium <4 mm (Fig 1), whereas 40% had a diameter of the ostium ≥4 mm. In addition, wide-ostium lesions represented 91% of the incompletely occluded aneurysms (Fig 2). Therefore, the binary logistic regression revealed that a wide ostium indicated 80% reduction in the probability of achieving long-term good occlusion after WEB treatment (OR = 0.2; 95% CI, 0.01–1; P = .04).
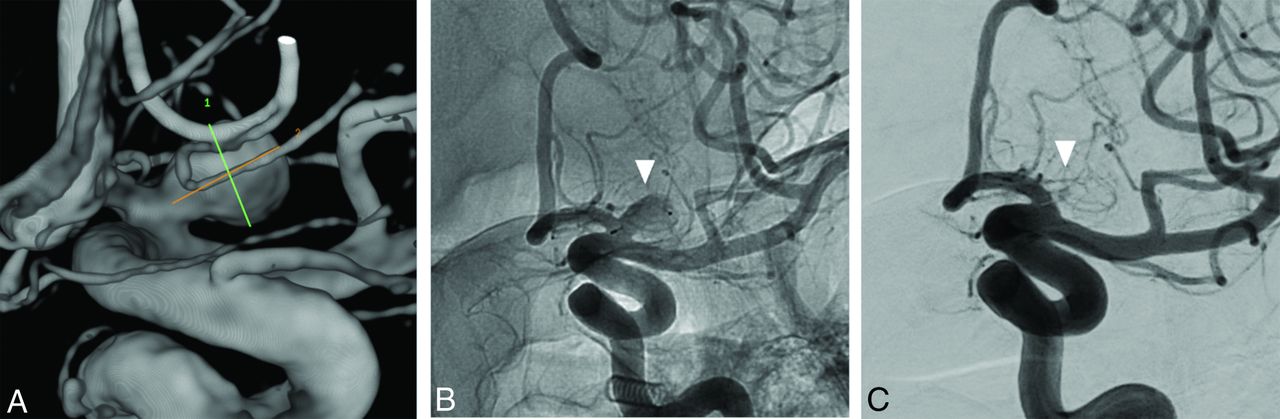
A, Left ICA angiography depicting an unruptured saccular aneurysm with regular morphology originating from the proximal A1 segment. The aneurysm dome, height, and ostium diameters were 6, 7, and 3 mm (small ostium), respectively. Accordingly, this aneurysm had all the predicting factors of adequate occlusion. B, A WEB-SLS (7 mm) was opened inside the sac, with a good aneurysm wall apposition (white arrowhead). C, Twelve-month DSA follow-up shows complete occlusion of the aneurysm (white arrowhead).

A, Right ICA angiography showing an irregular 9 (dome) × 5 mm (height) MCA unruptured aneurysm (white arrowhead) with a wide ostium (6 mm) (B). C, A WEB-SL (10 × 5) was delivered inside the sac (black arrowhead). Subsequently, in the same treatment session, a Neuroform Atlas (Stryker Neurovascular, Kalamazoo, Michigan) 3 × 20 (red arrow) was implanted from the M1 to the M2 (superior division branch) due to a small WEB protrusion into the vessel. D, Twelve-month DSA follow-up shows aneurysm recanalization (white arrowhead). This aneurysm presented with all the risk factors (wide ostium and irregular shape) for incomplete occlusion. E, Flat panel CT reconstruction depicts WEB shape modification (compaction) and the deployment of a second Neuroform Atlas 3 × 20 with a jailed microcatheter inside the sac. F, The residual aneurysm was completely occluded after Y-stent placement assisted coiling.
Lower occlusion rates among lesions with a wide ostium are likely related to the following reasons: 1) Ostium coverage might be more difficult among large-ostium lesions; and 2) the higher hemodynamic impact of blood flow may decrease the intrasaccular thrombosis or may promote WEB displacement toward the aneurysm fundus. Hemodynamic studies showed that intra-aneurysmal blood flow was faster when the aneurysm neck was wider.11 The presence of a wide neck has been previously reported as a factor associated with lower occlusion rates after coiling.12 Accordingly, higher intra-aneurysmal blood flow among lesions with a wide ostium may contribute, at least in theory, to the lower occlusion rate after WEB treatment. When one investigates the literature about other treatment options, a wide ostium appears significantly associated with aneurysm recanalization after coiling,13 whereas aneurysm size and incorporation of a branch vessel predicted persistence after flow diversion.14 Most interesting, in our analysis, aneurysm size and vessels coming from the aneurysm were not predictors of recanalization after WEB treatment. It is likely that size did not influence the angiographic occlusion due to the relatively small range of aneurysm dome size in our study (from 3 to 11 mm). Conversely, Bender et al14 reported a larger size as a predictor of lower occlusion after flow diversion, including a larger range of aneurysm diameters (from 1 to 31 mm). Finally, the distal hemodynamic demand through the branching vessel will likely maintain the flow across the ostium, lowering the occlusion in case of flow-diverter devices, but not impacting intrasaccular thrombosis after WEB implantation.
The second independent predictor of occlusion was aneurysm shape: Aneurysms with regular morphology were 6 times more likely to be occluded at 12-month follow-up (Fig 1), compared with lesions presenting with an irregular sac (OR = 5.9; 95% CI, 1.4%–24%; P = .01) (Fig 2). Our study is the first highlighting shape as prognosticator of occlusion after the WEB treatment. In our experience, among irregular lesions, the more difficult selection of the appropriate WEB dimension, together with the incomplete apposition of the device on the aneurysm wall and ostium, may decrease the likelihood of good occlusion.
Although undersized WEBs were more represented among the group of incompletely occluded aneurysms (58% versus 34%), adequate sizing and undersizing were not significant predictors of the angiographic outcome. However, most of the WEBs were just slightly undersized, often in case of branching vessels coming from the aneurysm. Accordingly, the impact of this factor can be underestimated in our series. However, other authors also found similar results: Herbreteau et al,15 in a prospective series of 39 aneurysms treated with WEB, reported statistically comparable rates of complete occlusion among undersized and appropriately sized WEB devices.
Another important point was that WEB shape change, though higher among the incompletely occluded aneurysms (50% versus 17.5%), was not an independent prognosticator of occlusion in the multivariate model (Fig 3). As discussed in the following paragraph, these data corroborate the theory that WEB shape modifications (sometimes called “WEB compaction”) are more of an epiphenomenon of the aneurysm thrombosis process rather than a reflection of the treatment failure.

A, Right MCA saccular and unruptured aneurysm (dome size, 8 mm; ostium size, 5.5 mm; height, 7 mm). B, The aneurysm was treated with a WEB-SL 9 × 5, and the flat panel CT reconstruction showed the correct WEB deployment inside the sac. C, The WEB presented with an evident reduction of the height at the 14-month DSA angiography follow-up (red arrow). D, However, despite the evident WEB shape modification, the aneurysm was still adequately occluded, having a residual ostium (red arrowhead).
Finally, consistent with recent publications,16 the use of the WEB with stent placement was feasible and effective, but additional devices did not significantly influence the final occlusion rate: Ruptured and unruptured lesions presented comparable rates of good angiographic results.
Predictors of WEB Shape Modification
WEB shape modification has been called, in some reports, “compression” or “compaction,” and it is relative to the reduction of the height of the WEB on the angiographic follow-up.4 This feature has been reported in up to 65% of patients, and whether WEB compaction is directly associated with aneurysm recanalization is still debated.1,2 Recent series reported similar rates of adequate occlusion, among the group of lesions both with and without WEB modifications.2,4 Herbreteau et al15 reported WEB shape modification among 31% of aneurysms, stressing the absence of a relationship between the sizing of the device and its height reduction. The WEB shape change was associated with an increase of the ostium remnants, without impacting the overall rate of adequate occlusion. Our results were in accordance with this study, showing no statistically significant correlation between sizing and the risk of WEB shape modification at follow-up. Most interesting, aneurysm shape and ostium dimensions were significant predictors of WEB compaction. Irregular aneurysms were 63% and 28% among the group of lesions with and without WEB shape modification, respectively, increasing the probability of this phenomenon at follow-up (OR = 5.4; 95% CI, 1.4–19; P = .01) (On-line Table 4) >5 times, while the presence of a wide ostium increased the likelihood of compaction (OR = 8; 95% CI, 1.6–60; P = .03) by 10 times.
However, this phenomenon is still a matter of debate. First, as reported in the article of Cognard and Januel,17 and in the response to this article by Pierot,8 the term “compression” is probably not appropriate because it indicates only a “water-hammer” mechanism that is not yet demonstrated. Pierot et al3 suggested that clot organization and retraction may contribute to both the intrasaccular occlusion and the shrinkage of the WEB. This effect has also been described in experimental models of coiled aneurysms, which observed that fibrosis increased coil retraction and compaction.18 However, we still do not have a full explanation for this event, and mechanisms underlying WEB compaction are probably multifactorial. In our series, we demonstrated that WEB shape modifications were not associated with lower aneurysm occlusion, supporting the theory of a retraction of the marker recesses related to thrombus evolution/fibrosis.
Reasons behind the association between irregular shape and WEB shape change are difficult to explain, and it has never been investigated before. Cognard and Januel,17 having reported this phenomenon for the first time, stressed that a large ostium and irregular shape were likely the main reasons for aneurysm remnants and cage compaction in their series. The authors questioned whether the cage must occupy the entire volume to obtain complete and stable occlusion, minimizing the risk of cage modifications by clot formation or cage displacement.19
Finally, as we previously reported, WEB shape modification was unlikely to be observed among small-ostium lesions (<4 mm), while a wide ostium was independently associated with this phenomenon. Accordingly, hemodynamic factors related to a larger diameter of the ostium may at least participate in the complex mechanism leading the decrease of the height of the device.20
Limitations of the Study
Our study has limitations intrinsic to single-center series. The data were analyzed retrospectively, and the number of patients was relatively small. The WEB shape modification was not quantitatively evaluated. Finally, due to the relatively small number of patients, some variables may not reach statistical significance in the multivariate analysis.
CONCLUSIONS
In our study, approximately 80% of aneurysms were adequately occluded after WEB implantation, whereas nearly 20% of the devices showed shape modification at follow-up. The likelihood of good occlusion was 5 times less in the presence of a wide ostium, whereas aneurysms with regular morphology were about 6 times more likely to be occluded. WEB shape change, though more prevalent among incompletely occluded lesions, was not independently associated with angiographic occlusion, and it was strongly dependent on aneurysm shape and ostium size.
Footnotes
Disclosures: Pierre-Henri Lefevre—UNRELATED: Payment for Development of Educational Presentations: Medtronic. Alain Bonafe—UNRELATED: Consultancy: Medtronic, Stryker, MicroVention.* Vincent Costalat—UNRELATED: Consultancy: Balt, Medtronic, MicroVention, Balt Stryker, Cerenovus; Grants/Grants Pending: Stryker, Medtronic; Payment for Development of Educational Presentations: Stryker, Medtronic. *Money paid to institution.
References
- Received June 10, 2019.
- Accepted after revision August 5, 2019.
- © 2019 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Neck apposition is a key factor for aneurysm occlusion after Woven EndoBridge device embolization
- Woven EndoBridge device apposition and compression using Sim&Size virtual simulation correlate with aneurysm occlusion status: a retrospective cohort study
- Use of the Woven EndoBridge Device for Sidewall Aneurysms: Systematic Review and Meta-analysis
- Impact of A1 Asymmetry on the Woven EndoBridge Device in Anterior Communicating Artery Aneurysms
- Shape Modification is Common in Woven EndoBridge-Treated Intracranial Aneurysms: A Longitudinal Quantitative Analysis Study
- Residual Flow Inside the Woven EndoBridge Device at Follow-Up: Potential Predictors of the Bicetre Occlusion Scale Score 1 Phenomenon
- Advances in endovascular aneurysm management: flow modulation techniques with braided mesh devices