
Abstract
SUMMARY: The poorly understood mechanisms of aneurysm healing contribute substantially to the pressing medical problem of coiled aneurysm recanalization. Using an established saccular aneurysm model, we developed an animal model system in rabbits to study aneurysm and skin wound healing concurrently in the same animal. We found treated aneurysm healing to be similar to skin wound healing both histologically and in biomarker gene and protein expression, but in a delayed fashion.
ABBREVIATIONS:
- GAPDH
- glyceraldehyde phosphate dehydrogenase
- H&E
- hematoxylin-eosin
- SMA1
- α smooth muscle actin
- TGFβ1
- transforming growth factor β 1
- PDGF
- platelet derived growth factor
- VEGF
- vascular endothelial growth factor
Despite wide use and considerable safety of endovascular coiling of intracranial aneurysms, the recurrence rate is high even with second-generation coils,1 partially due to a dearth of knowledge about healing mechanisms involved.2 Conversely, cutaneous wound healing is well-established. The 4 distinct-yet-overlapping stages of cutaneous wound healing (hemostasis, inflammation, proliferation, and remodeling) have been thoroughly described.3 Here we demonstrate that concurrent study, in the same research subjects, of endovascular-versus-cutaneous healing provides insight into deficiencies in the cellular, molecular, and humoral features in aneurysm healing, enabling elucidation of potential targets for improved outcomes.
Materials and Methods
Aneurysm Creation and Coil Embolization
All procedures were approved by the Institutional Animal Care and Use Committee before study initiation. Elastase-induced saccular aneurysms were created at the origin of the right common carotid artery in 12 female New Zealand white rabbits.4 At least 3 weeks later, aneurysms were treated with platinum coils. DSA was performed after embolization.
Cutaneous Ear Wound Creation
Immediately after aneurysm treatment, an ear skin defect was created on the ventral side of 1 ear using a 1-cm stainless steel punch,5 with removal of skin down to the cartilage. Hemostasis was achieved with pressure, followed by occlusive dressing (TegaDerm; 3M, St. Paul, Minnesota). Ear wounds were assessed visually daily for healing and wound closure rate.
Follow-Up Imaging and Tissue Harvest
At days 1, 5, 14, and 30 (groups 1–4) following treatment, DSA was performed from a left femoral approach, and the animals were euthanized. The aneurysm, ear wound, and contralateral control tissues were harvested for histology or cut in 2 for biomolecular studies.
Angiographic Analysis
Aneurysm occlusions at follow-up were rated either stable or progressive, or recanalizated compared with posttreatment angiograms using the modified Raymond scale.6
Histologic Analysis
Formalin-fixed aneurysms were evaluated for the degree of neck tissue coverage.7 Following a modified histologic technique, aneurysms and ear wounds were sectioned and stained with hematoxylin-eosin (H&E) or Masson Trichrome for collagen. A semiquantitative scoring for thrombus organization, neoepithelialization, inflammation, cellularity, and collagen deposition was performed by a blinded reviewer. In addition, an ordinal grading system was used to evaluate histologic healing of aneurysms between groups.
RNA Extraction and Expression Analysis by Real-Time Polymerase Chain Reaction
Total RNA was isolated and converted to complementary DNA followed by real-time polymerase chain reaction with SYBR greenER (www.thermofisher.com). Target gene expression (Table) was normalized to glyceraldehyde phosphate dehydrogenase (GAPDH) and reported as a fold change relative to control tissues (contralateral tissues) using the 2-ΔΔCt method.
Genes important in cutaneous wound healing
Protein Extraction and Analysis by Sodium Dodecyl Sulfate Polyacrylamide Gel Electrophoresis and Western Blot
Soluble proteins were extracted from tissue samples with RIPA buffer (https://www.thermofisher.com/order/catalog/product/89900). Protein separation and western analysis were performed using a Wes system (ProteinSimple, San Jose, California). Protein expression data were normalized to control proteins (GAPDH or β-actin) using Compass Software (http://www.compass-software.de/en-us) and reported as fold change relative to control tissues.
Statistical Analysis
Continuous variables were compared using a Student t test, and categoric variables were compared using the Fisher exact test.
Results
Aneurysm Angiography
Among the first 3 groups, mean aneurysm neck, width, and height were 3.3 ± 1.8 mm, 4.0 ± 1.8 mm, and 9.8 ± 1.6 mm, respectively. The aneurysms were completely occluded immediately after coil embolization in 11 of 12 cases (92%), the other being incompletely occluded (8%). Two of the 3 aneurysms in the 24-hour group, and 1 in the 14-day group showed recanalization at sacrifice. All the other aneurysms (9 of 12) remained completely occluded (75%) (Fig 1).

Angiograms with H&E-stained tissue sections. Elastase-induced aneurysm (A) on the day of platinum coil embolization and ear wound creation. Angiogram of coiled aneurysm at 14 days (B) with a corresponding ear wound (C, H&E, magnification ×100), macro image of the ear wound on day of sacrifice (D, ruler markings are in centimeters, the smallest ticks in millimeters). Angiogram of 30-day coiled aneurysm (E) with corresponding aneurysm (F, H&E, magnification ×200). Note diffuse, dense myofibroblast (long, spindle-shaped) proliferation in both H&E photomicrographs.
Histology
Histologic analysis revealed necrosis and inflammatory cell infiltration in both epidermal and dermal layers of ear wounds at both 24 hours and 5 days, whereas scab formation in the epidermis and diffuse, dense cellular proliferation of myofibroblasts within the dermal layer with minimal inflammatory cells was found by 14 days. Aneurysm features were consistent with previous findings,8 with sparse myofibroblasts at the periphery of the aneurysm dome by 14 days, increasing dramatically by 30 days (Fig 1D, -F).
Biomolecules
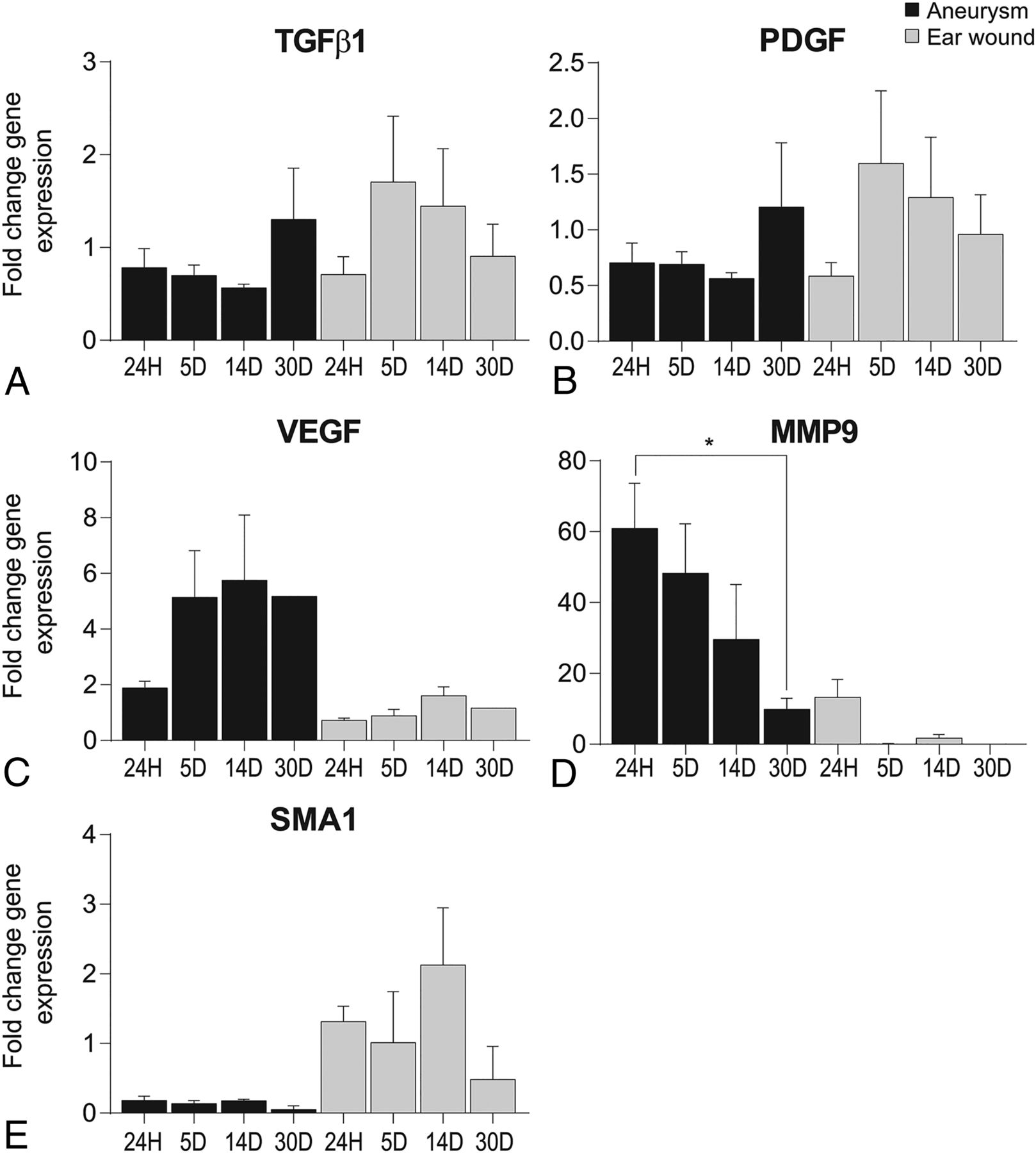
Inflammatory marker gene expression was elevated at 5 days in ear wounds but reduced/delayed until 30 days in aneurysms (Fig 2A, -B). Protein expression, however, was only 2-fold for transforming growth factor β1 (TGFβ1) at 24 hours and 30 days in ear wounds (data not shown). Proliferation marker expressions in aneurysms were higher compared with ear wounds (Fig 2C, -D) and with inflammatory markers, overall. α smooth-muscle actin (SMA1) remodeling markerexpressions were relatively unremarkable, with a small increase at 14 days in ear wounds (Fig 2E). Macrophage analysis showed an overall M1 polarization, with peak CD86 levels at 24 hours in aneurysms and 5 days in ear wounds (data not shown).
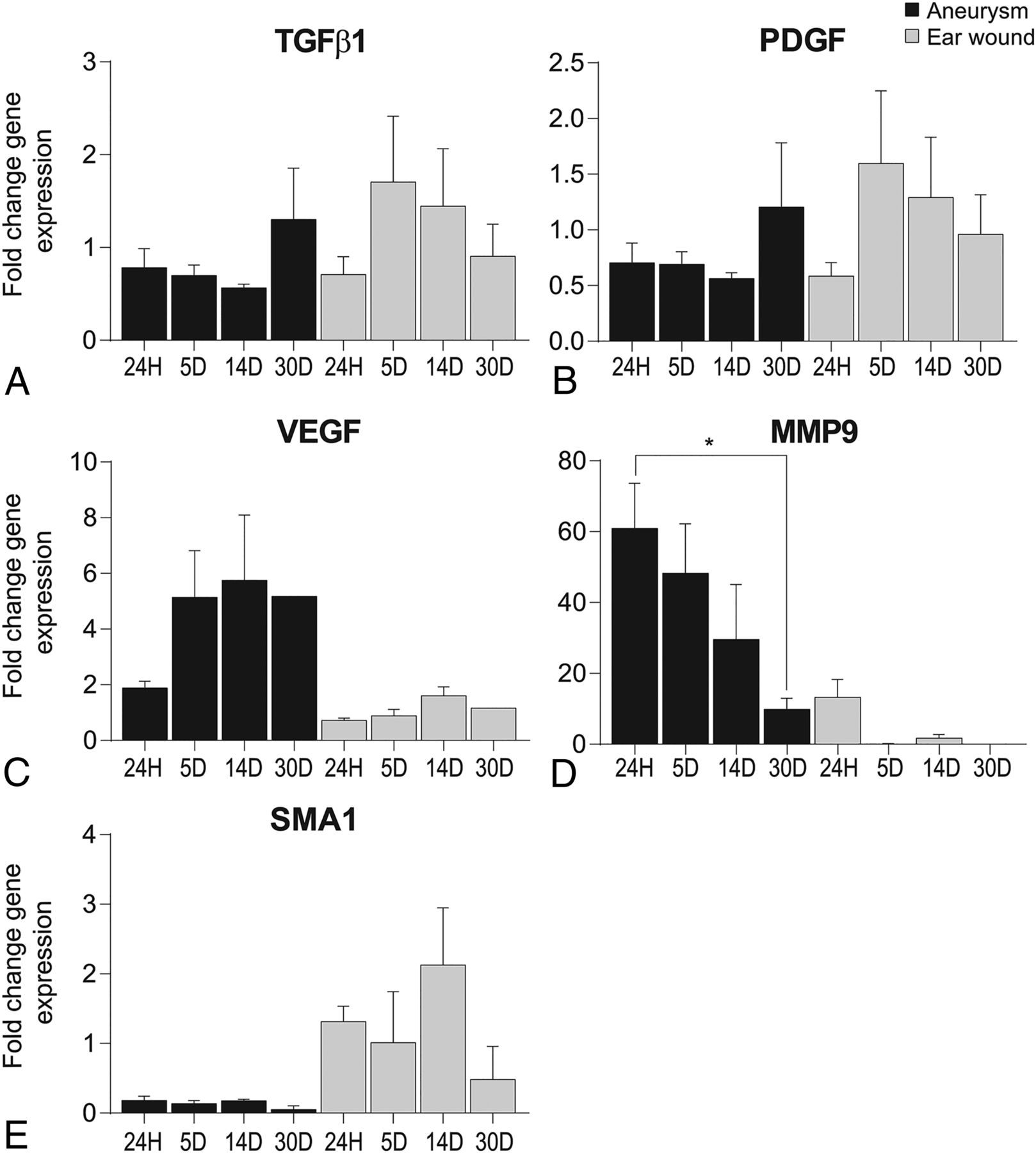
Gene expression data from aneurysms and cutaneous ear wounds after 24 hours (24H), 5 days (5D), and 14 days (14D). Data were normalized to GAPDH and displayed as a fold change relative to normal tissues (left carotid artery or contralateral ear, respectively) from the same animal (P = .0422 in D) (n = 3 animals, 3 experimental replicates). PDGF indicates platelet-derived growth factor; VEGF, vascular endothelial growth factor; MMP9, matrix metalloproteinase 9; 30D, 30 days.
Discussion
Our results reveal similarities and differences in wound-healing mechanisms for these 2 disparate environments. Histologically, skin wounds at 2 weeks resemble aneurysms at 1 month following platinum coil treatment,8 suggesting a roughly 2-week healing delay in coiled aneurysms relative to skin wounds. Previous studies8 showed similar findings, supporting this issue of deficient immune cell infiltration and immune-driven healing mechanisms in platinum-coiled aneurysms.2 The biomolecular profiles reflect this healing delay and confirm an M1 polarization in the macrophage profile, indicating a deficient prohealing phenotype.9
Conclusions
This novel animal model enabling longitudinal study of platinum-coiled aneurysm healing in parallel with cutaneous wound healing provides an exceptional level of control and will help determine key signaling events necessary for proper arterial wound healing, promising development of improved treatments.
Acknowledgments
We thank Chunfeng Zhao, MD, Praveen Kolumam Parameswaran, and Daiying Dai for essential work done for this article.
Footnotes
Disclosures: David F. Kallmes—UNRELATED: Stock/Stock Options: Superior Medical Experts, Comments: founder/shareholder. Ram Kadirvel—RELATED: Grant: National Institutes of Health, Comments: grant No. NS076491.* *Money paid to the institution.
This work was supported by Mayo Clinic Radiology Research and R01 grant number NS076491.
Indicates open access to non-subscribers at www.ajnr.org
REFERENCES
- Received March 13, 2019.
- Accepted after revision March 19, 2019.
- © 2019 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.