
Abstract
BACKGROUND AND PURPOSE: A few patterns of orbital fat prolapse have been described. Some are associated with disease, and others may mimic a neoplasm. We have observed prolapse of orbital fat into the infratemporal fossa via the inferior orbital fissure on MR imaging. The clinical relevance of this finding, if any, is unknown. The purposes of this study were to describe the MR imaging appearance of orbital fat prolapse through the inferior orbital fissure, to estimate the prevalence of this finding, and to assess possible pathologic associations.
MATERIALS AND METHODS: For this retrospective study of 228 orbital MR imaging examinations, 3 neuroradiologists independently assessed the presence of prolapse on high-resolution T1-weighted images. Discrepancies were resolved by consensus, and interobserver agreement was calculated. Patient demographics, indications for imaging, and pertinent clinical history were recorded. One-way analysis of variance and the Fisher exact test were used to assess possible associations between prolapse and specific patient characteristics.
RESULTS: Orbital fat prolapse through the inferior orbital fissure was observed in 20/228 patients (9%). This finding was unilateral in 11 patients (55%) and bilateral in 9 patients (45%). There was no significant association with age, sex, obesity, Graves disease, hypercortisolism, prior orbital trauma, proptosis, or enophthalmos. Interobserver agreement was 90%.
CONCLUSIONS: Prolapse of orbital fat into the infratemporal fossa via the inferior orbital fissure is a relatively common finding on orbital MR imaging that has no identified pathologic association. Neuroradiologists should recognize this finding so as not to report it as pathologic.
Several patterns of orbital fat prolapse have been previously described,1⇓⇓–4 some of which are clinically relevant. Intracranial fat prolapse has been associated with optic nerve compression in thyroid eye disease.1 Subconjunctival fat prolapse can mimic a neoplasm2; conversely, orbital lymphoma may mimic subconjunctival fat prolapse.5 Also, some data suggest an association between subconjunctival fat prolapse and thyroid eye disease.6 Not infrequently, orbital fat prolapse may be posttraumatic.3,4 Orbital fat prolapse may but does not necessarily occur in the setting of proptosis. In a small study of patients with proptosis with excess orbital fat,7 obesity, Graves disease, and Cushing syndrome were found to represent the underlying disease processes.
We have observed prolapse of the orbital fat into the infratemporal fossa via the inferior orbital fissure on MR imaging. The prevalence of this finding and the clinical relevance, if any, are unknown. We hypothesized that this finding falls within the range of normal anatomic variations and is not associated with orbital disorders or systemic diseases with orbital manifestations.
The purposes of this study were to describe the MR imaging appearance of orbital fat prolapse through the inferior orbital fissure, to estimate the prevalence of this finding, and to test our hypothesis that this finding represents a normal variant by assessing possible pathologic associations with aging, obesity, Graves disease, hypercortisolism (eg, Cushing disease, exogenous steroids), prior orbital trauma, proptosis, and enophthalmos.
Materials and Methods
Subjects
For this retrospective, Health Insurance Portability and Accountability Act–compliant, institutional review board–approved study, all orbital MR imaging examinations performed at Massachusetts Eye and Ear between January 1, 2017, and August 1, 2017, were reviewed (n = 324) by 3 neuroradiologists. Inclusion criteria were the following: 1) a high-resolution axial T1-weighted sequence through the orbits without gadolinium contrast, and 2) no prior orbital operation. Examinations were excluded if an orbital MR imaging examination had already been included in the study cohort for the same patient or the diagnostic assessment was precluded by severe motion artifacts or other artifact degradation. A total of 228 orbital MR imaging examinations satisfied these criteria and formed the study cohort.
Medical Record Review
Basic patient characteristics including age, sex, and body mass index were recorded. Pertinent medical history was also recorded, including a history of orbital trauma and endocrinopathies, including Graves disease and Cushing syndrome. A targeted review of patient medications was also performed, including the use of oral steroid medications.
Image Acquisition
All orbital MR imaging examinations were performed on a 3T scanner (Achieva; Philips Healthcare, Best, the Netherlands) using an 8-channel head coil (SENSE Flex M coil; Philips Healthcare). Although there was some variability in the individual sequences included in each orbital MR imaging examination related to the retrospective nature of this study, the typical examination included sagittal T1, axial DWI, axial T2, and axial T1 gadolinium-enhanced images of the brain as well as high-resolution axial T1, coronal T1, coronal STIR, and coronal fat-suppressed T1 gadolinium-enhanced images of the orbits. For high-resolution sequences, the slice thickness was 3-mm and the acquisition matrix ranged from 300 × 300 to 415 × 415.
Reader Assessment
After a training session based on 10 orbital MR imaging examinations that were not included in this study cohort, 3 fellowship-trained neuroradiologists (8, 3, and 2 years' subspecialty expertise) independently reviewed the high-resolution axial T1-weighted images from the 228 included orbital MR imaging examinations using the PACS of our institution. When present, the high-resolution coronal T1-weighted images were also reviewed.
Each neuroradiologist recorded the presence or absence of orbital fat prolapse for each eye in all patients. The recorded results were compared, and discrepancies were resolved by a consensus review.
Prolapse was defined as present when a discrete, rounded focus of fat signal intensity could be identified as both distinguishable from the normal infratemporal fossa fat and contiguous with the normal orbital fat via the inferior orbital fissure (Fig 1). When prolapse was present, 1 fellowship-trained neuroradiologist performed a long-axis measurement of the prolapsed fat on high-resolution T1 images. The same neuroradiologist also evaluated the prolapsed fat for associated septa on T1-weighted images, fluid signal on STIR images, and enhancement on gadolinium-enhanced T1-weighted images with fat suppression (Fig 2). Additionally, a different neuroradiologist measured the perpendicular distance from the anterior margin of each globe to the interzygomatic line with the upper limit of normal defined as 21 mm7 and the lower limit of normal defined as 12 mm.8

Axial (A) and coronal (B) T1-weighted images demonstrate prolapse of the left orbital fat (white arrows) into the left infratemporal fossa via the left inferior orbital fissure.
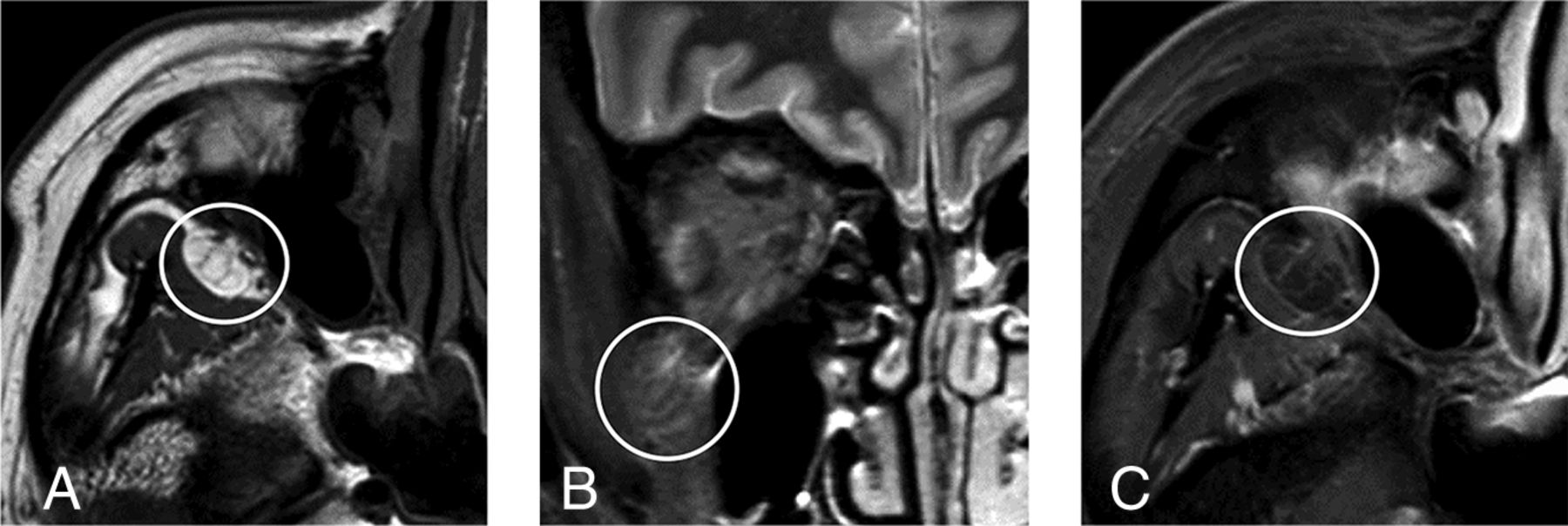
Axial T1-weighted image (A) demonstrates septa within the prolapsed orbital fat (circle). Coronal STIR image (B) demonstrates faintly increased fluid signal associated with the prolapsed orbital fat (circle). Axial gadolinium-enhanced T1-weighted image with fat suppression (C) demonstrates faint enhancement associated with the prolapsed orbital fat (circle).
Statistical Analysis
Absolute and relative frequencies are reported for categoric variables and interobserver agreement. The Fisher exact test was used to compare proportions, and 1-way analysis of variance was used to compare continuous variables. The Light κ coefficient was calculated to assess interrater reliability. All analyses were performed with JMP, Version 14 (SAS Institute, Cary, North Carolina), and a P value < .05 indicated a statistically significant difference.
Results
Subjects
A total of 324 orbital MR imaging examinations were reviewed with 72 examinations excluded for lack of a high-resolution axial T1-weighted sequence through the orbits without gadolinium contrast, 22 examinations excluded because of a prior orbital operation, and 2 examinations excluded because an orbital MR imaging examination from the same patient was already included in the study cohort. This yielded 228 patients who met the inclusion criteria of this study.
Patient age, sex, body mass index, Graves disease, hypercortisolism, prior orbital trauma, globe position, and study indication data are provided in the Table.
Characteristics of the study groupa
Reader Assessment
Interobserver agreement was 90.4% among the 3 readers for the presence or absence of orbital fat prolapse (206 patients without discrepancy, 22 patients with discrepancy). The Light κ coefficient was 0.65, indicating “good” agreement.
Prolapse of orbital fat into the infratemporal fossa via the inferior orbital fissure was observed in 20 patients (9%) ranging in age from 25 to 79 years. This finding was unilateral in 11 patients (55%) and bilateral in 9 patients (45%). The measured long axis of prolapsed fat ranged from 2 to 14 mm (mean, 7 ± 3 mm).
Among instances of prolapsed orbital fat, associated septa were present in 69%, faintly increased fluid signal was present in 26%, and faint enhancement was seen in 8%. There was no statistically significant association between orbital fat prolapse and age (P = .44), sex (P = 1.00), obesity (P = .52), Graves disease (P = 1.00), hypercortisolism (P = .07), prior orbital trauma (P = 1.00), proptosis (P = .61 for both right and left globes), or enophthalmos (P = .26 for the right globe, P = 1.00 for the left globe).
Discussion
Radiologists' responsibilities include confidently differentiating normal anatomy and normal variants from disease. Although the distinction between normal anatomy and pathology is often relatively straightforward, determining that a finding represents a normal variant rather than disease can be more problematic. Misdiagnosis of normal variation as pathology can lead to unnecessary additional tests and subject the patient to potentially harmful procedures. Accordingly, textbooks9,10 and articles11⇓⇓⇓–15 have been devoted to normal variants that may simulate disease. However, not infrequently, the evidence underlying the supposition that a particular finding represents a normal variant rather than pathology is anecdotal or, in some cases, altogether lacking. Because differentiating normal variants from disease is central to the work of the radiologist, we believe an evidence-based approach is worthwhile.
Numerous patterns of orbital fat prolapse have been previously described, many of which are clinically relevant. This study describes an additional pattern of orbital fat prolapse involving the inferior orbital fissure with an estimated prevalence of 9%, which is more commonly unilateral. This study provides evidence in support of our hypothesis that this finding falls within the range of normal anatomic variations and is unlikely to be of clinical significance.
It is unknown whether this pattern of prolapse results from a structural anomaly of the orbit. A recent case report16 describes herniation of buccal fat into the orbit through an abnormally enlarged inferior orbital fissure and postulates that herniation was possible because of the inferior orbital fissure configuration. It remains an open question whether prolapse of orbital fat into the infratemporal fossa via the inferior orbital fissure is associated with variations in the dimensions of the inferior orbital fissure from reported norms,17⇓–19 and this question would likely best be addressed with a future CT-based investigation.
An important limitation of this study is that a restricted number of possible pathologic associations were tested. An additional limitation is that the electronic medical record was used to determine the presence or absence of the diseases of interest. Relevant documentation could be incomplete or inaccurate, and it is also possible that relevant information was overlooked during our search. Although the literature informed the tested pathologic associations in this study, it is possible that a pathologic association that was not tested exists. Statistical testing for additional associations outside those supported by the literature could be performed but would also increase the risk of a type I error in this relatively small cohort. Future studies of larger cohorts testing additional possible associations could mitigate the theoretic risk of a true pathologic association not detected by the current study.
Conclusions
Prolapse of orbital fat into the infratemporal fossa via the inferior orbital fissure is a relatively common finding on orbital MR imaging that is likely a normal anatomic variant of no clinical significance. It is important for practicing neuroradiologists to recognize this finding so as not to mistake it for a pathologic entity, such as a mass.
Footnotes
Disclosures: Hillary R. Kelly—UNRELATED: Royalties: Elsevier, Comments: Book royalties were earned as editor of textbook on neuroradiology and head and neck radiology.
A previous and more primitive version of this work was presented as an electronic scientific poster at: Annual Meeting of the American Society of Head and Neck Radiology, September 26–30, 2018; Savannah, Georgia. This article contains additional data and analyses not included in the previous electronic scientific presentation.
REFERENCES
- Received March 20, 2019.
- Accepted after revision May 27, 2019.
- © 2019 by American Journal of Neuroradiology









{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.