
Abstract
BACKGROUND AND PURPOSE: Synthetic MR imaging enables the acquisition of phase-sensitive inversion recovery images. The aim of this study was to compare the image quality of synthetic phase-sensitive inversion recovery with that of other sequences in infants.
MATERIALS AND METHODS: Brain MR imaging with 3D T1-weighted fast-spoiled gradient recalled, synthetic T1WI, and synthetic phase-sensitive inversion recovery of 91 infants was compared. Contrast between unmyelinated WM and myelinated WM and between unmyelinated WM and cortical GM was calculated. Qualitative evaluation of image quality and myelination degree was performed. In infants with punctate white matter injuries, the number of lesions was compared.
RESULTS: The contrast between unmyelinated WM and myelinated WM was higher in synthetic phase-sensitive inversion recovery compared with fast-spoiled gradient recalled or synthetic T1WI (P < .001). Compared with synthetic T1WI, synthetic phase-sensitive inversion recovery showed higher gray-white matter differentiation (P < .001) and myelination degree in the cerebellar peduncle (P < .001). The number of detected punctate white matter injuries decreased with synthetic phase-sensitive inversion recovery compared with fast-spoiled gradient recalled sequences (1.2 ± 3.2 versus 3.4 ± 3.6, P = .001).
CONCLUSIONS: Synthetic phase-sensitive inversion recovery has the potential to improve tissue contrast and image quality in the brain MR imaging of infants. However, we have to be aware that synthetic phase-sensitive inversion recovery has limited value when assessing punctate white matter injuries compared with 3D fast-spoiled gradient recalled imaging.
ABBREVIATIONS:
- CP
- cerebellar peduncle
- FSPGR
- fast-spoiled gradient recalled
- GM-WM
- gray-white matter differentiation
- mWM
- myelinated white matter
- PSIR
- phase-sensitive inversion recovery
- uWM
- unmyelinated white matter
Numerous biologic changes occur in the brain tissue of infants. The brain continues myelination and vascularization before and after birth and eventually develops neurons and dendritic connections.1 Various imaging modalities have been used to depict this brain maturation in infants. MR imaging has been recognized as the most practical technique to do so by means of T1WI and T2WI.2,3 Several quantitative markers are widely accepted for this assessment, including T1 and T2 relaxation times4 and diffusion anisotropy.5 Yet, qualitative assessment of brain maturation is just as important as quantitative assessment in clinical practice.
One of the MR imaging sequences used for myelination assessment is phase-sensitive inversion recovery (PSIR). PSIR image reconstruction provides higher resolution by increasing gray-white matter differentiation (GM-WM) and the overall signal-to-noise ratio.6,7 In past studies, PSIR also enabled superior detection of focal lesions in adult patients with progressive multiple sclerosis or with cerebral autosomal-dominant arteriopathy with subcortical infarcts and leukoencephalopathy.8,9 In infants, another study concluded that PSIR images correlated well with the chronology of brain maturation and provided adequate information about brain injuries.1
There has been much effort to make MR imaging clinically more feasible for children and especially to resolve issues with its long acquisition time.2,10 The recently developed synthetic MR imaging is a multiparametric quantitative MR imaging that can generate multiple sequences by manipulating TR, TE, and TI.2,11 This technique has reduced scanning times in pediatric brain MR imaging.2 With synthetic MR imaging, we are able to obtain not only synthetic T1WI, T2WI, and proton-density images but also synthetic PSIR images.9
To the best of our knowledge, there has been no study conducted on synthetic PSIR in the assessment of brain maturation in infants. In previous studies, synthetic T1WI or T2WI showed lower or equivalent image quality compared with conventional T1WI or T2WI.2,10,12 However, the brain MR imaging protocol of infants frequently includes 3D-T1WI instead of 2D.13 The role of thin-slice images from 3D acquisition is important because it allows detection and quantification of WM injuries from perinatal insult, which predict the outcome in infants.14 Thus, the image quality of synthetic images and conventional 3D-T1WI needs to be compared before synthetic MR imaging can be implemented in infants. Therefore, the aim of our study was to compare tissue contrast, image quality, myelination degree, and the number of punctate white matter lesions assessed with synthetic PSIR in infants with those assessed with synthetic T1WI, conventional 3D-T1WI, and conventional T2WI.
Materials and Methods
Patients
The institutional review board of Ajou University Hospital approved this retrospective study. We reviewed the brain MR imaging of infants obtained from July 2016 to October 2017 using a 3T scanner (Discovery 750W; GE Healthcare, Milwaukee, Wisconsin). During the study period, the routine MR imaging protocols of infants included 3D-T1WI fast-spoiled gradient recalled (FSPGR) and multiparametric quantitative MR imaging, with or without the axial T2WI fast spin-echo sequence. With multiparametric quantitative MR imaging, synthetic T1WI and synthetic PSIR images were generated and automatically loaded on a PACS system. Demographic information and indications for MR imaging were collected through a review of the medical records. We also further classified a subgroup of infants with punctate white matter injuries.
Image Acquisition
The parameters for FSPGR were the following: TR = 9 ms, TE = 3 ms, slice thickness = 1 mm, NEX = 1, and FOV = 22 × 22 cm (scanning time = 3 minutes 6 seconds). Multiparametric quantitative MR imaging was performed using 4 saturation delays of 130, 500, 1370, and 2970 ms, and the TR was 4452 ms. The TR included 2 TEs of 22 and 128 ms. Each acquisition created 8 images per section (scanning time = 5 minutes). Slice thickness was 3 mm, and the FOV was 20 × 20 cm.3 For synthetic T1WI, the parameters were TR = 550 ms and TE = 10 ms. For synthetic PSIR, the parameters were TR = 6000 ms, TE = 10 ms, and TI = 500 ms. The parameters for synthetic PSIR were the default setting of the MR imaging scanner. The parameters for T2WI were the following: TR = 6000 ms, TE = 151 ms, slice thickness = 3 mm, NEX = 2, and FOV = 18 × 18 cm (scanning time = 3 minutes 18 seconds). Synthetic T1WI and PSIR were automatically generated after multiparametric quantitative MR imaging and were displayed on the PACS.
Image Analysis
For quantitative analysis, ROIs were manually drawn and the mean signal intensities of unmyelinated white matter (uWM), myelinated white matter (mWM), and cortical GM were measured on the images (Fig 1). The ROIs were drawn using PACS of our hospital. The contrast between uWM and mWM and between uWM and GM was measured using the Michelson contrast equation. In this equation, the contrast is the difference between the maximal and minimal intensities divided by the sum of the maximal and minimal intensities.2
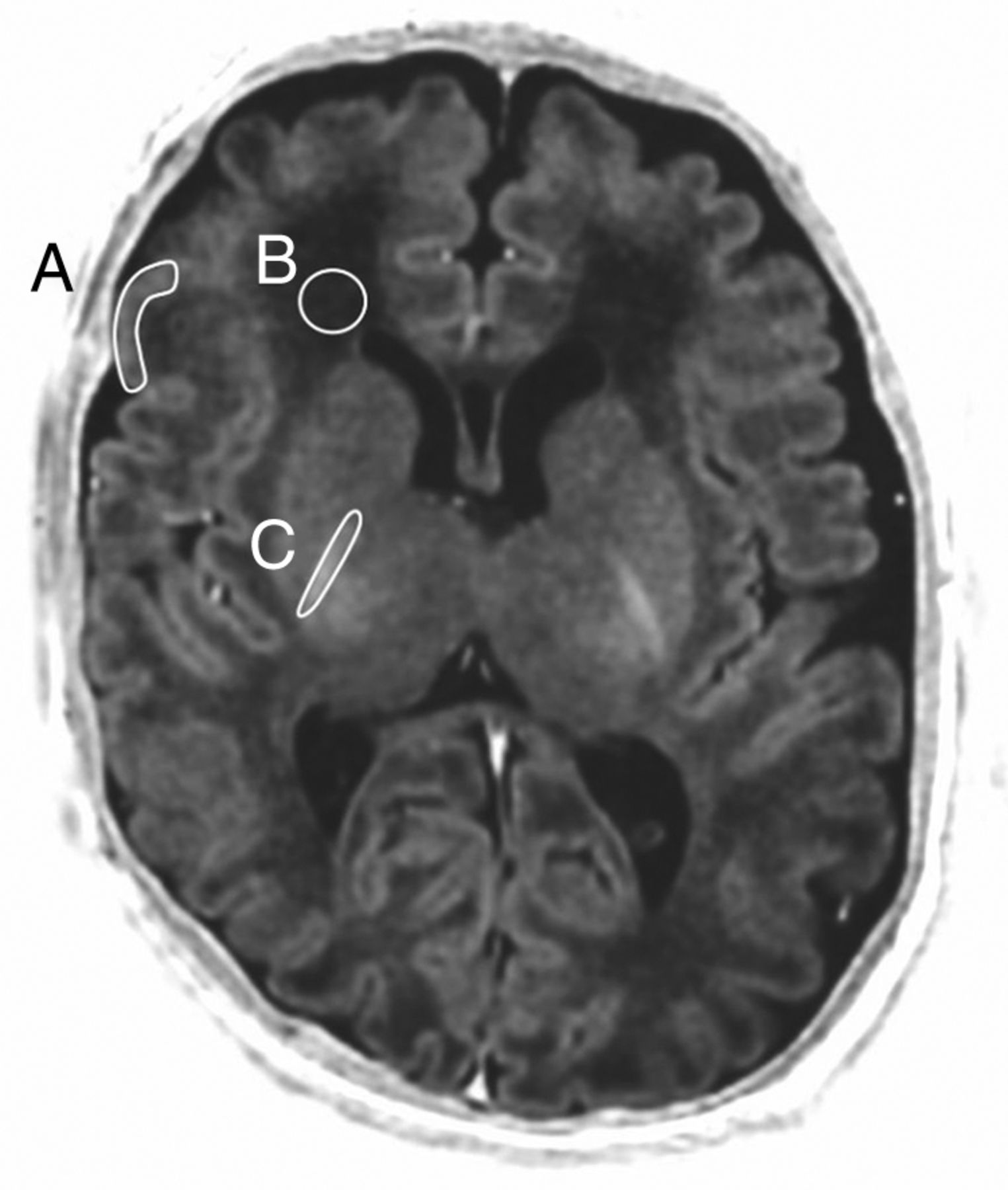
Representative synthetic PSIR image showing the drawn ROI along with cortical GM (A), uWM (B), and mWM (C).
For qualitative analysis, 2 radiologists with 8 years of experience in pediatric neuroradiology (radiologist 1) and 6 years of experience in neuroradiology (radiologist 2) performed the visual assessment. Images of 26 infants without visual abnormalities were analyzed blindly and independently in random order. The qualitative analysis was composed of 2 assessments, 1 for image quality and 1 for myelination degree. Image quality was evaluated by diagnostic quality and GM-WM. Both parameters were graded as follows: 1 = poor, 2 = moderate, and 3 = good. Myelination degree was evaluated in the cerebellar peduncle (CP), posterior limb of internal capsule, anterior limb of the internal capsule, and frontal and occipital WM. The myelination degree of each anatomic region was scored as follows: 1 = unmyelinated, 2 = intermediate, and 3 = fully myelinated.
For the subgroup with punctate white matter injuries, the injuries were shown as focal lesions with increased T1 signal intensity.15 The total number of lesions in each sequence was counted by the radiologist with 8 years of experience in pediatric neuroradiology. Then, using the coronal images of 3D-FSPGR, we measured the cranial-to-caudal diameters of lesions that were not detectable with synthetic PSIR.
Statistical Analysis
In quantitative analysis, the Friedman test was used to compare the first 3 sequences, which were FSPGR, synthetic T1WI, and synthetic PSIR. Two of the 3 sequences were compared using the Wilcoxon signed rank test, and Bonferroni correction was applied to reduce errors associated with multiple comparison. The Wilcoxon signed rank test was also used to compare tissue contrast between synthetic PSIR and T2WI. In qualitative analysis, Cochran-Mantel-Haenszel statistics were used to compare the image quality and myelination degree of the 3 sequences. To compare 2 among the 3 sequences, we performed the χ2 test after reclassifying image quality and myelination degree into 2 categories (1 or 2 versus 3). To compare the number of punctate WM lesions detected on the 3 sequences, we used the Friedman test. The mean relative comparison for synthetic PSIR versus FSPGR and synthetic PSIR versus synthetic T1WI was expressed as a percentage of FSPGR and T1WI, respectively. A positive relative comparison value means a gain in the number of lesions detected using PSIR, and a negative value indicated a loss. Statistical analyses were performed with SAS, Version 4.9 (SAS Institute, Cary, North Carolina) and R statistical and computing software, Version 3.5.0 (http://www.r-project.org/), and P values < .05 were considered statistically significant.
Results
Patient Information
A total of 91 infants (58 boys and 33 girls) were included in this study. The age range of the infants was from 1 to 180 days, and the mean corrected gestational age at MR imaging was 42.1 ± 11.1 weeks. The infants underwent brain MR imaging for various indications, with prematurity and intracranial hemorrhage being the most common. Other indications included an apnea event, seizure, suspicion of hydrocephalus, minor head trauma, and history of meningitis. The T2WI sequence was performed in 86 of 91 infants. The age range of infants with T2WI was from 1 to 175 days, and the mean corrected gestational age of these infants was 42.9 ± 10.4 weeks. There were 10 infants with punctate white matter injuries.
Contrast Comparison of the FSPGR, Synthetic T1WI, and Synthetic PSIR Sequences
Contrast observed with FSPGR, synthetic T1WI, and synthetic PSIR was compared, and the comparison results are summarized in Table 1. For the contrast between uWM and mWM, there were significant differences among the 3 sequences. When 2 of the 3 sequences were compared, PSIR (0.506) showed higher contrast compared with FSPGR (0.249, P < .001) and synthetic T1WI (0.182, P < .001). FSPGR showed significantly higher contrast compared with synthetic T1WI (P < .001). For the contrast between uWM and GM, there were also significant differences among the 3 sequences. Again, synthetic PSIR (0.393) showed the highest contrast compared with FSPGR (0.124, P < .001) and synthetic T1WI (0.099, P < .001). There was no significant difference between FSPGR and synthetic T1WI (P = .454).
Contrast comparison of the FSPGR, synthetic T1WI, and synthetic PSIR sequences (n = 91)a
Contrast Comparison between the T2WI and PSIR Sequences
Contrast observed with T2WI and synthetic PSIR was compared, and the comparison results are summarized in Table 2. Compared with T2WI, synthetic PSIR showed significantly higher contrast between uWM and mWM (0.516 versus 0.226, P < .001). For the contrast between uWM and GM, synthetic PSIR showed significantly higher contrast compared with T2WI (0.386 versus 0.176, P < .001).
Contrast comparison between the T2WI and synthetic PSIR sequences (n = 86)a
Assessment of Image Quality and Myelination Degree
The qualitative comparison of the 3 sequences is summarized in Table 3, and representative images are shown in Fig 2. For image quality, diagnostic quality and GM-WM assessed by radiologist 1 and GM-WM assessed by radiologist 2 showed significant differences among the 3 sequences. When 2 of the 3 sequences were compared by radiologist 1, synthetic PSIR showed significantly higher diagnostic quality (synthetic PSIR versus FSPGR, P = .023; synthetic PSIR versus synthetic T1WI, P = .002) and GM-WM (synthetic PSIR versus FSPGR, P = .002; synthetic PSIR versus synthetic T1WI, P < .001) compared with the other 2 sequences. When 2 of the 3 sequences were compared by radiologist 2, synthetic PSIR showed significantly higher GM-WM compared with synthetic T1WI (P < .001) but not compared with FSPGR (P > .999).
Image quality and myelination degree assessment by the 2 radiologistsa
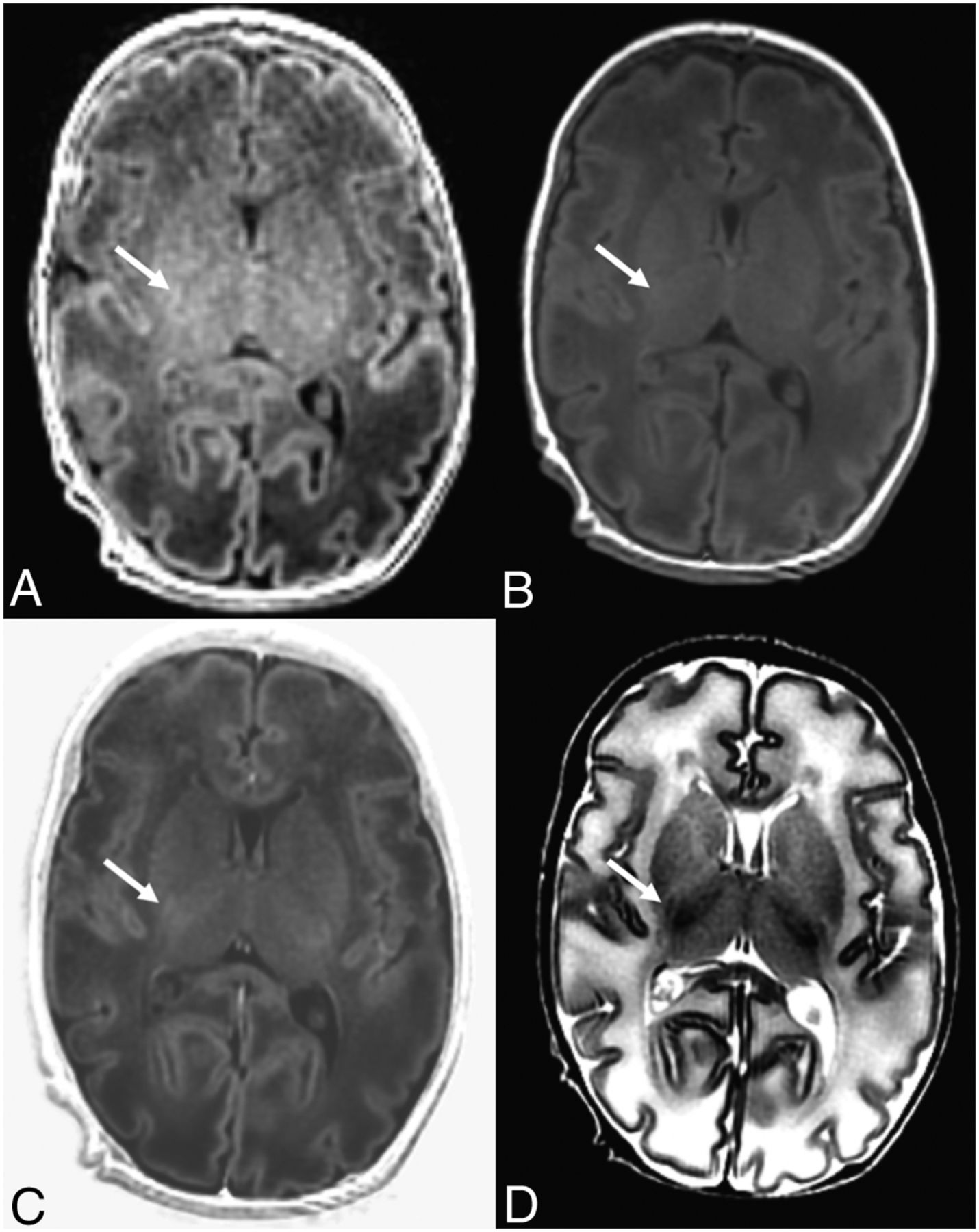
A 30-day-old neonate. There is limited myelination at the posterior limb of the internal capsule (arrow), showing higher signal intensity on the FSPGR (A), synthetic T1WI (B), and synthetic PSIR (C) images compared with the uWM regions. D, On the T2WI, the myelinated posterior limb of internal capsule (arrow) shows lower signal intensity compared with the uWM regions.
Myelination degree in the CP assessed by radiologist 1 and that in the CP and posterior limb of the internal capsule assessed by radiologist 2 showed significant differences among the 3 sequences. When 2 of the 3 sequences were compared by radiologist 1, the CP showed a significantly higher myelination degree with synthetic PSIR compared with FSPGR (P = .023) and synthetic T1WI (P < .001). When 2 of the 3 sequences were compared by radiologist 2, synthetic PSIR showed a significantly higher myelination degree in the CP compared with synthetic T1WI (P < .001), but not compared with FSPGR (P > .999). The posterior limb of the internal capsule showed significantly higher myelination degree with synthetic PSIR compared with FSPGR (P = .049) and synthetic T1WI (P < .001) by radiologist 2. Myelination degrees in other regions (anterior limb of the internal capsule, frontal WM, and occipital WM) were not significantly different.
Punctate WM Lesions
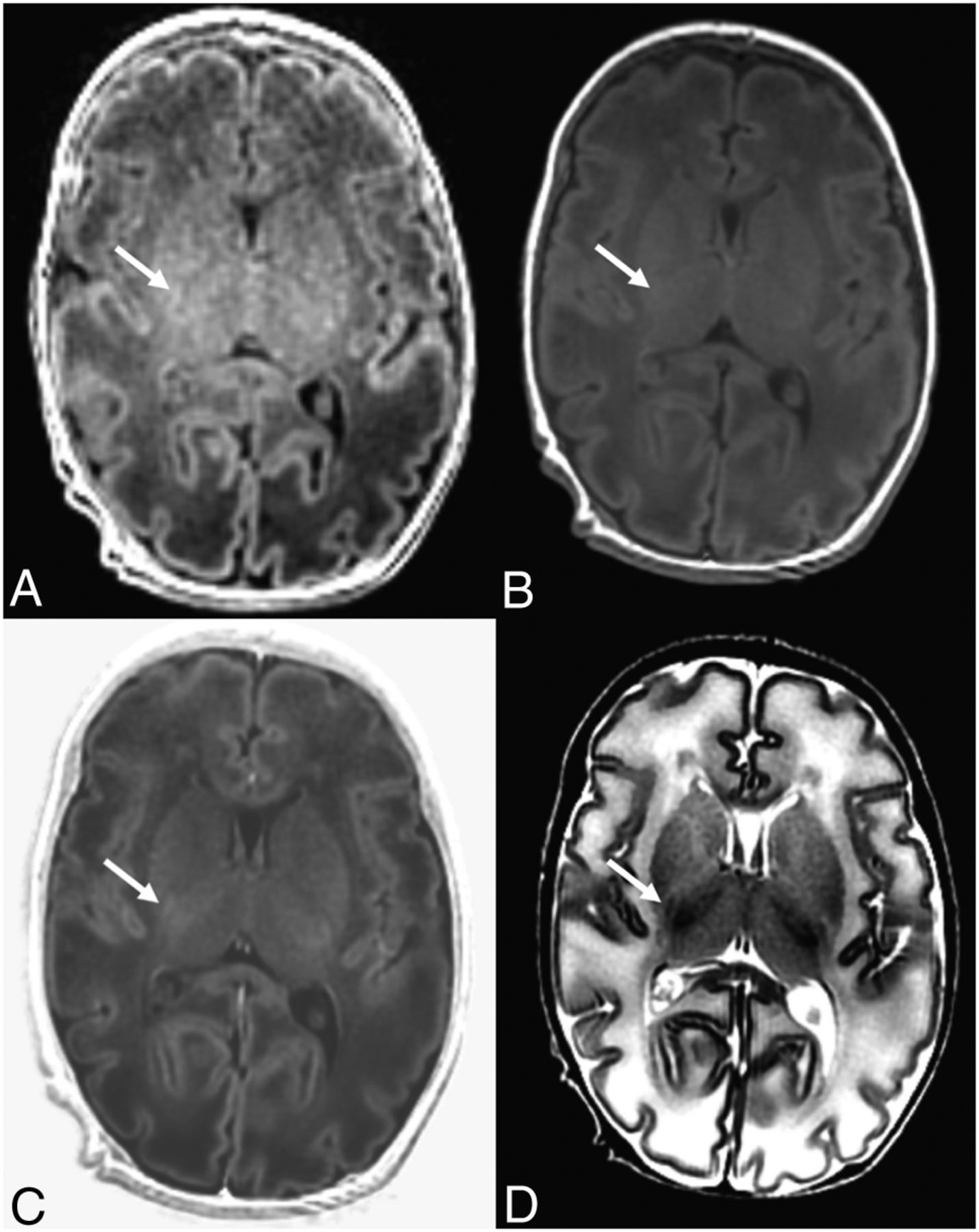
The number and location of the WM lesions found in the 10 infants using the 3 sequences are summarized in Table 4. Several lesions that appeared on FSPGR were not detectable on the synthetic PSIR images (Fig 3). Among the 10 infants with punctate WM injuries, FSPGR revealed a total of 67 lesions, whereas both synthetic T1WI and PSIR revealed 24 lesions. The number of lesions detected using FSPGR (3.35 ± 3.62) was significantly higher than the number of lesions detected using synthetic T1WI (1.2 ± 2.89, P = .002) and synthetic PSIR (1.2 ± 3.24, P = .001). The mean relative differences in the numbers of lesions for synthetic PSIR versus FSPGR and synthetic PSIR versus T1WI were −67.2% and 0%, respectively. The mean of the cranial-to-caudal diameters of punctate WM lesions that were not detectable on synthetic PSIR was 1.57 ± 0.27 mm.
Number of punctate WM lesions detected on FSPGR, synthetic T1WI, and synthetic PSIR in the 10 patients

A 7-day-old neonate who underwent brain imaging due to an apnea event. There are multifocal high signal intensity lesions in the WM, which are readily detectable on both the FSPGR (A) and synthetic PSIR (B) images (short arrows). However, some of the lesions only appear on the FSPGR (long arrow) and not on the synthetic PSIR image.
Discussion
In this study, we found that synthetic PSIR could be a practical imaging sequence for assessing brain maturation both quantitatively and qualitatively in infants. Synthetic PSIR showed significantly higher tissue contrast compared with conventional 3D-T1WI, synthetic T1WI, and T2WI. In our qualitative assessment, synthetic PSIR showed comparable or higher image quality or myelination degree than 3D-T1WI or synthetic T1WI. On the other hand, punctate WM injuries were better detected with 3D-T1WI than with synthetic PSIR.
Synthetic MR imaging is a time-efficient imaging technique that can generate multiple synthesized images at a single acquisition.2,16,17 A few studies have shown that synthetic MR imaging can be used in children2,10,18 as well as in adults.12,19 However, while one of these previous studies did compare the value of synthetic T1WI, T2WI, and FLAIR with conventional sequences,2 the value of synthetic PSIR has not been evaluated in any study that we know of.
In our study, tissue contrast was superior with synthetic PSIR compared with synthetic T1 or FSPGR, and this result is consistent with those of a previous study using conventional PSIR.20 The previous study compared contrast between GM and WM but did not compare contrast between uWM and mWM. PSIR provides a greater range of signal intensity compared with FSPGR and T1WI with conventional magnitude reconstruction, resulting in higher tissue contrast.21 This is possible by additively combining positive and negative longitudinal magnetization in PSIR images, in contrast to magnitude images without any directional component of magnetization.
According to our results, synthetic PSIR showed higher tissue contrast than conventional T2WI. This is in line with the previous qualitative comparison study that showed higher contrast with the PSIR sequence compared with the T2 spin-echo sequence.20 With a decrease in water content and an increase in lipids and protein levels, mWM appears to be hyperintense compared with uWM or GM on T1WI, while mWM on T2WI shows decreased signal intensities.1,22,23 In addition, the milestones of normal maturation are different between T1WI and T2WI.23 Therefore, a direct comparison of contrast between T2WI and PSIR images has limited value.
We also showed that for image quality, synthetic PSIR showed the highest level of qualitative GM-WM among the 3 sequences. Recently, conventional and synthetic PSIR were compared for the detection of cortical lesions in patients with multiple sclerosis.16 In that study, synthetic PSIR showed similar sensitivity to conventional PSIR.16 We did not acquire conventional PSIR, so we could not compare its performance with that of synthetic PSIR in the infant brain. A prospective study on this subject is needed in the future.
Assessing myelin development can be crucial in infants. This is because many disorders are associated with delayed or abnormal myelination, and early detection is essential for early treatment and better prognostication.24 Myelination assessment has been facilitated by the introduction of MR imaging, and there have been many attempts to evaluate myelination in infants more noninvasively and accurately. The high signal intensity observed on PSIR with neural development reflects the shorter longitudinal relaxation times of water protons in mWM. Water content decreases in mWM, and this may induce a decrease in the relaxation times of the water protons.25 Conversely, lipid and protein levels increase in mWM. These changes in the developing brain result in signal intensity changes on MR imaging.22
Therefore, the assessment of myelination degree in our study reflects the ability to find clinically relevant features using different sequences. In a past study with children, myelination patterns observed with synthetic T1WI were compared with those observed with conventional T1WI, and the estimated age based on myelination degree was found to be similar between both sequences.10 Our qualitative results regarding myelination degree were superior with synthetic PSIR in the CP or posterior limb of the internal capsule. There was no significant difference in myelination degree in the anterior limb of the internal capsule, frontal WM, and occipital WM. This is probably because myelination was limited in those regions as our subjects were young, with a mean corrected gestational age of 42 weeks. If a larger group of subjects with older ages were included, there might have been significant differences in the above-mentioned regions as well. Synthetic MR imaging may not only allow quantitative assessment3 but also enhance the qualitative assessment of myelination degree in children.
As a subgroup analysis, we evaluated the potential of synthetic PSIR to detect punctate WM injuries. Reports have shown that most preterm neonates have abnormal neuroimaging findings such as parenchymal volume loss, cystic change, or enlargement of ventricles.13,14 Among such abnormal findings in preterm neonates, WM signal abnormalities are referred to as “periventricular white matter injuries of prematurity.” Because tissue contrast comparisons showed higher contrast with synthetic PSIR images, we expected the periventricular WM lesions to appear more prominently on synthetic PSIR than on FSPGR images. However, periventricular WM lesions were more readily and sensitively detected using FSPGR rather than synthetic PSIR imaging. We speculate that this finding is most likely due to higher spatial resolution in 3D-FSPGR compared with 2D synthetic PSIR sequences. This is because the mean cranial-to-caudal diameter of lesions that were not detectable with synthetic PSIR (1.57 mm) was smaller than the slice thickness of 2D synthetic images (3 mm) but larger than that of 3D FSPGR (1 mm). In addition, the number of lesions detected with synthetic T1WI and PSIR imaging were the same. Another possible reason is the pathologic characteristics of punctate WM lesions, which are different from normal brain tissue. The high T1 signal intensities of punctate WM lesions indicate focal necrosis with macrophages and foci of activated microglia.26 In addition, hemorrhagic components commonly accompany punctate WM injuries.27,28 Because the lesions have shorter T1 values than surrounding normal WM, if we applied an optimal null point of normal WM (ie, optimal TI value), a higher sensitivity for detecting WM lesions might be possible. Future studies comparing the contrast of WM lesions and surrounding normal WM lesions between synthetic PSIR and other sequences would also be helpful. Because neonatal MR imaging plays a role in predicting neurodevelopmental outcomes and the detection of periventricular WM lesions is one such marker, radiologists have to be aware that 2D synthetic PSIR imaging has limited value when detecting punctate WM lesions.
This study has some limitations. First, the study group included infants and neonates with brain abnormalities. Although we included subjects without visual abnormalities for qualitative comparison, these subjects cannot reflect a healthy population. Myelination degree of the abnormal brain such as in hydrocephalus is noticeably different from that of the normal brain.29 Therefore, the 4 sequences we compared in this study do not reflect the myelination of the healthy population. Second, 2 radiologists with different degrees of experience in pediatric neuroradiology performed the qualitative assessment. Inter- and intraobserver variability was not evaluated, and differing experience levels in pediatric neuroradiology may have caused the discordant results between the 2 radiologists. Third, we did not optimize TR, TE, and TI for infants when generating synthetic PSIR from synthetic MR imaging. With synthetic MR imaging, we can create multiple different contrast images combining distinctive TR, TE, and TI.30 Future studies with optimized TR, TE, and TI could further improve the image quality of synthetic PSIR in the infant population.
Conclusions
Synthetic PSIR has the potential to improve tissue contrast, image quality, and myelination degree assessment when evaluating the brains of infants compared with conventional sequences and other synthetic images, despite being of limited value when evaluating punctate WM injuries.
Acknowledgments
The authors thank Sung-Min Gho of GE Healthcare Korea for technical assistance.
Footnotes
Disclosures: Hyun Gi Kim—RELATED: Grant: National Research Foundation of Korea grant.
This work was funded by the National Research Foundation of Korea (NRF-2017R1D1A1B03034768).
Paper previously presented at: 74th Korean Congress of Radiology, September 2018, Seoul, Republic of Korea.
Indicates open access to non-subscribers at www.ajnr.org
REFERENCES
- Received March 23, 2019.
- Accepted after revision June 17, 2019.
- © 2019 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.