
Abstract
BACKGROUND: Surveillance imaging of previously unruptured, coiled aneurysms remains routine even though reports of rupture of these aneurysms are extremely rare.
PURPOSE: We performed meta-analysis to examine long-term rupture risk over ≥1-year follow-up duration in patients with unruptured intracranial aneurysm who underwent endovascular therapy.
DATA SOURCES: Multiple databases were searched for relevant publications between 1995 and 2018.
STUDY SELECTION: Studies reporting outcome of long-term rupture risk over ≥1-year follow-up in treated patients with unruptured intracranial aneurysms were included.
DATA ANALYSIS: Random effects meta-analysis was used, and results were expressed as long-term rupture rate per 100 patient-year with respective 95% CIs. For ruptured aneurysms during follow-up, data were collected on size and completeness of initial Treatment.
DATA SYNTHESIS: Twenty-four studies were identified. Among 4842 patients with a mean follow-up duration of 3.2 years, a total of 12 patients (0.25%) experienced rupture of previous unruptured intracranial aneurysms after endovascular treatment. Nine of these 12 patients harbored aneurysms that were large, incompletely treated, or both. A total of 2 anterior circulation, small, completely coiled aneurysms subsequently ruptured. The long-term rupture rate per 100 patient-year for unruptured intracranial aneurysms treated with endovascular therapy was 0.48 (95% CI, 0.45–0.51). Retreatment was carried out in 236 (4.9%) of these 4842 patients.
LIMITATIONS: A limitation of the study is that a lack of systematic nature of follow-up and mean follow-up duration of 3.2 years are not sufficient to make general recommendations about aneurysm followup paradigms.
CONCLUSIONS: Given a 5% retreatment rate, postcoil embolization spontaneous rupture of previously unruptured, small- and medium-sized, well-treated aneurysms is exceedingly rare.
ABBREVIATIONS:
- CI
- confidence interval
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PY
- patient-year
- UIA
- unruptured intracranial aneurysm
The advent and popularization of endovascular techniques have led to a growing paradigm shift in coil embolization and decline in historical microsurgical clipping techniques for the treatment of unruptured intracranial aneurysms (UIAs) over the past 20 years or so. Multiple studies have emphasized the follow-up imaging of patients treated with endovascular therapy due to concerns for its long-term durability and increased recurrence rates coupled with greater need for retreatment compared with microsurgical clipping.1⇓-3 However, even though recurrences after endovascular therapy are reported in up to 30% of treated aneurysms, reports of spontaneous rupture of previously unruptured, coiled aneurysms have been unusual. Even though such spontaneous ruptures are rare, most practitioners carry out long-term surveillance imaging and offer retreatment for previously unruptured, coiled aneurysms.4,5 Surveillance imaging carries substantial cost and may cause ongoing anxiety, and retreatment carries risk of stroke.6 Thus, it would benefit the community to better understand the rate of spontaneous rupture of coiled, unruptured aneurysms.
To date, there is lack of randomized controlled trials as well as a paucity of aggregated data regarding rupture risk for both small and large UIAs treated with endovascular techniques. We therefore performed a systematic review and meta-analysis of studies to examine the long-term risk of rupture over a follow-up duration of ≥1 year in patients with UIA who underwent endovascular therapy.
MATERIALS AND METHODS
Literature Search
The current study adheres to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The electronic databases Ovid MEDLINE, Ovid EMBASE, and Scopus were systematically examined to locate relevant studies by using predefined search criteria. The search strategy was designed and conducted by a medical reference librarian with input from the authors. Controlled terminology supplemented with keywords was used to search for unruptured cerebral aneurysm, unruptured brain aneurysm, unruptured intracranial aneurysm AND endovascular treatment of aneurysm, coiling of aneurysm, endovascular coiling, endovascular embolization, elective coil treatment AND long-term follow-up, long-term results, aneurysm rupture, rupture of aneurysm. The search was confined to investigations that were published between January 1995 and December 2018. The search strategy is available in the On-line Appendix.
Three independent investigators scanned all manuscripts and performed data extraction. Abstracts or conference papers were excluded because of insufficient data. All retrieved studies were examined, and any potential overlapping data were omitted. Three reviewers performed the final screening of reports for inclusion in the meta-analysis. In the event of any disagreement, a general consensus was met between reviewers after further extensive review of the full-text articles. In addition, all references cited in the identified articles were manually searched for potentially relevant studies.
Study Eligibility
The inclusion criteria for studies in the analysis were 1) studies assessing long-term risk of rupture in patients with UIA who underwent endovascular therapy, 2) studies examining previously unruptured small (<10 mm) and large (>10 mm) intracranial aneurysms that underwent endovascular treatment, and 3) studies reporting mean follow-up duration of ≥1 year after endovascular therapy. Studies published before 1995 were excluded from this meta-analysis. Studies or patients in the included studies were also excluded if they reported giant (>25 mm) or ruptured aneurysm at initial presentation. Additionally, animal or in vitro studies as well as studies with ≤10 patients were excluded as were studies published in languages other than English without any available translation.
Data Collection
Three independent investigators (A.R., S.M.S., and M.A.) extracted data with subsequent verification. The following data were collected for each eligible investigation: year of publication, patient demographics, aneurysm location, mean follow-up duration, and number of patients with ruptures. For documented ruptured aneurysms during follow-up, we collected data on size and completeness of initial treatment (On-line Table 2).
Methodologic Quality
Because the studies were uncontrolled (case series), the methodologic quality of these series (ie, risk of bias) was analyzed by using a modified tool suggested by Murad et al.7 Each study was judged on 5 items categorized into 4 groups: 1) selection bias (whole experience of the treating center, ie, the study reporting consecutive patients at the recruiting center and therefore less likelihood of selective reporting of the patients who had better outcomes), 2) ascertainment bias (ascertainment of exposure and outcome of interest), 3) causality bias (adequate follow-up period for outcomes to occur), and 4) reporting bias (sufficient details to allow for replication of research). For the purposes of the current study, we determined that the risk of bias depended mainly on 2 factors: selection domain and the independent or blinded assessment of outcomes.
Outcome Variables
For the current study purposes, the following outcome was assessed: long-term rupture of UIA following endovascular treatment over a follow-up duration of ≥1 year.
Statistical Analysis
From each eligible study, data were extracted for the number of patients with UIA and rupture after endovascular therapy during a follow-up duration of ≥1 year. Event rates were expressed as long-term (≥1 year) rupture rate per 100 patient-year (PY) with respective 95% confidence intervals (95% CIs) that were derived from the Poisson distribution. A continuity correction factor of 0.001 was used to address studies with zero event rates. Random effects meta-analysis was used for pooling across studies.8 The I2 statistic was used to express the proportion of heterogeneity that is not attributable to chance.9 Meta-analysis was conducted by using STATA Version 15 (StataCorp).
RESULTS
Literature Search
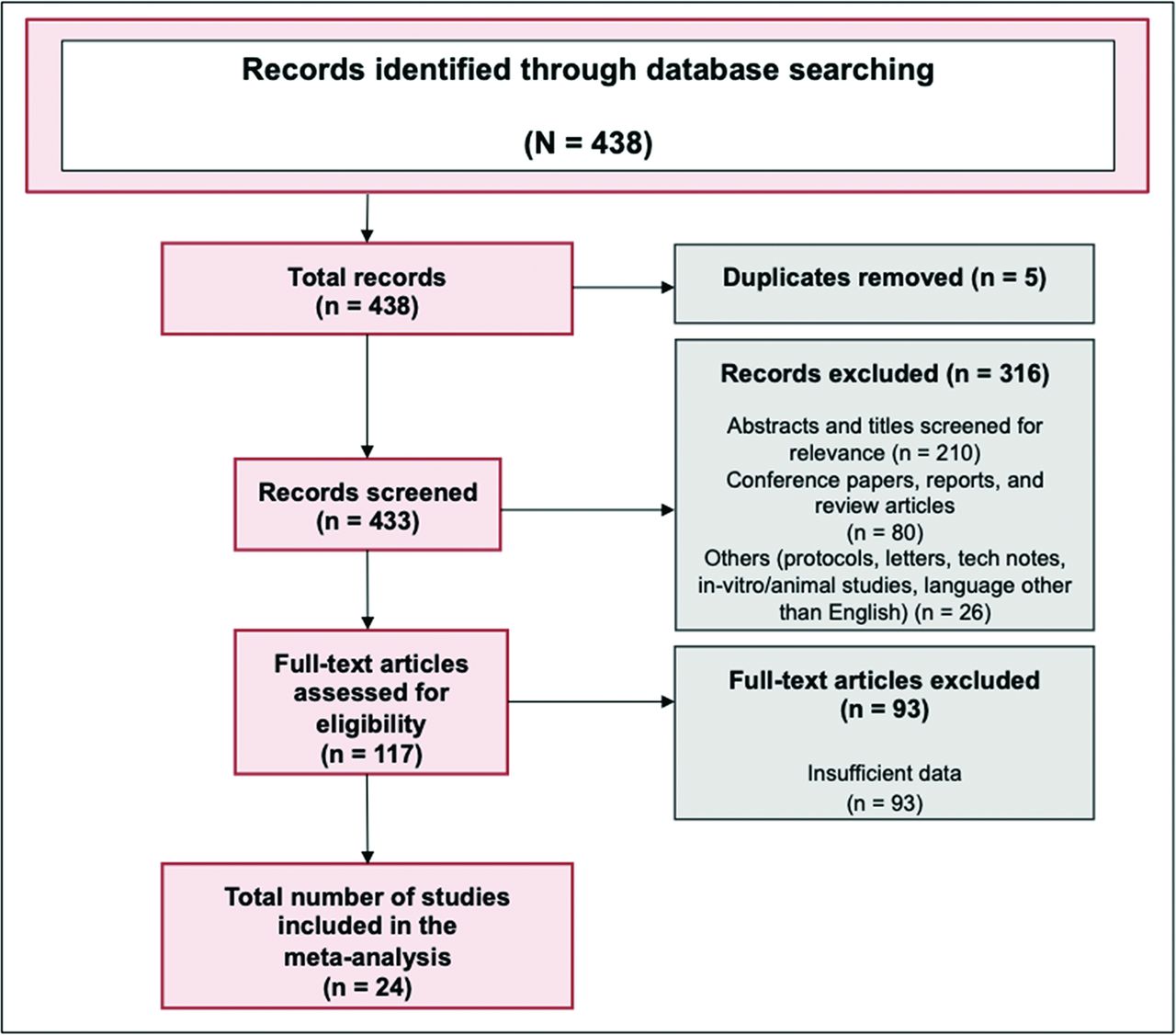
We identified 438 articles from the literature search. After removing duplicates, 433 articles were screened by title and abstract. Of these, 122 articles were read full-text. A total of 24 studies met the eligibility criteria and were included in the meta-analysis. A PRISMA flow chart of the search and selection process of the articles is shown in Fig 1.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram.
Baseline characteristics of each study are listed in On-line Table 2. A total of 5309 patients were included who were followed-up for ≥1 year after endovascular therapy. The mean age within studies was 55.0 ± 6.0 years, and the mean follow-up duration was 3.2 years. The largest study had 2035 patients,10 and the smallest study had 13 patients.11 Four studies were multicenter,10,12⇓-14 and 20 were single-center studies.11,15⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓-33 Among all included studies, the longest mean follow-up duration was 15.5 years,14 and the shortest follow-up duration was 1 year.24,27,30 Methodologic quality was moderate to high in all included studies (On-line Table 3).
Long-Term Rupture Risk with Unruptured Aneurysms Treated with Endovascular Therapy
Among 4842 patients with a mean follow-up duration of 3.2 years, a total of 12 patients (0.25%) experienced rupture of previously unruptured aneurysms following endovascular treatment. Nine of these 12 patients harbored aneurysms that were either large, incompletely treated, or both. A total of 2 anterior circulation, small, completely coiled aneurysms subsequently ruptured. All these ruptures of previous UIAs were reported more than 1 year after the initial endovascular treatment (Table). The long-term rupture rate per 100 PY for UIAs treated with endovascular therapy was 0.48 (95% CI, 0.45–0.51) (Fig 2). In particular, 4.9% of these patients (236 among 4842 patients) underwent retreatments for previously treated UIAs (On-line Table 1).
Studies that reported long-term aneurysm rupture following endovascular therapy
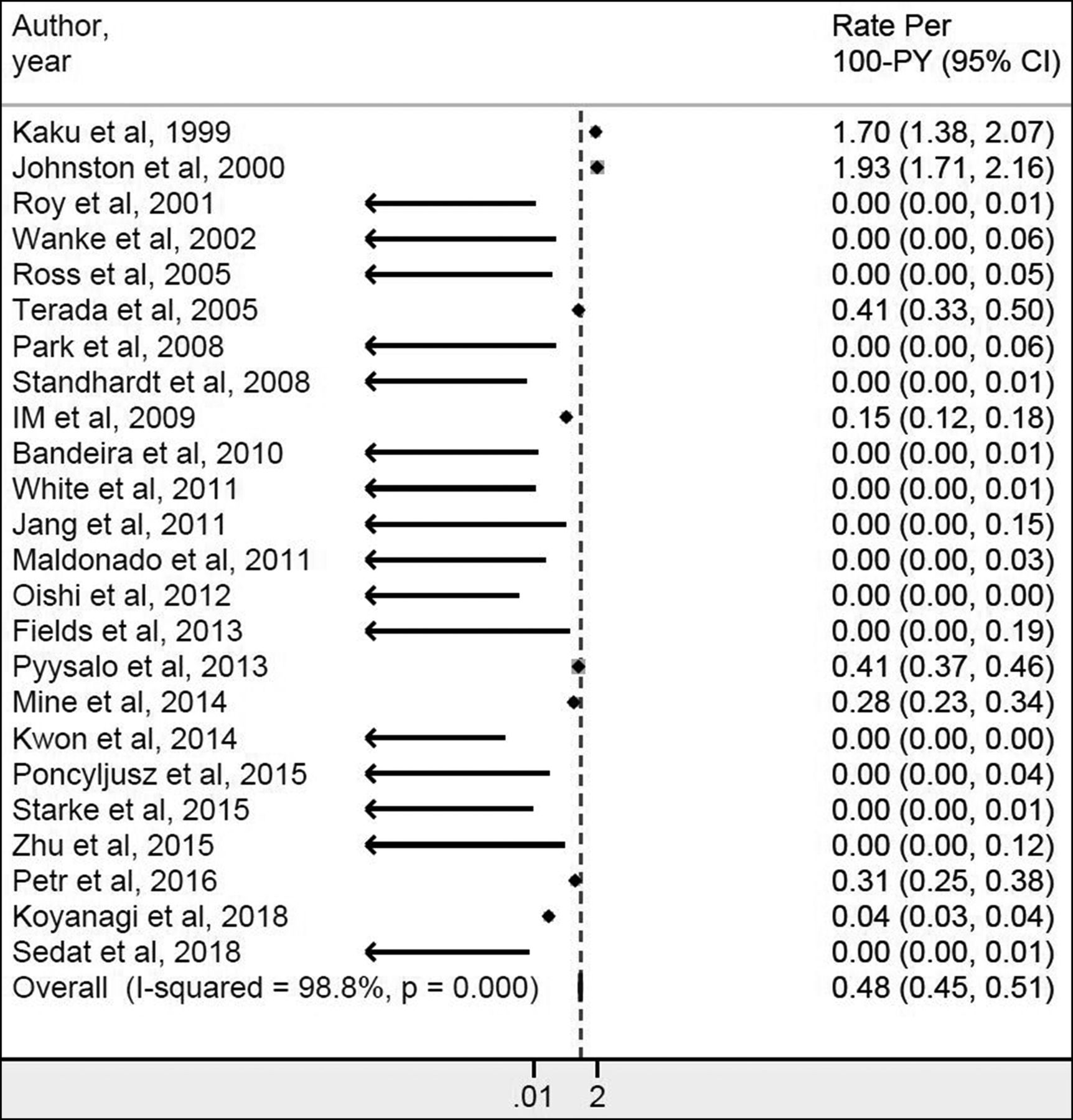
Forest plot for long-term (≥1 year) rupture rate per 100 patient-year (PY) with respective 95% confidence intervals (95% CIs).
Heterogeneity
The I2 value was 98.8% for long-term rupture rate per 100 PY, suggesting high heterogeneity. The low numbers precluded analysis of the reasons for this apparent heterogeneity.
DISCUSSION
This systematic review and meta-analysis revealed that the subsequent rupture of treated UIAs is extremely unusual and was nearly nonexistent among well-treated, small aneurysms. Overall, we noted that about 1 aneurysm ruptured every 200 PY, and most of those few cases represented either small or initially incompletely treated aneurysms. It is potentially notable that the 12 ruptures were spread out over case series published between 1999 and 2018. We fully acknowledge that the true rupture rate of coiled aneurysms remains unknown because about 5% of the patients in this meta-analysis underwent retreatment. Furthermore, it is plausible that these 5% were a high-risk group that may have gone on to rupture. We also acknowledge that a mean follow-up of 3.2 years is not sufficient to make general recommendations about aneurysm surveillance imaging, and a MR angiography every 5 years is not a big request among patients who have a propensity to form life-threatening brain aneurysms. To this end, prior studies have also reported predisposing factors that may predict aneurysm recurrence, which is essentially the biggest risk factor for posttreatment rupture.34 Even so, the data contained herein should prompt additional discussion and scrutiny regarding the routine use of surveillance imaging and retreatment in patients with previously treated UIA.
In particular, most reports of rupture of aneurysms previously treated with endovascular therapy were in large,14,20,32 suboptimally coiled aneurysms,16,29 or both.28 Further still, the rates of rupture of UIA may vary widely depending on aneurysm location, size, history of other (ruptured) aneurysms, positive family history, and/or smoking history. The current study brings robust meta-analytic techniques to further underscore the significance of low rupture rates among UIAs previously treated by endovascular therapy and represents a systematic aggregation of long-term rupture rate after endovascular therapy during a follow-up duration of ≥1 year. It extends the findings of smaller studies, which may be limited by factors such as small sample size or single-center design, and it broadens generalizability.
The extremely low rate of posttreatment rupture is not at all surprising, given the low rates of spontaneous rupture of untreated UIA. Based on outcomes from ruptured aneurysm case series, it is clear that coil embolization is highly protective of rerupture, diminishing rerupture rates from about 50% for untreated aneurysms to <2% for coiled aneurysms. A similar relative decrease in rupture rate for UIA would bring down an already low rate to a vanishingly low rate, rendering routine surveillance imaging, at least in small, completely coiled aneurysms, potentially unnecessary. Our study carried out a complete analysis of the best existing data on rupture of previously unruptured, coiled aneurysms and has shown that rupture is extremely rare. It will hopefully prompt future researchers to catalog all relevant data, including reasons for retreatment, in future publications. We acknowledge that noninvasive imaging with MR angiography at extended intervals would not be unreasonable until further data are available.
This study has limitations. There was lack of a systematic nature of follow-up among included studies with imaging modalities such as digital subtraction angiography and MR angiography. We were unable to stratify outcome of long-term rupture by size of aneurysms because specific data from most of the studies cannot be used because of a lack of detailed information for statistical analysis purposes. Additionally, a mean follow-up duration of 3.2 years is not sufficient to make general recommendations about aneurysm follow-up paradigms. As noted, about 5% of aneurysms underwent retreatment, so we cannot exclude the possibility that some of these retreated aneurysms would have gone on to rupture without retreatment. Further still, specific reasons for retreatment were not provided in the available studies, though we can surmise that recanalization likely was the most common cause. For this reason, our study can be best applied in the setting of patients who were not subsequently retreated, for any reason, which remains most patients. There is a lack of a core laboratory and lack of standardization in reporting specific data, such as size criteria defining an aneurysm as “large,” what constitutes a suboptimally coiled aneurysm, or even agreement in how to measure a complex-shaped aneurysm. Furthermore, variability exists in the type (MR angiography vs digital subtraction angiography) and intervals of surveillance imaging. Techniques and technology also dramatically changed during the study period, which may affect results, as well as the applicability of the practices and rupture rate in the 1990s to today’s practices and surveillance philosophies. We also acknowledge that correlation of rupture with myriad demographic features would be instructive. However, the vanishingly rare event rate (12 cases among almost 5000 aneurysms) renders any such subanalysis or correlative study impossible. Another limitation is that particularly in large metropolitan medical centers, the ability to reliably track for subsequent hemorrhage may be susceptible to underreporting, and given that this is a literature review, we do not have access to systematic databases such as the Veterans Affairs system. Last, this review includes studies of various designs, each of which may have its own set of limitations.
CONCLUSIONS
Given a 5% retreatment rate, post–coil embolization spontaneous rupture of previously unruptured, small- and medium-sized, well-treated aneurysms is exceedingly rare. Future studies are warranted with complete follow-up reporting to address the basic question about the risk of hemorrhage.
Footnotes
Grant support: This research was supported by AHA postdoctoral fellowship award # 19POST34381068 and NIH grant # NS076491.
Disclosures: Asim Rizvi—RELATED: Grant: 19POST34381068, Comments: American Heart Association Grant, AHA postdoctoral fellowship award*; Support for Travel to Meetings for the Study or Other Purposes: 19POST34381068, Comments: American Heart Association Grant, AHA postdoctoral fellowship award*; Other: NS076491, Comments: NIH grant*; UNRELATED: Grants/Grants Pending: 19POST34381068, Comments: This research was supported by AHA postdoctoral fellowship award # 19POST34381068 and NIH grant # NS076491.* Seyed Mohammad Seyedsaadat—RELATED: Grant: AHA 2 years postdoctoral research fellowship. Ram Kadirvel—RELATED: Grant: NIH, Comments: R01 NS076491 and R43 NS110114; Other: Cerenovus, Insera Therapeutics LLC, Marblehead Medical LLC, Microvention Inc, MIVI Neuroscience Inc, Neurogami Medical Inc, Triticum Inc, Comments: Research contracts; UNRELATED: Stock/Stock Options: Neurosigma Inc.* David Kallmes—UNRELATED: Grants/Grants Pending: Medtronic, Microvention, NeuroSigma, Neurogami, General Electric, Comments: Research support*; Stock/Stock Options: Superior Medical Experts, Comments: Founder/stockholder. *Money paid to institution.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received November 17, 2019.
- Accepted after revision March 19, 2020.
- © 2020 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.