
Abstract
BACKGROUND AND PURPOSE: About 20% of patients with acute ischemic stroke due to large-artery occlusion do not achieve recanalization with mechanical thrombectomy. We aimed to determine whether the speed of retrieval of the stent retriever influences the efficacy in removing different clot types.
MATERIALS AND METHODS: Sixty mechanical thrombectomies were performed using an in vitro pulsatile cerebrovascular circulation model with controlled pressure and flow rate. Experiments were dichotomized into fast and slow retrieval using a wedging technique, in which the stent retriever and distal catheter are retrieved together. We used 3 different clot types: erythrocyte-rich, fibrin-rich, and friable clots. Primary end points were complete (TICI 3) and successful (TICI 2b–3) recanalizations. Secondary measures were distal and new territory embolizations.
RESULTS: Fast retrieval was more frequently associated with complete (RR = 1.83; 95% CI, 1.12–2.99) and successful recanalization (RR = 1.50; 95% CI, 1.03–2.19) than slow retrieval, without a difference in distal embolization (RR = 0.75; 95% CI, 0.29–1.90). There were no emboli in a new territory. The advantage of fast retrieval over slow retrieval differed according to the clot composition, with a stronger effect with fibrin-rich clots with regard to complete (RR = 4.00; 95% CI, 1.11–14.35; Pint = .04) and successful (Pint = .10) recanalization.
CONCLUSIONS: In our experimental model, a fast removal improved recanalization rates of mechanical thrombectomy, especially in the case of fibrin-rich clots. An in vivo confirmation is warranted to see whether our findings can have an impact in clinical practice.
ABBREVIATIONS:
- DC
- distal catheter
- MT
- mechanical thrombectomy
- RR
- relative risk
- Pint
- P interaction
- RBC
- red blood cell
- SR
- stent retriever
Mechanical thrombectomy (MT) is considered the first-line therapy for selected patients with acute ischemic stroke with a proximal cerebral artery occlusion.1⇓-3 The dramatic technological improvements, such as the combined use of stent retrievers (SRs) and distal catheters (DCs), have led to recanalization rates unreached before.4,5 With the goal of increasing clot entrapment, techniques in which the thrombus is wedged between the SR and DC have become more popular.6⇓-8 Nevertheless, a successful recanalization is still not obtained in around 20% of patients.9 Potential issues may arise from the retrieval technique itself, the interactions between device-thrombus, and the clot composition.9,10 To date, only a few experimental studies have investigated th1053e interaction of the SR with artificial thrombi,11⇓⇓⇓⇓⇓⇓-18 and the influence of the retrieval speed on MT success has never been explored. The most instinctive approach to remove an SR is to pull it back slowly to save the vessel from potential damage and the clot from breaking.5,9 However, a fast removal can mobilize the clot suddenly and allow application of higher pulling force to enhance wedging. We aimed to determine whether the speed of retrieval influences the efficacy in removing clots.
MATERIALS AND METHODS
Study Setting
Using an in vitro model of cerebrovascular occlusion, we performed a total of 60 thrombectomy experiments (1 pass only for each), dichotomized into 2 groups according to the speed of retrieval of the SR-DC unit (fast or slow retrieval). The experiments were performed with 3 types of clots. Half of the tests were performed with Solitaire 2 (4 × 20 mm) (Medtronic) and half with Embotrap II (5 × 21 mm) (Neuravi/Cerenovus). Consequently, there were 2 speeds × 3 types of clots × 5 maneuvers each × 2 devices, corresponding to 60 MTs in total.
Flow Model
In brief, the model is made of silicone channels (Elastrat) mimicking the human anterior intracranial circulation. The flow model had sharp angles and large perforator diameters to create challenging conditions, and a posterior flow was also added for complete circle of Willis flow. A saline solution at 37°C was pumped through the model with a 430-mL/min flow rate and 110/60 mm Hg pulsatile pressure. A fresh clot was introduced into the model to simulate the vessel occlusion (Fig 1).

Flow model.
Clots Types
We used 3 different types of clot depending on their composition (Fig 2): red blood cell (RBC)-rich, fibrin-rich, and hybrid clots (representing the challenges of a friable clot). The RBC-rich clots were formed from whole ovine blood by allowing the blood to clot spontaneously. The fibrin-rich clots were prepared by first spinning down the blood sample in a centrifuge and recombining 5% RBCs with 95% plasma to produce a fibrin-rich clot.19 Hybrid clots were prepared specifically to represent the challenges of friable clots. They were prepared by cutting spontaneously formed clot (RBC-rich) into 1- to 1.5-mm cubes. Ten of these cubes were inserted into a 2.5-mm diameter silicone tube where they were lightly glued together with a mixture of blood and thrombin. Once the mixture was fully set (30 minutes), the hybrid clot was carefully removed from the silicone tube. The size of all clot types was standardized at a 2.5- mm diameter by 10-mm length. Clots were introduced into the model and navigated into the M1 or M2 MCA segment using the anterograde flow of the circulating fluid. A 3-minute embedding time was respected.

Clot types. The figure shows the 3 types of clot during MT inside the model: RBC-rich (left), fibrin-rich (middle), and hybrid friable clot (right).
Thrombectomy Technique
MT consisted of a microcatheter (Rebar-18; Medtronic) navigated through a distal catheter (Sofia Plus; MicroVention), which was advanced into a guide catheter (Neuron Max; Penumbra). We used 0.014-inch microwires (Traxcess 14; MicroVention) to cross the thrombus. The proximal third to half of the stent retriever was deployed across the clot. Thereafter, the DC was advanced into the proximal M1, and the microcatheter was withdrawn inside the DC. After 3 minutes, the SR was retrieved until half was inside the DC or until resistance was felt. Then, the system was retrieved completely as a single unit (SR + DC + microcatheter) with a continuous movement.7,8 No suction was applied during removal. A fast retrieval was performed in 5 seconds maximum, and a slow retrieval, in 15 seconds minimum. To ensure reproducibility, we performed 10 training experiments before starting the study. The speed was calculated by dividing the time (measured by an assistant with a stopwatch) by the distance (measured from the guide catheter tip to the proximal limit of the thrombus with a flexible meter). The MT result was instantly graded by the performing physician according to an adapted TICI score: complete recanalization (TICI 3), recanalization with small emboli exceeding the model limits (TICI 2b), recanalization but emboli blocked distally (TICI 2a), a piece of thrombus removed but persistent occlusion (TICI 1), and no recanalization (TICI 0). Distal emboli corresponded to part of the initial thrombus migrating in the MCA territory farther than the distal limit of the model (ie, <1.5 mm in diameter). Emboli in a new territory were any clots migrating into another area. Primary outcome measures were complete (TICI 3) and successful recanalization (TICI 2b–3). Secondary measures were distal and new territory emboli. All experiments were recorded and reviewed for verification purposes (On-line Videos).
Statistical Analyses
Distribution normality was assessed using the Kolmogorov-Smirnov test. Continuous variables were described as mean ± SD or median and interquartile range and were compared using the Student t test or Mann-Whitney U test. Categoric variables were presented as counts and compared using the χ2 or Fisher exact test. Relative risks and their 95% confidence intervals were calculated. Interaction analyses were performed using the Cochran-Mantel-Haenszel test. Analyses were performed using STATA software (Realease 15.0; StataCorp).
RESULTS
Fast-versus-Slow Retrieval
The mean time of retrieval was 2.4 ± 1.2 seconds in the fast group and 27.3 ± 6.8 seconds in the slow group (P < .001). Overall, fast retrieval led to higher rates of complete (73% versus 40%, P = .01) and successful (80% versus 53%, P = .03) first-pass recanalization than slow retrieval. Fast retrieval was more frequently associated with complete (Relative Risk = 1.83; 95% CI, 1.12–2.99) and successful first-pass recanalization (RR = 1.50; 95% CI, 1.03–2.19) than slow retrieval. Recanalization rates in the whole experiment as well as according to clot type and SR type are shown in Fig 3.
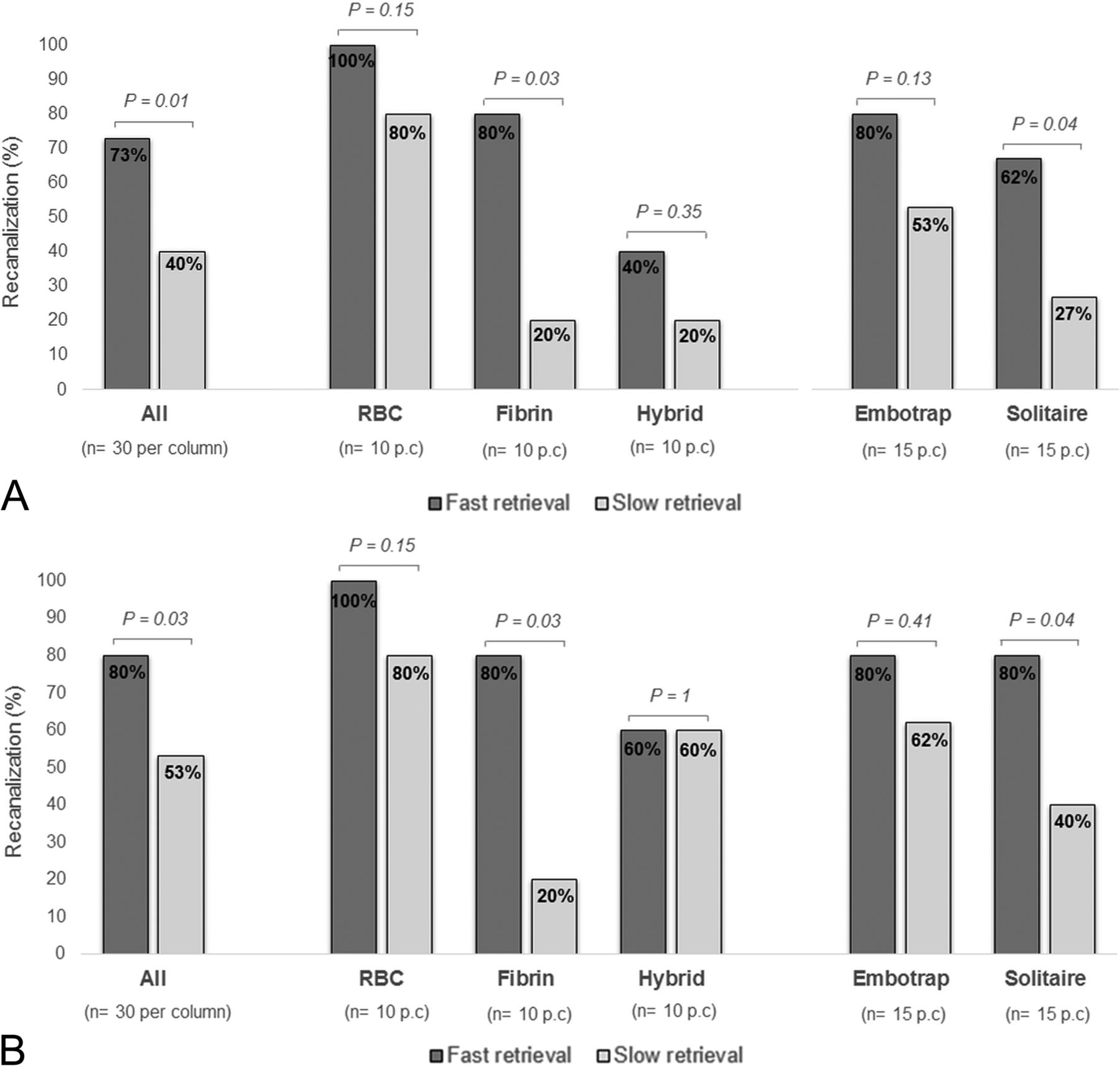
Complete (A) and successful (B) recanalization rates.
Clot Composition
The advantage of fast retrieval over slow retrieval differed according to the clot composition (Fig 4), with a stronger effect obtained with fibrin-rich clots (RR = 4.00; 95% CI, 1.11–14.35) than with RBC-rich (RR = 1.25; 95% CI, 0.92–1.70) and hybrid friable (RR = 2.00; 95% CI, 0.47–8.56) clots with regard to complete recanalization (Pint = .04). This result was similar when considering successful recanalization instead (Pint = .10) (Fig 2).

Interactions analyses. Interaction between the speed of retrieval and the clot type with regard to complete (A) and successful (B) recanalization. Interaction between the speed of retrieval and stent retriever type with regard to complete (C) and successful (D) recanalization.
SR Type
The advantage of fast retrieval over slow retrieval did not differ according to the SR type (Fig 2) with regard to complete recanalization (Pint = .32) or successful recanalization (Pint = .19) (Fig 4).
Distal Embolization
Distal embolization occurred only with hybrid friable clots and was not different between fast (20.0%) and slow (26.7%) retrieval groups (RR = 0.75; 95% CI, 0.29–1.90). There were no emboli in a new territory.
DISCUSSION
Our experimental study showed that a fast retrieval improves recanalization rates, without increasing the rate of distal embolization. It was all the more important that we measured the achievement of complete/successful revascularization after 1 pass, which is associated with significantly higher rates of good clinical outcome.20⇓-22 In this experimental study, we reached 73% and 80% of complete and successful recanalization with 1 pass, while in clinical routine, current thrombectomy techniques yield around 30% and 50% complete and successful recanalization, respectively.20⇓-22 Although not instinctive, a fast removal can mobilize the clot suddenly, allow application of higher pulling force, enhance clot wedging, and minimize loss of apposition during the path of retrieval. Also, it may leave less time for variations of the pulling force, hence avoiding undesired loss of contact between SR and DC. A fast removal did not modify the rate of distal embolization, probably because of an active pinning of the whole thrombus length.
While fast retrieval seems promising in terms of recanalization, an important concern is the clinical safety of this technique. Indeed, human perforating arteries cannot be modeled accurately, and the risk of injury remains unknown. The manufacturers recommend slowly withdrawing the SR as a precaution for safety. When one performs a mechanical retrieval, the perforators may be exposed to excessive force due to stretching and may be rarely sheared off, leading to extravasation. A sudden mobilization of the clot may enhance its retrieval, but the effect on the lenticulostriate arteries is unknown. Thus, the safety of fast retrieval needs to be evaluated in vivo.
The composition and physical properties of the clot can play a key role in the response to MT.9,23⇓-25 We observed a stronger advantage of fast over slow retrieval with fibrin-rich clots. These clots probably account for a large part of MT failures because they are firm and sticky.9,23,24 Fast retrieval, by mobilizing the clot suddenly, may have contributed to better clot trapping. Because imaging features of fibrin-rich thrombi are correlated with decreased revascularization rates,25,26 a fast retrieval might be recommended in such cases, to enhance first-pass revascularization. This is all the more important in that there is the potential for thrombus compression and increasing difficulty of subsequent retrieval after each thrombectomy attempt.9
Our study has potential limitations. First, the model and clots were more representative of embolic stroke types (not atherosclerosis). The circulation model does not fully simulate the human artery, and further in vivo studies are mandatory to confirm our results and evaluate the clinical safety. Also, tortuous anatomy probably has an impact that cannot be measured with our model.22 Second, because we aimed to analyze only factors attributable to the SR, we did not apply aspiration. In all the in vitro attempts, the DC was always in the M1 proximal part, covering the anterior cerebral artery and in the same axis as the clot. In such cases, the need for proximal aspiration was probably less important than when clot and DC are far away from each other (eg, distal M2 clot, or DC still in the ICA) or in a very tortuous M1. Because only 1 specific procedural setup was simulated, it may not translate to other procedures (longer clots, techniques not similar to Aspiration-Retriever Technique for Stroke or stent-assisted vacuum-locked extraction (SAVE technique), and use of a baloon guide catheter). Such setups remain to be tested.
CONCLUSIONS
In our experimental model, a fast removal improved recanalization rates of MT, especially in case of fibrin-rich clots, which are known to be challenging to remove. An in vivo confirmation is warranted to see whether our findings can impact clinical practice.
Footnotes
Disclosures: Laurent Pierot—UNRELATED: Consultancy: Balt, MicroVention, phenox, Vesalio. Mahmood Mirza—UNRELATED: Employment: Cerenovus; Stock/Stock Options: Cerenovus. Matthias Gawlitza—UNRELATED: Expert Testimony: MicroVention, Comments: member of the Clinical Event Committee for a company-initiated study on a neurovascular device; Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: Neuravi/Cerenovus, phenox, MicroVention, Comments: travel and accommodations for training workshops of the respective companies; Other: Lin. Michael Gilvarry—UNRELATED: Employment: Cerenovus; Stock/Stock Options: Cerenovus.
References
- Received January 17, 2020.
- Accepted after revision March 2, 2020.
- © 2020 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}