
Article Figures & Data
Figures
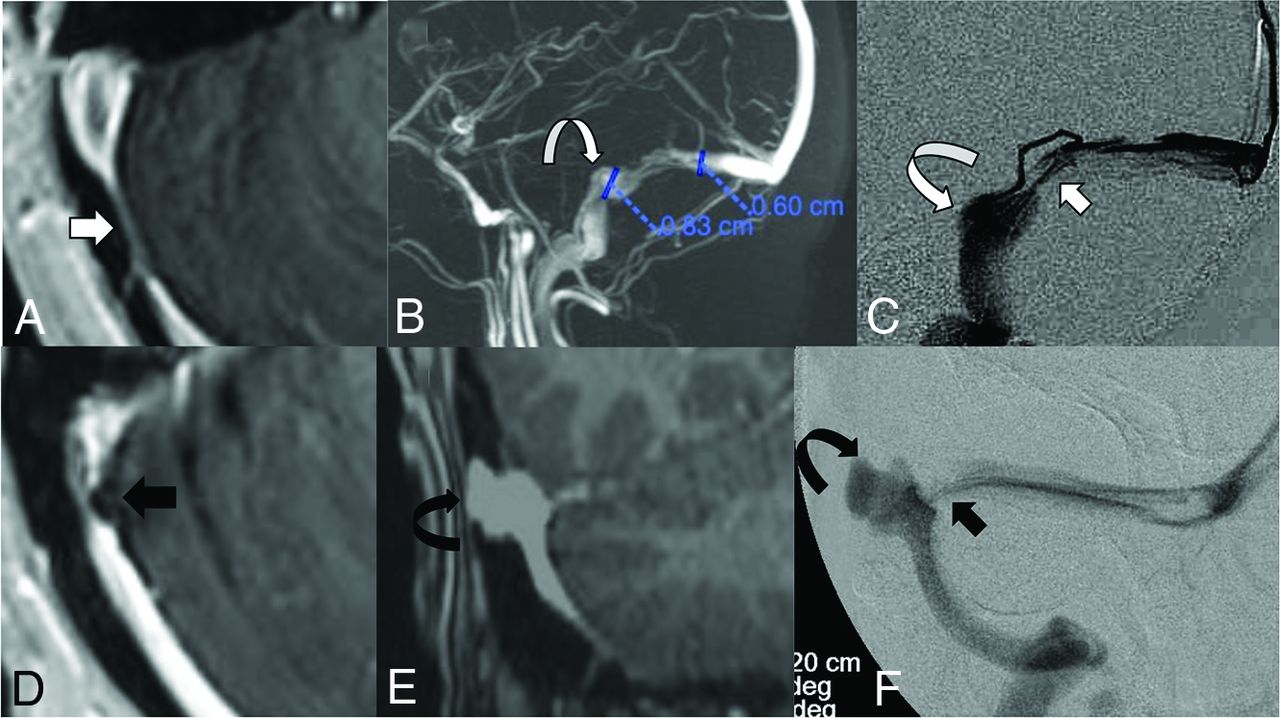
- FIG 1.
A, Axial postcontrast MRV demonstrating extrinsic stenosis from the overlying cerebellum (short white arrow). B, Contrast-enhanced 3D-MRV image shows poststenotic sigmoid sinus enlargement (curved white arrow). C, Accompanying lateral venography confirms stenosis (white arrow) and sinus enlargement (curved white arrow) seen on the corresponding MRV. D, Separate axial postcontrast MRV shows intrinsic stenosis from arachnoid granulations (black arrow). E, A coronal postcontrast MRV sequence shows lateral sinus dehiscence with a venous aneurysm (curved black arrow). F, Accompanying frontal venography confirms stenosis (short black arrow) and a saccular aneurysm (curved black arrow) seen on the corresponding MRV.
- FIG 2.
A, 2-Click automatic vessel analysis start point selection in the sigmoid sinus (short arrow). B, 2-Click automatic vessel analysis end point selection (short arrow) in the superior sagittal sinus (long arrow). C, 3D volume-rendered vessel segmentation. D, Lumen view shows the straightened vessel segmentation.
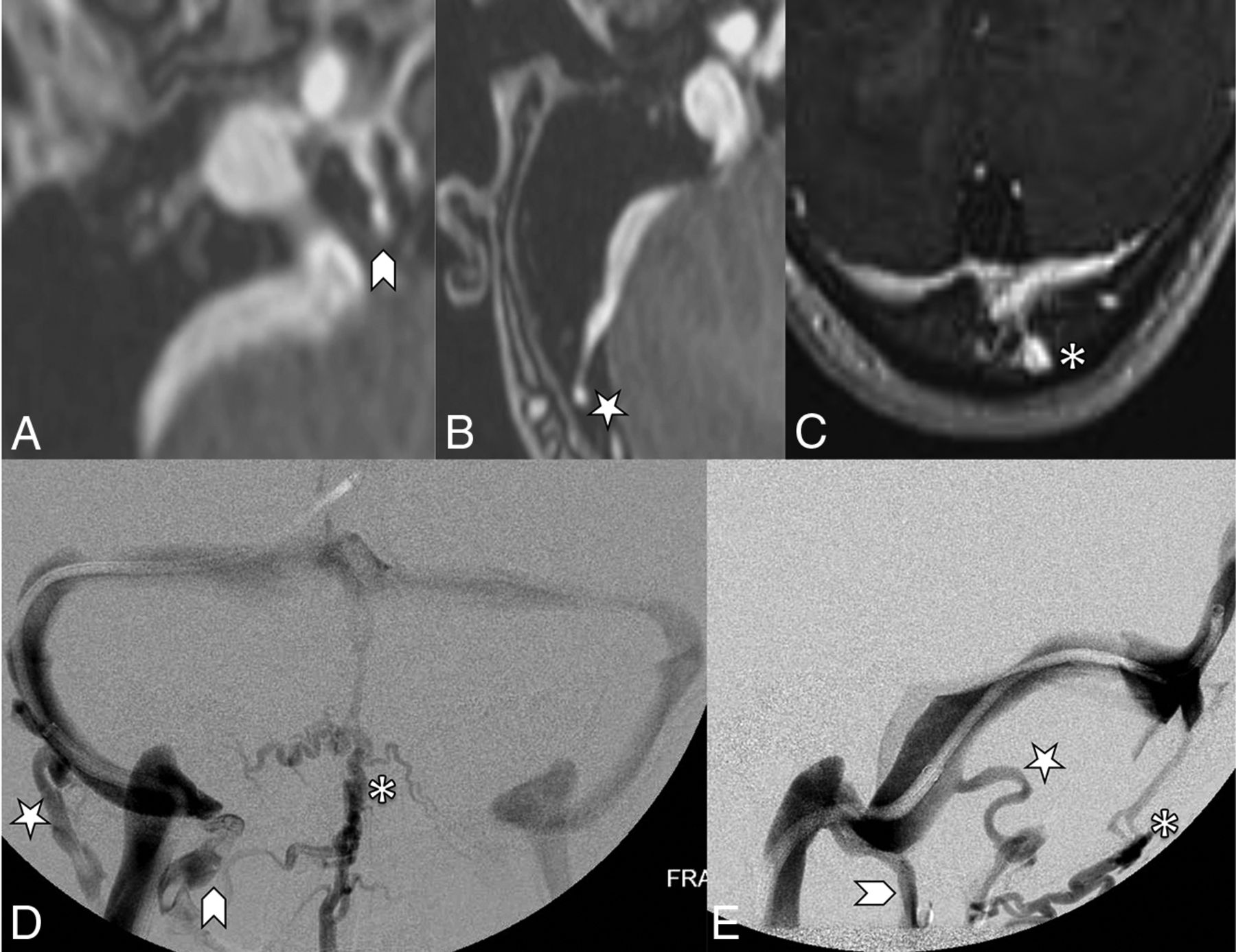
- FIG 3.
Objective parameters implemented in recording corollary findings of both idiopathic intracranial hypertension and pulsatile tinnitus cohorts. A, Marked optic nerve tortuosity, with >50% of optic sheath width deviation noted relative to its expected straight path along the optic canal (white arrows). Bilateral ≥ 5-mm internal jugular bulb diverticula, as seen on MRV (B) and catheter venography (C) images (curved white arrows). D, Cerebellar tonsil projecting 1–3 mm below the foramen magnum, referred to as ectopia (black arrow). E, Empty sella recorded if there is >75% loss of pituitary height (curved black arrow). F, Coronal T2 MR imaging demonstrates a left temporal lobe cephalocele through the tegmen tympani (arrowhead) and CSF in mastoid air cells (star).
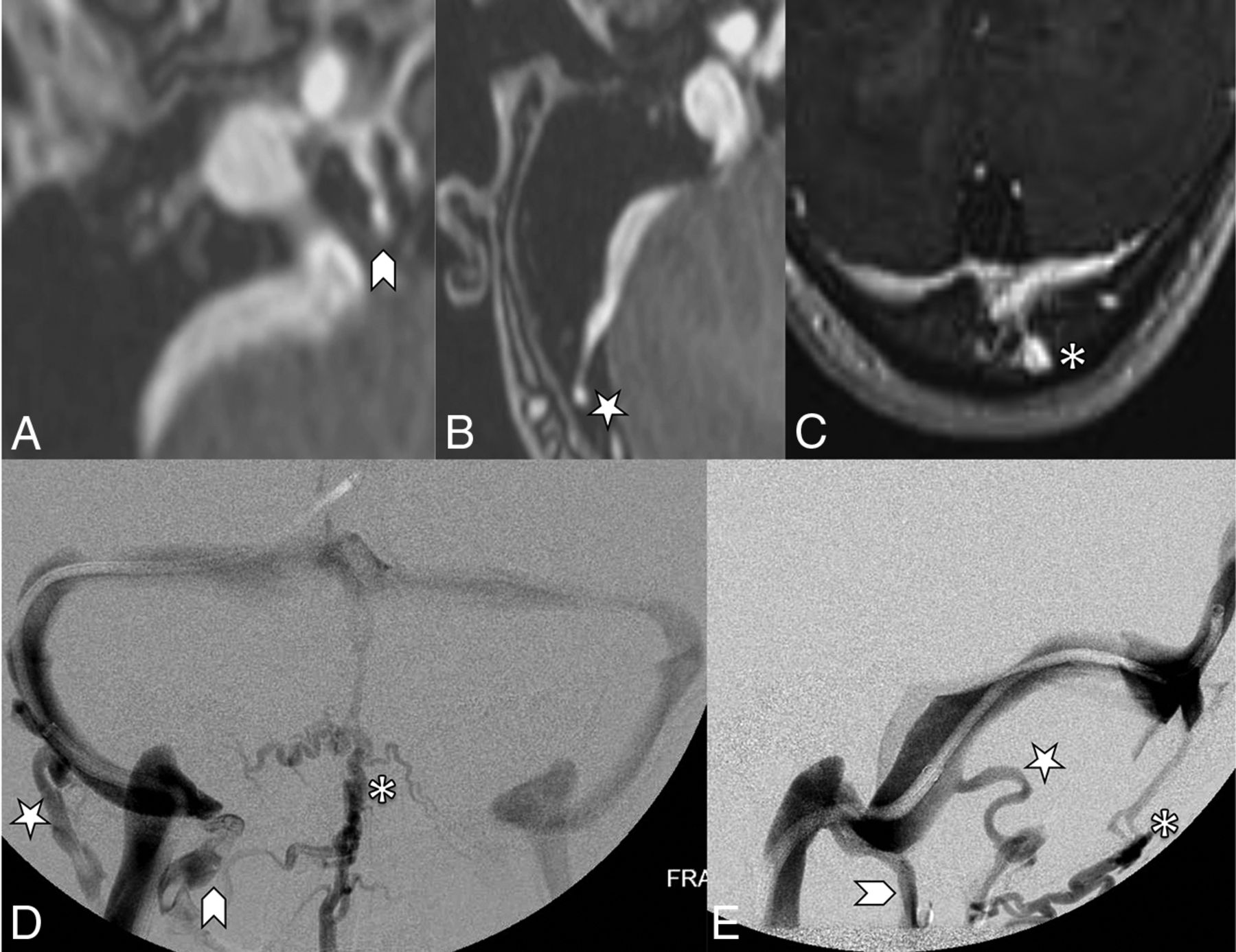
- FIG 4.
Contrast-enhanced MRV images (A, B, and C) highlighting features of the emissary veins categorized in this study. A, A condylar vein is seen arising from the internal jugular vein bulb extending through the condylar canal (arrowhead). B, A mastoid emissary vein is seen arising from the sigmoid sinus traversing the mastoid foramen (star). C, An occipital emissary vein is seen arising from the torcula extending through the calvaria (asterisk). Conventional venography frontal (D) and lateral (E) images showcase the 3 emissary vein types categorized in this study. The condylar vein (arrowhead) extends inferiorly toward the vertebral plexus. The mastoid emissary vein (star) extends posteriorly and inferiorly to join the suboccipital plexus and external jugular vein. The occipital emissary vein (asterisk) drains inferiorly into the suboccipital plexus.
- FIG 5.
MR images showing extrinsic stenosis of the right transverse sinus. The short arrows point to right cerebellar parenchyma location, and the long arrows points to the occipital calvaria location. A, An axial contrast-enhanced MRV image. B, A 3D reconstruction image. C, A straight-vessel reformat of the right transverse-to-proximal sigmoid sinus from source contrast-enhanced axial images.
- FIG 6.
MR images showing intrinsic stenosis of the right transverse sinus. The short arrow points to a prominent arachnoid granulation situated inside the sinus. A, An axial contrast-enhanced MRV image, B, A 3D reconstruction image. C, A straight-vessel reformat of the right transverse-to-proximal sigmoid sinus from source contrast-enhanced axial images, noting orange shading of the arachnoid granulation and transparency of the remaining dural venous sinus.
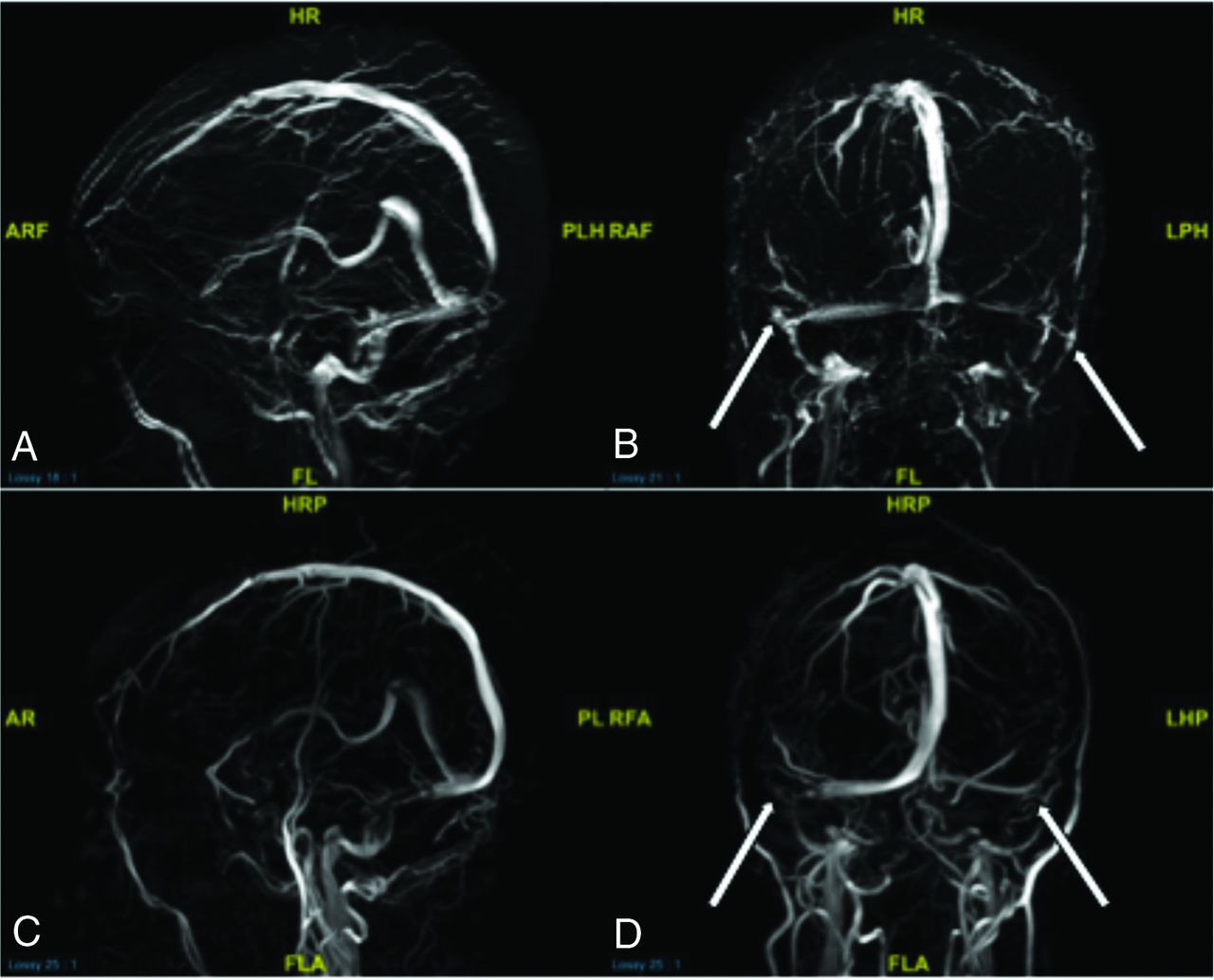
- FIG 7.
Comparing TOF sagittal and coronal 3D reconstructions (A and B) and contrast-enhanced sagittal and coronal 3D reconstructions (C and D) from MRV in a patient with idiopathic intracranial hypertension. Note how the TOF images show the patient’s physiologic venous drainage due to properties of TOF imaging, showing only blood draining back to the patient’s heart (veins). Contrast-enhanced imaging, though crisper, shows arteries and veins in the same image. B and D, Arrows point to severe extrinsic stenoses in the bilateral transverse sinus–sigmoid sinus junctions, a common location for idiopathic intracranial hypertension stenosis. Such short-segment severe stenoses appear to simulate the abrupt narrowing commonly seen in short-segment intrinsic stenoses on these 3D reconstructions. However, review of source imaging would demonstrate brain parenchymal narrowing rather than primary arachnoid granulations producing the stenoses. HRP indicates head right posterior; PLH, posterior left head; RAF, right anterior foot; RA, right anterior; FL, foot left; PL, posterior left; RFA, right foot anterior; LHP, left head posterior; LPH, left posterior head; ARF, anterior right foot; AR, anterior right; FLA, foot left anterior; AF, anterior foot.
- FIG 8.
MR images demonstrating focal intrinsic stenosis just proximal to dominant extrinsic stenosis in this patient with idiopathic intracranial hypertension. The short arrow in A demonstrates focal arachnoid granulation. The long arrows in B and C demonstrate a primary extrinsic stenosis pattern. Despite the mixed presence of intrinsic and extrinsic stenoses, this was categorized as primary extrinsic stenosis. RHA indicates right head anterior; PH, posterior head; LFP, left foot posterior; AF, anterior foot; AR, anterior right; PL, posterior left; H, head; F, foot.






Tables
Demographic Idiopathic Intracranial Hypertension Pulsatile Tinnitus No. of patients 115 43 Age (yr) Mean = 32.8 Mean = 38.1 Min = 4 Min = 20 Max = 66 Max = 67 No. of females 107 (90%) 41 (95%) No. of males 8 (10%) 2 (5%) No. of sinuses: 115 45 sinusesa Right 90 29 Left 25 16 Note:—Min indicates minimum; Max, maximum.
↵a Two patients were stented bilaterally.
- Table 2:
Breakdown of intrinsic and extrinsic stenosis relative to the total number of sinuses and distribution of additional corollary findings noted in the idiopathic intracranial hypertension and pulsatile tinnitus cohortsa
Imaging Finding IIH PT Stenosis type Extrinsic stenosis 58 8 Mixed extrinsic and intrinsic 17 0 Intrinsic stenosis 40 37 Total 115 45 χ² P value ≤ .001b Saccular venous aneurysm Yes 4 11 No 111 34 Total 115 45 χ² P value ≤.001 Sella appearance Partially empty 49 18 Empty 61 15 Normal 5 11 NA (adenoma) 0 1 Total 115 45 χ² P value ≤ .001 Optic nerve tortuosity Minimal 46 31 Marked 69 14 Total 115 45 χ² P value = .001 Note:—NA indicates not applicable; IIH, idiopathic intracranial hypertension; PT, pulsatile tinnitus.
↵a χ2 cross-tabulation P values were calculated for each variable. Eighty-two percent of pulsatile tinnitus sinuses had intrinsic stenosis, and 65% of idiopathic intracranial hypertension sinuses had extrinsic stenosis (P value < .001). Statistically significant differences were noted when comparing the distribution of optic nerve tortuosity, sella appearance, and saccular aneurysm presence between the 2 groups (P values ≤ .001).
↵b Extrinsic and mixed subgroups summed for χ2 calculation.
- Table 3:
Continued breakdown of intrinsic and extrinsic stenosis relative to the total number of sinuses and distribution of additional corollary findings noted in the idiopathic intracranial hypertensin and pulsatile tinnitus cohortsa
Imaging Finding IIH PT Internal jugular bulb diverticulum size <5 mm 47 26 ≥5 mm 68 19 Total 115 45 χ² P value = .053 Cerebellar tonsil location Above 22 11 At 54 23 Ectopia 35 11 Above (prior Chiari I surgery) 4 0 Total 115 45 χ² P value = .522 Cephalocele presence No 110 44 Yes 5 1 Total 115 45 χ² P value = .525 Emissary vein prominence Condylar 52 19 Occipital and condylar 28 11 Mastoid 6 1 Mastoid and condylar 5 3 Occipital, condylar, and mastoid 1 2 None 23 9 Total 115 45 χ² P value = 1 Note:—IIH indicates idiopathic intracranial hypertension; PT, pulsatile tinnitus.
↵a No significant differences were noted when comparing the distribution of internal jugular bulb diverticulum size, cerebellar tonsil location, cephalocele presence, or emissary vein prominence (P values ≥ .053).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Total brain volume is associated with severity of transverse sinus stenosis in idiopathic intracranial hypertension
- Non-invasive imaging modalities for diagnosing pulsatile tinnitus: a comprehensive review and recommended imaging algorithm
- Intravascular ultrasound characteristics of different types of stenosis in idiopathic intracranial hypertension with venous sinus stenosis