
Abstract
BACKGROUND AND PURPOSE: Stent-assisted treatment techniques can be an effective treatment option for intracranial aneurysms. The aim of this study was to evaluate the periprocedural feasibility and safety of the new LVIS EVO stent for the treatment of intracranial aneurysms.
MATERIALS AND METHODS: Patients with intracranial aneurysms treated with the LVIS EVO in 11 European neurovascular centers were retrospectively reviewed. Patient and aneurysm characteristics, procedural parameters, immediate grade of occlusion, and technical and clinical complications were assessed.
RESULTS: Fifty-seven patients with 59 aneurysms were treated with the LVIS EVO device; 57.6% of the aneurysms were incidental; 15.3% were acutely ruptured; 15.3% were recanalized or residual aneurysms; and 11.9% were treated for symptoms other than acute hemorrhage. The most frequent aneurysm locations were the middle cerebral artery (25.4%) and the anterior communicating artery (22.0%). The rate of immediate successful deployment was 93.2%. In 6.8% (n = 4) of cases, additional in-stent angioplasty was needed. The immediate complete occlusion rate was 54.2%, while there was a residual aneurysm in 35.6% and a residual neck in 10.2%. Periprocedural technical complications occurred in 7/59 treatments (11.9%; the most frequent technical complication [n = 3] was thrombus formation), which all resolved completely without clinical sequelae. Postprocedural neurologic complications occurred after 4/59 treatments (6.8%; 2 transient ischemic attacks, 1 minor stroke, 1 major stroke), of which only 1 persistent complication was directly related to the procedure (minor stroke in the vascular territory distal to the stent).
CONCLUSIONS: The LVIS EVO stent is a safe, feasible device for the treatment of intracranial aneurysms.
ABBREVIATIONS:
- ACA
- anterior cerebral artery
- AcomA
- anterior communicating artery
- ASA
- acetylsalicylic acid
- BA
- basilar artery
- DFT
- drawn filled tube
- SAC
- stent-assisted coiling
Stent-assisted coiling (SAC) is a well-established endovascular technique for the treatment of intracranial aneurysms.1⇓⇓-4 Implantation of a stent can have several advantages, such as prevention of coil protrusion into the parent vessel and the ability to increase the coil packing density, ultimately aiming to enhance the safety of the procedure and improve the long-term stability of coil occlusion of intracranial aneurysms.2,5,6 SAC is specifically indicated for wide-neck aneurysms, anatomically complex aneurysms, and aneurysms situated at vessel bifurcations. Various stents with differences in material, composition, and structure are currently available for SAC.4,7⇓⇓-10 The LVIS EVO (MicroVention) is a new stent, specifically designed for SAC, which has recently been introduced to the market. Compared with other braided stents, such as the LVIS Jr (MicroVention), potential differences of the LVIS EVO include enhanced visibility, shorter flared ends, and a smaller cell size. The aim of this study was to investigate the periprocedural feasibility and safety of this new device for the endovascular treatment of intracranial aneurysms.
MATERIALS AND METHODS
Study Design
This work is a retrospective, multicenter, observational study at 11 European neurovascular centers. The clinical and radiologic records of patients with intracranial aneurysms who were treated with the LVIS EVO stent between September 2019 and April 2020 were systematically reviewed on the basis of a dedicated survey that was completed by the interventionalists who had used the device. Institutional ethics committees approved this study.
Patient and Aneurysm Characteristics
The collected patient data included the patient’s age, sex, clinical presentation, and the pretreatment mRS score. For patients presenting with ruptured intracranial aneurysms, the severity of the subarachnoid hemorrhage was assessed according to the Hunt and Hess scale.
The assessed characteristics of the treated aneurysms included aneurysm location, type, size (maximal diameter), neck diameter, the diameter of the parent vessel proximal and distal to the aneurysm, and the degree of angulation of the parent vessel at the site of the aneurysm. Wide-neck aneurysms were defined as aneurysms with a neck diameter of ≥4 mm or a dome-to-neck ratio of <2.
Device Characteristics
The LVIS EVO consists of drawn filled tubes (DFTs) consisting of an inner platinum wire and an outer nitinol wire. The platinum core makes every wire of the device x-ray–visible. Additionally, 4 radiopaque markers are attached to short (0.5 mm) flared ends at each end of the device. The metal coverage of the LVIS EVO ranges from 17% to 28%, depending on factors such as the diameter and the configuration of the deployed stent and the parent vessel. Without packing the stent, the stent cell size ranges from approximately 0.4 to 1.0 mm. The recommended delivery systems are the Headway 17 microcatheter (MicroVention) and the Scepter C or XC dual-lumen balloon catheters (MicroVention).
Two other braided low-profile stents are currently available: the LVIS Jr and the Leo+ Baby (Balt Extrusion). The most important difference in the LVIS EVO to these devices is the material of the stent, which is DFT for the LVIS EVO and nitinol for the LVIS Jr and Leo+ Baby. While every DFT wire is inherently visible, the stent body of the LVIS Jr and the Leo+ Baby is made visible by 3 (LVIS Jr) or 2 (Leo+ Baby) additional tantalum wires. Other special features are the relatively high metal coverage and the small cell size of 0.4–1.0 mm, which is much higher for the LVIS Jr (1.5 mm) and slightly higher for the Leo+ Baby (0.9 mm).
Treatment
The indication for choosing the LVIS EVO, the treatment technique, and the peri-interventional medical treatment were recorded. The ease of deployment and the radiopacity of the device were rated by the treating interventionalist on a 5-point scale: 1, very poor; 2, poor; 3, intermediate; 4, good; 5, very good. Successful deployment was defined as complete opening of the stent without the need for additional techniques such as in-stent angioplasty.
Safety and Feasibility
Periprocedural technical complications were assessed by the neurointerventionalist on fluoroscopy, DSA, and, in some cases, additionally with 3D-DSA and/or flat panel CT. Postprocedural clinical complications until discharge were assessed. Clinical evaluation was performed by a board-certified neuroradiologist, neurosurgeon, or neurologist before the procedure, immediately after the procedure, 24 (±6 hours) after the procedure, and at discharge. The patient’s clinical status was assessed with the mRS. The grade of occlusion immediately after treatment was reported according to the modified Raymond-Roy classification.11
RESULTS
Patient and Aneurysm Characteristics
Fifty-nine aneurysms in 57 patients were treated in 11 European centers between September 2019 and April 2020. Patient and aneurysm characteristics are summarized in Table 1.
Patient and aneurysm characteristics
The patient age was 58.5 [SD, 12.0] years; 73.7% of the patients were female; and 26.3% were male. The pretreatment mRS was 0.6 [SD, 1.2] (mRS 0 in n = 42, 71.2%; mRS 1 in n = 11, 18.6%; mRS 2 in n = 2, 3.4%; mRS 3 in n = 1, 1.7%; and mRS 5 in n = 3, 5.1%). All patients with an mRS of >2 had acute aneurysmal subarachnoid hemorrhage or ischemic stroke. 57.6% of the aneurysms were incidental; and 27.1% were symptomatic (15.3% acute subarachnoid hemorrhage, 3.4% ischemic stroke related to the aneurysm, and 8.5% other symptoms). In 15.3%, the treatment indication was a recanalized or residual aneurysm. For 11.9% of the aneurysms, treatment was indicated because of recanalization after previous coiling; 3.4% were treated because of a residual aneurysm after a previous treatment. The 9 patients with acutely ruptured aneurysms (15.3%) presented with a Hunt and Hess scale score of 1.9 [SD, 1.2].
Most of the aneurysms were located in the MCA (25.4%), followed by the anterior communicating artery (AcomA; 22.0%), the basilar artery (BA; 15.3%), the supraophthalmic ICA (11.9%), and the anterior cerebral artery (ACA; 10.2%). Most aneurysms (93.2%) had a saccular configuration, 5.1% were dissecting aneurysms, and 1.7% were blisterlike aneurysms. The maximal diameter of the treated aneurysms was 6.2 [SD, 3.9] mm, ranging from 1 to 18 mm. Fifty-five aneurysms (93.2%) were wide-neck with a neck diameter of 4.2 [SD, 1.8] mm and a dome-to-neck ratio of 1.5 [SD, 0.7] mm. The diameter of the parent vessel was 2.8 [SD, 0.8] mm proximal to the aneurysm and 2.4 [SD, 0.8] mm distal to the aneurysm. The angulation of the parent vessel at the site of the aneurysm was 102.6° [SD, 44.1°], ranging from 23.0° (sharp angle) to 180° (straight vessel). In 28.8% of the aneurysms, there was a sharp angle of the parent vessel (<90°) at the site of the aneurysm.
Treatment
Treatment characteristics are summarized in Table 2. Example cases are illustrated and described in Figs 1 and 2. The most frequent indication for choosing the LVIS EVO device was a wide aneurysm neck (94.9%). In 2 patients (3.4%), the reason was flow diversion, and in 1 patient (1.7%), the LVIS EVO device was used as a bailout technique after failure of conventional coiling. The ease of deployment was rated as very good in 93.2% and good in 6.8% of cases. Most of the interventionalists rated the radiopacity of the LVIS EVO as good (47.5%) or very good (50.8%).

Stent-assisted coiling of an incidental aneurysm of the AcomA. DSA (A) and 3D reconstructions of rotational angiography (B and C) show a wide-neck aneurysm of the AcomA. After positioning of a microcatheter within the aneurysm (black arrow in D), a 3 × 18 mm LVIS EVO stent was deployed in the A1 and A2 segments of the left ACA (stent ends marked with white arrows). Shouldering of the stent at the base of the aneurysm (black arrowheads) enabled protection of the aneurysmal neck. Subsequently, the aneurysm was coiled (E and F). The shouldered stent enabled complete protection of the parent artery at the aneurysmal neck (black arrows in E) and remodeling of the parent artery. DSAs after treatment (G–I) show complete occlusion of the aneurysm.

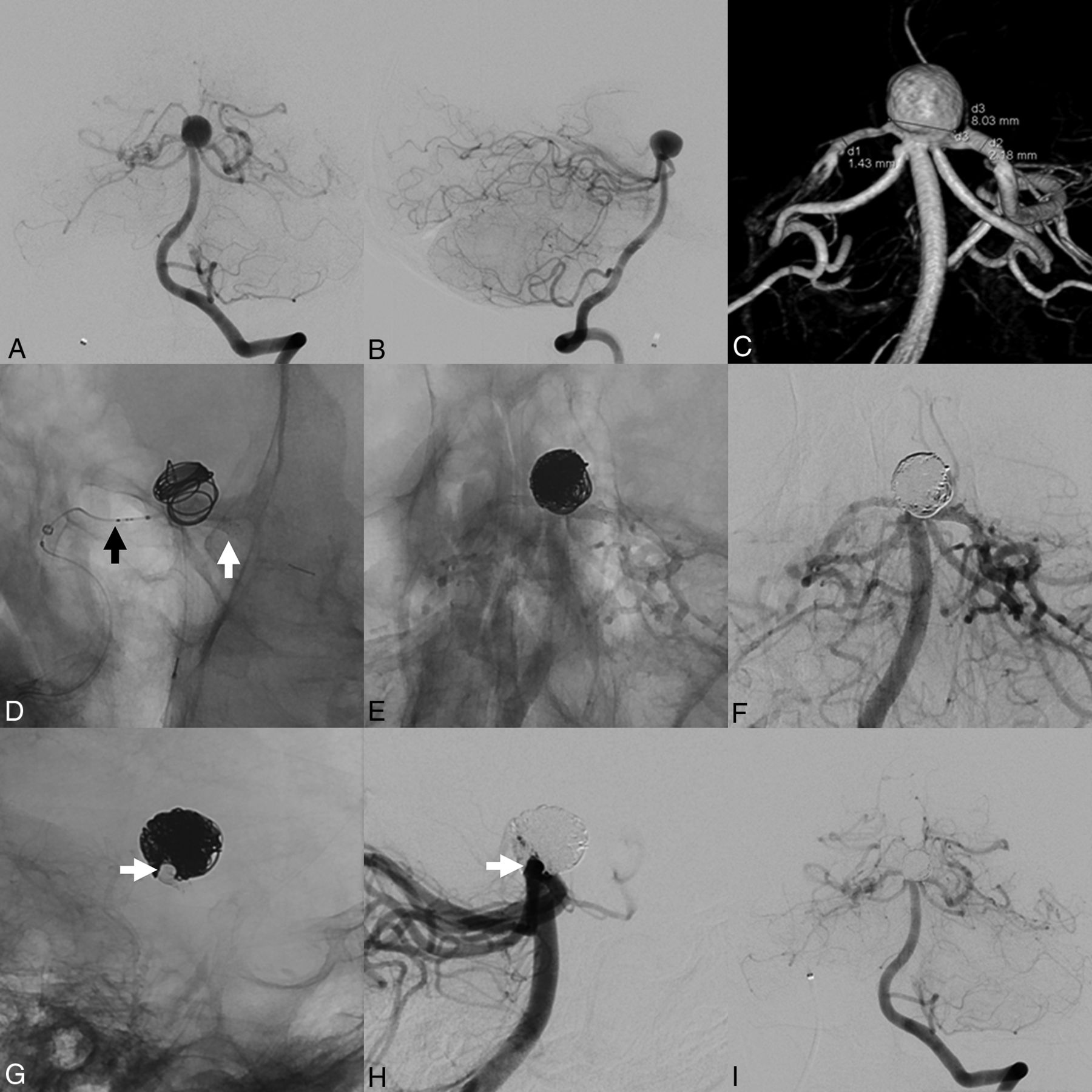
Stent-assisted coiling of an incidental aneurysm of the basilar artery. Digital subtraction angiography (A and B) and 3D reconstructions of rotational angiography (C) show a wide-neck aneurysm of the tip of the basilar artery. After positioning of a microcatheter within the aneurysm, a Headway 17 microcatheter was positioned in the left posterior cerebral artery via the right posterior cerebral artery (black arrow in D), the right posterior communicating artery, and the right ICA. Subsequently, a 2.5 × 17 mm LVIS EVO stent (distal end marked with a white arrow in D) was deployed horizontally over the aneurysmal neck, followed by coiling of the aneurysm (E and F). The stent ensured protection and remodeling of the parent artery (white arrow in G and H). DSAs after treatment (F, H, and I) show complete occlusion of the aneurysm.
Treatment characteristics, safety, and feasibility
Jailing was the predominant treatment technique (88.1%), while the LVIS EVO was used in combination with a Woven EndoBridge device (WEB; MicroVention) in 3 cases (5.1%) and alone without coiling or a WEB in 2 cases (3.4%). In the 3 cases in which a WEB was combined with the LVIS EVO, there was an acute angulation of the aneurysm in relation to the parent vessel, explaining why the WEB was primarily combined with stent implantation. In the 2 cases in which the LVIS EVO device was used alone, the aim was to achieve a flow-diverting effect by the implanted stent. In the first case, coiling with the jailing technique of an aneurysm of the superior cerebellar artery was intended but not possible because a severe stenosis at the entry of the fusiform aneurysm impeded the navigation of a second microcatheter into the aneurysm before implantation of the LVIS EVO. In the second case, treatment of a residual ACA aneurysm was intended after previous SAC using a Neuroform Atlas stent (Stryker Neurovascular). Because jailing of a microcatheter into the residual aneurysm was impeded by the previously implanted stent, the LVIS EVO was used alone. Coiling passing through the stent struts was performed in 2 cases (3.4%). In-stent angioplasty was performed in 4 treatments (6.8%). The reason for in-stent angioplasty was incomplete wall apposition (>75% stent opening) in 3 cases and incomplete opening of the stent (50% stent opening) in 1 case.
Antiplatelet Therapy
The most frequently administered preinterventional therapy was acetylsalicylic acid (ASA) in combination with clopidogrel (79.7%), followed by ASA combined with ticagrelor (11.9%). In 5 patients with ruptured aneurysms (8.5%), no preinterventional antiplatelet therapy was used. Peri-interventional glycoprotein IIb/IIIa antagonists (tirofiban or abciximab) were given in 13.6% of the cases. Postinterventional antiplatelet therapy consisted of ASA combined with ticagrelor in 45.8%, ASA combined with clopidogrel in 42.4%, ASA combined with prasugrel in 6.8%, and cilostazol combined with clopidogrel in 3.4% of cases. Platelet function testing was performed in 43 patients (72.9%).
Safety and Feasibility
Safety and feasibility parameters are summarized in Table 2.
The LVIS EVO stent could be successfully deployed in 55 of 59 treatment procedures (93.2%). As stated above, in-stent angioplasty was needed in the remaining 4 cases without immediate complete stent opening. The total number of periprocedural technical complications was 7 (11.9%), 2 of which occurred during the treatment of acutely ruptured aneurysms. All except 1 of these technical complications were directly related to the LVIS EVO and included thrombus formation within the stent lumen in 3 cases as well as coil protrusion into the parent vessel, shortening of the stent, and insufficient stent opening in 1 case each.
Unsuccessful stent deployment occurred during the treatment of an aneurysm of the ICA. The proximal stent only opened incompletely (50% of the vessel lumen), which was most probably related to a 180° curve of the vessel at the site of the proximal stent. Navigation with a balloon catheter into the stent and following in-stent angioplasty caused slight compression of the proximal half of the stent without any flow disruption.
Thrombus formation occurred during the treatment of aneurysms of the MCA (unruptured), AcomA (ruptured), and ICA (ruptured), respectively, and was successfully treated by intravenous abciximab infusion, which led to complete resolution of the thrombus. In one of these cases (an MCA aneurysm), thrombus formation was observed in a second stent (Neuroform Atlas), which was positioned in an MCA M2 branch for Y-stent placement. The thrombosis in this second stent might have resulted from the interaction of the 2 stents (constraining full opening of the second stent and/or increased metal density within the vessel). This patient received ASA in combination with clopidogrel before the treatment, both of which showed an adequate effect in the preinterventional platelet function test. The 2 patients with ruptured aneurysms and periprocedural in-stent thrombosis received periprocedural intravenous abciximab and heparin.
Coil protrusion occurred in an aneurysm of the AcomA in the direction of the nonstented A2 segment and was successfully treated by stent placement (Acclino flex; Acandis) in the contralateral ACA. Slight stent shortening occurred during modeling of an 18 × 4 mm LVIS EVO with a 6 × 9 mm Eclipse 2L balloon (Balt Extrusion). A technical complication that was not directly related to the LVIS EVO consisted of coil dislocation, which did not lead to any angiographic or clinical consequences. All of these technical complications resolved without clinical sequelae. In 1 case, full opening of the stent was reported to occur only after removing the jailed microcatheter, which we did not classify as a technical complication.
In 4 patients (6.8%), neurologic complications were reported before hospital discharge. Of these complications, 2 were transient (TIAs) and 2 were permanent (minor and major stroke), while 1 occurred after the treatment of a ruptured aneurysm (major stroke) and 3 occurred after the treatment of unruptured aneurysms. Two neurologic complications were directly related to the LVIS EVO: 1 minor stroke in the vascular territory distal to the stent and 1 TIA. Both of these complications occurred after the treatment of unruptured aneurysms in patients who received pre- and postinterventional antiplatelet therapy using ASA and clopidogrel with positive antiplatelet function test results. The neurologic complications, which were persistent until discharge, included a major stroke not restricted to the territory of the stented artery due to vasospasms in a patient with a ruptured ICA aneurysm, and the above-mentioned minor stroke in the territory of the stented artery, which became clinically apparent as dizziness. Both of these ischemic strokes led to an increase in the mRS score (2–5 for the major stroke and 1–2 for the minor stroke). Apart from these 2 complications, no increase in mRS scores was observed when comparing the preinterventional mRS and the mRS at discharge. Two patients (3.4%) had transient postprocedural headache, which was not classified as a clinical complication.
Postprocedural non-neurologic complications occurred in 3 patients (5.1%) and included upper gastrointestinal bleeding, puncture site bleeding, and acute ischemia of the leg contralateral to the puncture site in a patient with known peripheral arterial occlusive disease.
Immediately after the treatment, “complete occlusion” was observed in 54.2%; “residual neck,” in 10.2%; “residual aneurysm with contrast within coil interstices,” in 30.5%; and “residual aneurysm with contrast along the aneurysm wall,” in 5.1%.
DISCUSSION
This multicenter study, reporting the experience of 11 European neurovascular centers, demonstrates acceptable periprocedural safety and feasibility of the new LVIS EVO stent for the treatment of intracranial aneurysms.
Endovascular treatment has become the first-line therapy for most intracranial aneurysms.12 For aneurysms with a wide neck, aneurysms with complex anatomy, or aneurysms situated at vessel bifurcations, it was shown that SAC provides better occlusion rates and anatomic results, compared with coiling only or balloon remodeling.1,2 The advantages of this treatment technique include the possibility of increasing the density of coil packing, the impediment of coil protrusion into the parent artery, the forming of a scaffold for endothelialization, and the generation of a flow-diverting effect past the aneurysm.1,2,13,14 All these factors ultimately aim to improve the immediate and long-term occlusion rates of ruptured and unruptured intracranial aneurysms and to enhance the safety of the treatment procedure.
For the new LVIS EVO stent, as initially indicated, the major innovation is the structure of the wires of the stent. While established braided stents, such as the Leo+ and Leo+ Baby or the LVIS and LVIS Jr, predominantly consist of pure nitinol wires, the LVIS EVO consists of DFT wires with a platinum core and an outer nitinol coating. In addition to these structural differences, the wires of the LVIS EVO are arranged in a specific braiding pattern, which is based on the specific behavior of the DFT wires. These technical features aim to improve the visibility and enhance the opening ability and formability of the stent. The results of this study are in line with these promoted features. In all except one of the treatments (98.2%), the visibility of the device was rated as good or very good. The LVIS EVO stent was deployed successfully in most of the treatment procedures, while the ease of deployment was rated as good in 6.8% and very good in 93.2% of the cases.
The metal coverage of the LVIS EVO device, which depends on the size of the implanted stent and its configuration within the parent vessel, is relatively high and can range up to 28%. This maximum metal coverage is equal to the minimum metal coverage of the Flow-Redirection Endoluminal Device (FRED Jr; MicroVention) stent, which features a metal coverage ranging from 28% to 33%.15 Accordingly, it is likely that the LVIS EVO stent also offers a certain flow-diverting effect. In this study, the LVIS EVO was used for flow diversion in 2 cases (without additional coiling). In both cases, stasis within the aneurysm but not complete occlusion was observed immediately after the procedure. Mid- and long-term follow-up data are needed to assess the value of the flow-diverting effects of the LVIS EVO stent.
Compared with other braided stents, the LVIS EVO has a relatively small cell size. This smaller cell size can be a disadvantage because it may impede passing through the stent with a microwire/microcatheter for coiling. Therefore, we recommend jailing as the first-line treatment technique with the LVIS EVO. However, crossing the stent with a microcatheter is also possible, while its ease depends on the anatomy, the outer diameter of the stent, and the degree of stent packing. Nevertheless, the small cell size might impede crossing-stent techniques, such as Y- and X-stent placement. In such cases, T-stent placement could be an alternative treatment option.
Despite these very positive results, no statement with regard to the superiority of the LVIS EVO stent over other stents can be made on the basis of this study because we only investigated the periprocedural results of the LVIS EVO without comparison with any other device. However, the high rate of technical feasibility is similar to that in other comparable devices, such as the Leo+ Baby, LVIS, LVIS Jr, Neuroform Atlas, or Acclino stents.4,8,16⇓-18
In this study, periprocedural technical complications occurred in 11.9% of treatments. However, all of these technical complications resolved without clinical sequelae. The rate of neurologic complications until discharge was 6.8%, of which only 2 complications were directly related to the LVIS EVO stent (1 minor ischemic stroke in the vascular territory of the stented artery and 1 TIA). One major stroke, which was unrelated to the procedure, was observed. The low rate of symptomatic and persistent complications in this study is in line with results reported in the literature.2,4
The rate of immediate aneurysm occlusion in this study was 54.2%, which is in accordance with immediate occlusion results after SAC reported in the literature.19,20 A systematic review and meta-analysis by Hong et al20 reported an immediate occlusion rate of 57.6%. A substantial angiographic improvement in occlusion during follow-up can be expected after SAC.1,20,21
We acknowledge that this study has some noteworthy limitations. Because this is a retrospective, observational study based on a dedicated survey, which was completed by the interventionalists themselves, without additional data analysis by a core lab, there is inherent selection and reporting bias associated with it. The number of patients and aneurysms in this study is relatively small, the data are quite heterogeneous, and a control group is lacking. However, this is a multicenter study and, to our knowledge, it is the only study reporting on the clinical use of the LVIS EVO stent to date. No follow-up data are available for this study yet. To assess the effectiveness of this device in particular, long-term follow-up data are necessary. However, the focus of this study was the periprocedural safety and feasibility of the LVIS EVO device. Furthermore, this device was introduced only recently, and accordingly, to the best of our knowledge, comprehensive follow-up results are not yet available.
CONCLUSIONS
The LVIS EVO stent is a safe and feasible device for the treatment of intracranial aneurysms. Further studies are needed to assess the mid- and long-term effectiveness as well as potential advantages of this new device over other available stents.
Footnotes
Disclosures: Dominik F. Vollherbst—UNRELATED: Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: MicroVention and Stryker Neurovascular, Comments: travel support.* Ansgar Berlis—RELATED: Consulting Fee or Honorarium: proctor for MicroVention; UNRELATED: Consultancy: proctor for Stryker Neurovascular and Medtronic; Payment for Lectures Including Service on Speakers Bureaus: Penumbra; Other: Clinical ethics comittee for phenox. Christoph Maurer—UNRELATED: Grants/Grants Pending: MicroVention, Comments: educational grant. Sebastian Fischer—UNRELATED: Consultancy: MicroVention, Comments: proctoring and consultancy agreement; Payment for Lectures Including Service on Speakers Bureaus: MicroVention. Markus Holtmannspötter—UNRELATED: Consultancy: MicroVention, Medtronic, Stryker Neurovascular, phenox, Mentice, Rapid Medical, Comments: proctoring and consulting. Riitta Rautio—UNRELATED: Consultancy: Stryker Neurovascular, MicroVention, Medtronic. Wojciech Poncyljusz—UNRELATED: Consultancy: proctoring for MicroVention. Fritz Wodarg—UNRELATED: Consultancy: MicroVention, Cerus Endovascular, Acandis; Payment for Lectures Including Service on Speakers Bureaus: MicroVention, Cerus Endovascular, Acandis; Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: MicroVention, Cerus Endovascular, Acandis, Stryker Neurovascular. Christoph Kabbasch—UNRELATED: Consultancy: proctor for MicroVention, consultant for Acandis. Johannes Trenkler—RELATED: Support for Travel to Meetings for the Study or Other Purposes: MicroVention. Markus A. Möehlenbruch—UNRELATED: Consultancy: Medtronic, MicroVention, Stryker Neurovascular, phenox*; Grants/Grants Pending: Balt, MicroVention*; Payment for Lectures Including Service on Speakers Bureaus: Medtronic, MicroVention, Stryker Neurovascular.* Martin Bendszus—UNRELATED: Board Membership: Vascular Dynamics, B. Braun Medical, Boehringer Ingelheim Pharma; Consultancy: Guerbet; Grants/Grants Pending: European Union, German Research Foundation, Hopp Foundation, Siemens, Novartis, Stryker Neurovascular*; Payment for Lectures Including Service on Speakers Bureaus: Merck, Teva Pharmaceutical Industries, Novartis, Bayer AG, Grifols. Christian Herweh—UNRELATED: Consultancy: Brainomix. *Money paid to the institution.
References
- Received May 13, 2020.
- Accepted after revision September 7, 2020.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Multicenter early United States feasibility study and periprocedural safety of LVIS EVO for the treatment of unruptured intracranial aneurysms
- Safety, Efficacy, and Durability of Stent-Assisted Coiling Treatment of M2 (Insular) Segment MCA Aneurysms
- How much safety is actually 'safe? Commentary on 'Safety of the Apollo Onyx delivery microcatheter for embolization of brain arteriovenous malformations: results from a prospective post-market study by Meyers et al