
Abstract
BACKGROUND AND PURPOSE: The developing nervous system is particularly vulnerable to late adverse effects of cranial radiation therapy, such as leukoencephalopathy, microbleeds, and cavernomas. Cystlike lesions have been rarely described and characterized in the literature. We aimed to characterize cystlike lesions, their risk factors, and association with other late adverse effects.
MATERIALS AND METHODS: Children treated for brain tumors during a 30-year period (n = 139) were included. We documented imaging findings, focusing on cystlike lesion development and its relationship with clinical history and other imaging findings. Multivariable analysis was performed using logistic regression and negative binomial regression models.
RESULTS: Cystlike lesions developed in 16.5% of patients treated with radiotherapy, with a median of 2 years until the development of the first lesion. For every 4-year age increase, there were 50% decreased odds of developing lesions and a 50% decrease in the average count of lesions. Females demonstrated a 4.00 rate ratio of developing a higher number of lesions. Patients who underwent chemoradiotherapy had 3.20 increased odds of developing cystlike lesions compared with patients with radiation therapy alone. A larger proportion of patients treated with methotrexate (25%) developed cystlike lesions, but this was not statistically significant. Cystlike lesions tended to develop in cerebral locations where leukoencephalopathy was worse. A strong relationship was found between the development of cystlike lesions and leukoencephalopathy severity.
CONCLUSIONS: Cystlike lesions are frequent and under-reported late adverse effects of cranial radiation therapy in children. Younger age, chemoradiotherapy, and the severity of leukoencephalopathy represent risk factors for the development of cystlike lesions.
ABBREVIATIONS:
- CLL
- cystlike lesions
- LE
- leukoencephalopathy
- MTX
- methotrexate
- RT
- radiotherapy
Central nervous system tumors are the most common solid tumors in children, accounting for up to 22% of tumors in patients between 0 and 14 years of age.1 The 5-year relative cancer survival rate in these patients has been increasing in the past decades.2 Childhood cancer therapy causes chronic health problems in almost 75% of survivors, which can become clinically visible several years after treatment and are frequently irreversible and progressive.1
Late adverse effects are related to chemotherapy, radiation therapy (RT), or a combination of both.1,3,4 These adverse effects of treatment are additive, with a higher disease burden in patients who had more aggressive therapies or were younger at diagnosis.5,6 The developing nervous system of young children is particularly vulnerable to cancer treatment, especially to the effects of radiation.4,7,8 One of the chemotherapy agents with more significant CNS adverse effects is methotrexate (MTX). Concomitant brain radiation and young age represent risk factors for MTX-associated adverse effects.3,4
Neuroimaging abnormalities after chemotherapy, RT, or multimodal therapy are described in several studies, ranging from the common leukoencephalopathy (LE), microbleeds, and cavernomas to the rarely described cystlike lesions (CLL).4,8 In fact, only 3 cohort studies describe these lesions.9⇓-11 This study aimed to characterize the risk factors and associations of CLL with other late adverse effects.
MATERIALS AND METHODS
Sample Characteristics
Between January 1990 and June 2020, one hundred seventy-five children with brain tumors were treated with cranial RT at Instituto Português de Oncologia de Lisboa Francisco Gentil, Lisbon, Portugal. Most patients underwent multimodality treatment with different therapy regimens, including surgery, chemotherapy, and RT.
According to previous studies, only pediatric patients treated with cranial RT develop CLL, with a median time from cranial RT to imaging findings of 2 years (range, 0.26–5.7 years); thus, a minimum of 5 years of follow-up was considered adequate. 9⇓-11
The inclusion criteria for case enrollment in this retrospective cohort study were cranial RT, 17 years of age or younger at the time of cranial RT, and a minimum of 5 years of follow-up after cranial RT with serial MR imaging. Thirty-six patients without a minimum of 5 years of follow-up were excluded. This retrospective study was approved by the institution's ethics committee.
Data Collection
All patients were regularly followed in a dedicated outpatient consultation. The clinical files from neuro-oncology, radiation therapy, and pediatrics were reviewed. The pertinent clinical data were retrieved from patients' clinical charts, including demographic information (age, age at cranial RT, sex), tumor characteristics (location, histology), and treatment (treatment protocol, RT technique and total dose [Gy], and the chemotherapy regimen).
MR Imaging Evaluation
Patients underwent MR imaging at the time of diagnosis and during routine follow-up examinations. By protocol, after treatment completion, the patients underwent sequential MR imaging studies with 6-month intervals during the first 4 years and every year after that. MR imaging protocols included the following sequences: T2WI, FLAIR, DWI, and T1WI after gadolinium administration. Most of the performed examinations also included an iron-sensitive sequence, eg, T2* and SWI.
Neuroimaging studies of these patients were retrospectively reviewed for the presence of cystlike lesions, leukoencephalopathy, microbleeds, and cavernomas. All the examinations were previously reported by staff radiologists trained in neuroradiology, with a mean of 20 years of experience in neuro-oncology imaging. A neuroradiologist (with 4 years of experience) blinded to the clinical status and imaging report reviewed all the examinations twice. Discrepancies between the 2 observers were reviewed for consensus.
CLL (Fig 1) were defined as cystlike cavities of the cerebrum white matter with MR signal equal to that of CSF in all sequences, without enhancement after gadolinium, at any time of follow-up (Fig 2). All the observed cysts had a minimum distance of 1 cm from the tumor site or surgical bed. The number, size, and distribution of the WM cysts were recorded in each examination.

Patient 10 was treated for medulloblastoma (A–C) (T2WI, T2 FLAIR, T1WI after gadolinium administration). D–L, Three T2WIs, T2 FLAIR, DWI/ADC map, T1WI, T1WI after gadolinium, and SWI, all obtained 7 years after treatment. The patient underwent whole-brain RT; consequently, CLL developed diffusely in both cerebral hemispheres (D–F). CLL (black arrows) are cystlike cavities of the cerebrum white matter with MR signal equal to that of CSF on all sequences, which frequently develop in proximity to LE (white arrows), represented by T2 and T1 prolongation of white matter signal.

Patient 24 underwent all the MR imaging examinations of the protocol. Pretreatment images are shown in the first row, depicting a frontotemporal anaplastic ependymoma (T2 FLAIR and T1WI after gadolinium) and the corona radiata (T2WI). CLL developed between 3 and 4 years of follow-up. CLL (black arrows) mainly evolved from previous LE, represented by noncystic white matter lesions, with T2 and T1 prolongation, without gadolinium enhancement (white arrows). Only the right cerebral hemisphere was irradiated; consequently, the left cerebral hemisphere was spared from LE and CLL.
LE was classified according to the Fazekas scale on the basis of the distribution and size of white matter T2WI hyperintensities, as previously described in the study by Yamasaki et al11 (Fig 3A–C).12
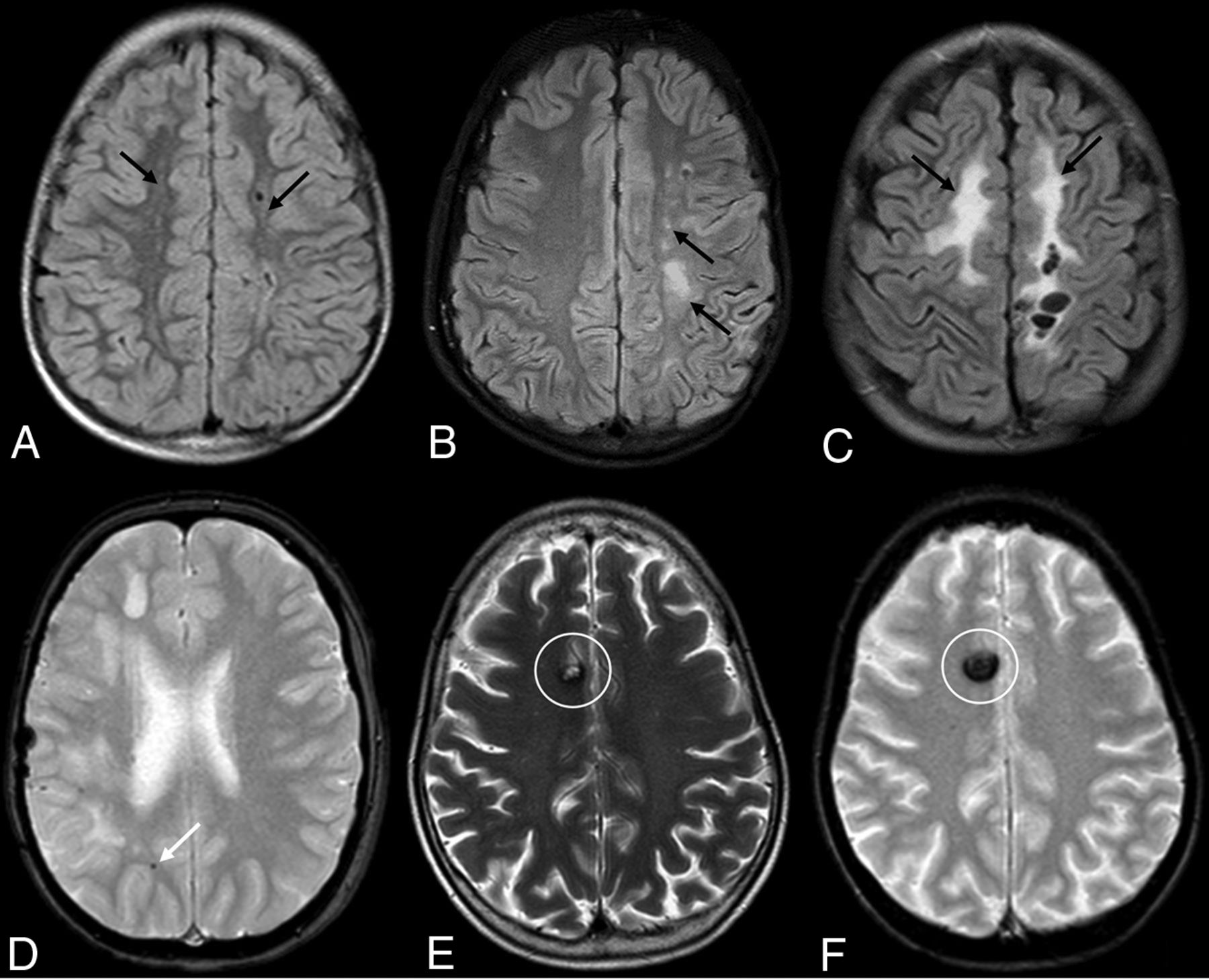
A, Patient 42. LE (Fazekas grade 1) is shown, with punctate white matter T2-hyperintense lesions (black arrows). B, Patient 43. LE (Fazekas grade 2), with a slight confluence of T2-hyperintense lesions of the white matter (black arrows). C, Patient 26. LE (Fazekas grade 3), with large confluent areas of white matter T2 hyperintensities (black arrows). D, Patient 24. Small cerebral microbleeds, with a T2* blooming black dot (white arrow), not visible on T2WI. E and F, Patient 107 demonstrates a cavernoma with a classic “popcorn” appearance on T2WI and a large hypointensity on T2* with blooming (white circles).
Microbleeds were defined by small, round or ovoid, well-defined hypointense lesions on T2* and SWI, not seen on T1WI and T2WI, with a maximum diameter of 3 mm (Fig 3D). The potential mimickers (calcium deposits, vessel flow void, and traumatic brain injury) were excluded by imaging or clinical history.5,13 All lesions within a 1-cm margin of the surgical resection site were excluded.
Cavernomas were defined as all T2* and SWI hypointense lesions with signal changes in T1WI and/or T2WI that could be categorized using the Zabramski classification as type I, II, or III (Figs 3E, -F).14
Statistical Analysis
Categoric data are presented as frequencies and percentages, and quantitative variables, as median and range (minimum-maximum). Groups of patients (with and without CLL) were compared using χ2 or Fisher exact tests for categoric variables (sex, tumor location and histology, treatment protocol, chemotherapy regimen, and RT technique) and Mann-Whitney tests for quantitative variables (age at cranial RT and RT total dose).
Hurdle models were used to identify factors associated with CLL development and associated with the number of cystlike lesions, such as sex, tumor histology, tumor location, age during radiation therapy, treatment protocol, radiation therapy technique and dose (Gy), and chemotherapy agents. All variables that attained a P value of ≤.25 were considered for the multivariable analysis. The hurdle model is a 2-component model useful when there is an excess of zeroes, as is the case in our study in which many of the children did not have CLL. The first part (hurdle model) is a logistic regression model, and it is used to estimate the odds of developing CLL through the estimation of the OR, while the second part (count model) is a negative binomial regression model, which is used to estimate rate ratios regarding the number of cysts.
A level of significance α = .05 was considered. The analysis was performed using R statistical and computing software (http://www.r-project.org/).
RESULTS
Patient Characteristics
Table 1 summarizes baseline demographic and clinical data by groups of patients (with and without CLL). A total of 139 patients met the inclusion criteria, 82 (59.0%) of whom were male. Patients' ages at the time of cranial RT varied between 0 and 17 years, with a median of 8 years.
Demographic, clinical, and imaging characteristics of the studied sample with CLL compared with those without CLL
Medulloblastomas (37.4%), ependymomas (15.8%), and germinal cell tumors (13.7%) were the most represented tumors. Eighty (57.6%) tumors were infratentorial.
Concerning the RT technique, 72 (51.8%) patients were treated with combined whole-brain RT and focal RT, 64 (46.0%) were treated with isolated focal RT, and 3 (2.2%), with isolated whole-brain RT. Twenty-nine (20.9%) patients underwent chemoradiotherapy (chemotherapy-RT).
Ninety-eight patients (70.5%) underwent chemotherapy. Only 8 patients (5.8%) had MTX included in their chemotherapy regimen. The RT median total dose was similar in both subgroups, but the CLL group's minimum dose was 50 Gy.
Twenty-three (16.5%) individuals of the sample of 139 patients developed CLL. The median time to the first appearance of CLLs after radiation therapy was 2 years (mean, 2.1 [SD, 0.64] years; minimum, 1 year; maximum, 3.5 years). Seventeen of 23 patients (73.9%) had >1 cystlike lesion, with a median of 4 per patient (minimum, 2; maximum, 45). No CLLs were observed in the infratentorial compartment or outside the radiation field (Fig 2).
Fifty-eight (41.7%) patients developed LE, while 88 (63.3%) patients developed microbleeds and 53 (38.1%) developed cavernomas. A significantly higher proportion of patients developed CLL, depending on the severity of LE (according to the Fazekas scale). These data are summarized in Table 2. The development of CLLs was not related to acute or subacute clinical manifestations.
Posttreatment imaging characterization of the studied sample comparing patients with and without CLL
Risk Factors Associated with the Development of Cystlike Lesions
Regarding risk factors for the development of CLL, results of the univariable study depicted in Table 1 showed that a statistically significant association was found with chemotherapy-RT (P = .027) and younger age (P = .004). One-third (31%) of the patients who underwent chemotherapy-RT developed CLL, compared with 12.8% of patients with a single therapy. Younger patients demonstrated higher susceptibility when considering CLL prevalence in age groups with 4-year gaps (Table 3). Histology was also associated with development of CLL (P = .044).
Prevalence of CLL in age groups (4-year gap)
Both variables (age, chemotherapy-RT) remained significant in the multivariable analysis (Table 4). Children exposed to chemotherapy-RT had increased odds of 3.20 of developing CLL compared with those not exposed to chemotherapy-RT (P = .024; 95% CI, 1.17–8.75). It was also demonstrated that for each 4-year increase in a child's growth, there was a 49% decrease in the odds of developing CLL (OR = 0.51; P = .015; 95% CI, 0.30–0.88). The remaining factors, such as sex (P = .841), tumor location (P = .725), chemotherapy regimen (P = .584), and RT total dose (P = .294), were not found to be associated with CLL (Table 1).
Results of the multivariable regression model for CLLa
Among those who had positive counts, the CLL average count was 1.61. The number of lesions decreased by 0.5 times (95% CI, 0.27–0.97; P = .041) for each 4-year age increase, and it was increased 4 times in females (95% CI, 1.53–10.41; P = .005).
Associated RT Late Adverse Effects
A strong association was found between the development of CLL and LE (P < .001), but no significant association was found with microbleeds or cavernomas (Table 2). However, 52.2% of patients with CLL developed cavernomas, and only 35.3% of patients without CLL had cavernomas. A strong relationship was also found between the development of CLL and the severity of LE, measured by the Fazekas scale (P = .001).
DISCUSSION
Most scientific literature has classically described children's radiation therapy brain toxicity as a replication of the adult toxicity, but with increased incidence and/or severity of the adverse effects.3,15 The vulnerability of developing tissues to radiation determines a range of adverse events in children, different from those seen in the adult population.16
The reviews of neuroimaging findings in pediatric cancer survivors include brain volume loss, leukoencephalopathy, mineralizing microangiopathy, microbleeds, and cavernomas.1,3,15 However, in previous literature reviews, CLL9⇓-11 have not been mentioned as RT adverse effects in the pediatric brain.1,3,15
To the present date, only 3 studies have been published relating to these types of late-induced lesions from radiation therapy.9⇓-11 The first, the only one in the Western population, was published in 2000 and included the largest number of patients.9 The last 2 articles, published in 2007 and 2017, were based on much smaller populations from Japan (33 and 41 patients, respectively).10,11 The 3 studies attributed different names to these lesions: silent lacunar lesions, cystic malacia, and asymptomatic cystic lesions.9⇓-11 Because no histology was obtained in any of the studies and the nature of the lesions is unknown, we opted to name them cystlike lesions, which represent the imaging phenotype. To our best knowledge, our study is the second with >100 patients in a Western population.
Characterization of CLL and Risk Factors
The percentage of patients who developed CLL (16.5%) is similar to that reported by Kitajima et al10 (18%) but is considerably higher than that of Fouladi et al9 (6%). This latter study included the use of CT, which might have contributed to decreased sensitivity. Similar to the results of previous studies, CLL appeared a median of 2 years after cranial RT.9⇓-11 This finding supports the evidence that these lesions develop only in the first years after cranial RT.
As previously described in the literature, late adverse effects of cranial RT depend on several factors, such as patient age, radiation dose, type of irradiation, and concomitant antineoplastic or radiosensitizing agents.3 Our analysis demonstrated that for each 4-year age increase, there are 50% decreased odds of developing CLL and a 50% decrease in the average lesion count. In line with previous studies, this finding suggests that increasing age has an attenuating effect on disease burden.
We hypothesized that the RT dose could be a risk factor; however, the significant overlap of radiation doses between the subgroups, namely in patients subject to ≥50 Gy, precluded a statistically significant result. However, none of the patients irradiated with <50 Gy developed CLL, which appears to be a cutoff value below which patients tend to not develop CLL.
Given the neurotoxicity of MTX, we also hypothesized that it could represent an independent risk factor.3,4,10 In fact, a larger proportion of patients treated with MTX (25%) developed CLL, compared with the patients who underwent chemotherapy without MTX (18%) and the ones treated without any chemotherapy (12%). These results suggest that chemotherapy could be a risk factor, eventually aggravated by the inclusion of MTX. However, the small number of patients treated with MTX limits the statistical significance of the results.
The patients who underwent chemotherapy-RT had 3.20 increased odds of developing CLL, showing that concomitant chemotherapy also acts as a radiosensitizing agent in healthy brain tissue.
The patient's sex does not seem to relate to CLL development, but females demonstrated a 4.00 rate ratio of developing a higher number of lesions. This has not been previously described, and the reasons for this finding are unknown. As in previous studies, no relationship was established with tumor location.
Similar to what happens with other RT late adverse effects, CLL seem to develop only in the radiation field.15,17
Association of CLL with Other Late Adverse Effects
Younger age at treatment has a detrimental effect on the development of CLL, LE, microbleeds, and cavernomas.6,8 We hypothesized that there could be an association in the susceptibility to develop these 4 types of injuries.
We demonstrated an association between LE and the development of CLL. In fact, the lesions tend to develop in cerebral locations where LE is worse, and a strong relationship was also found between the development of CLL and the global severity of LE, measured by the Fazekas scale. This finding suggests that the pathophysiologic processes of LE and CLL could be related. Similar to what happens with LE8 and in line with previous studies,9⇓-11 we also demonstrated that infratentorial WM is less susceptible to the development of CLLs.
Nature and Clinical Significance of CLL
The study of Fouladi et al9 described the lesions as cerebral lacunes, in direct analogy to typical adult small ischemic infarcts. Radiation therapy–induced vasculopathy was inferred as the pathophysiologic mechanism.9 As stated, none of the children presented with acute neurologic deficits, the lesions were regular cystic lesions located in the cerebral WM, and some of the lesions demonstrated growth. All these characteristics argue against the possibility of cerebral ischemic lacunes, which are widely described in the scientific literature as irregular lesions without growth, commonly located in the deep gray matter and pons and frequently associated with acute neurologic deficits.9,18,19
Yamasaki et al11 coined the term “cystic malacia” as the final result of WM necrosis. Indeed, the development of cerebral malacia lesions has been described as a later stage of radionecrosis.1,3 However, these lesions are different from CLL, presenting as pseudotumoral masses with contrast enhancement mimicking tumor progression, frequently presenting with clinical manifestations such as seizures or signs of intracranial hypertension.15
None of the patients presented with clinical symptoms that could be related to the location of CLL. All lesions had well-defined, regular margins, oval or rounded, with CSF-isointense MR signal in all sequences, without hemosiderin deposits or gadolinium enhancement (Figs 1 and 2). Most of them evolved in deep and periventricular WM, demonstrated some growth, and subsequently stabilized (Fig 2). Like Kitajima et al,10 we consider these characteristics to be consistent with dilated perivascular spaces.19 Incidentally, some anecdotal reports have reported growing dilated perivascular spaces as late cranial RT effects in the adult population.20 Post-RT pathologic findings such as hyalinization and fibrinoid necrosis of small arteries and arterioles, demyelination, gliosis, or brain atrophy could contribute to the growing dilated perivascular spaces.10,17
There is no reference to cystic lesions in the literature other than as a result of radionecrosis, which, as argued before, does not represent CLL.21 The reason may be the paucity of post-RT pathology studies in the pediatric population or the interpretation of these lesions as enlarged perivascular spaces, unrelated to RT.
The differentiation between therapy toxicity and recurrent disease is sometimes difficult but is critical to therapeutic management and prognosis.3,20 Thus, the knowledge of all late adverse effects of cancer treatment is crucial, including the described CLL. We consider that the clinical significance of these lesions remains unknown and that long-term follow-up and pathologic studies are necessary.
Limitations
There are several limitations to our study, the first being its retrospective nature. This is a 30-year-long cohort, during which different RT and multimodality protocols have been used.6,22 Some of the differences between protocols were not considered, such as the type of irradiation or chemotherapy regimens. Radiation-induced brain injury is probably multifactorial, but the pathophysiology of late CNS radiation cytotoxicity remains unclear.8 We hypothesized that CLL represent dilated perivascular spaces; however, we did not perform histologic analysis of any specimen, so the nature and pathogenesis of these lesions remain unknown.
Pediatric cranial RT is associated with a decline in intelligence quotient, and the most significant cognitive decline happens in patients treated at younger than 5 years of age.5 Specifically, it is known that LE and microbleeds are related to poorer neurocognitive performance.5,8 Cognitive tests were not administered to the studied population; thus, the cognitive impact of CLL remains unknown.
CONCLUSIONS
This study illustrates CLL as a frequent but less studied and under-reported late toxicity of cranial RT in the pediatric population. We demonstrated that CLL developed in the first 4 years after irradiation of the pediatric brain with ≥50 Gy, irrespective of sex, tumor location, and radiation protocol. Particularly, younger children were at higher risk of developing CLL, with a higher lesion count, with a progressive risk reduction for older children and teenagers. Patients who underwent chemotherapy-RT had a 3-fold higher risk of developing CLL. Female patients had a higher risk of developing a higher number of CLL. Postradiation LE was associated with a higher risk of the development of CLL.
Our data reinforce iatrogenic sequelae differing among age groups, even in pediatric patients, suggesting higher radiosensitivity of tissues in younger patients.
RT-induced acute and late effects on normal tissue limit the delivery of therapeutically optimal RT doses for a variety of pediatric and adult cancers; thus, a sound knowledge of all adverse effects is essential.
Footnotes
Disclosures: Joao Passos—UNRELATED: Employment: Clinica de Santo António, Comments: payment related to the provision of services of neurology consultation.
References
- Received January 12, 2021.
- Accepted after revision March 8, 2021.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.